Published on 19/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 5071 times
Ravi Ratnavel
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
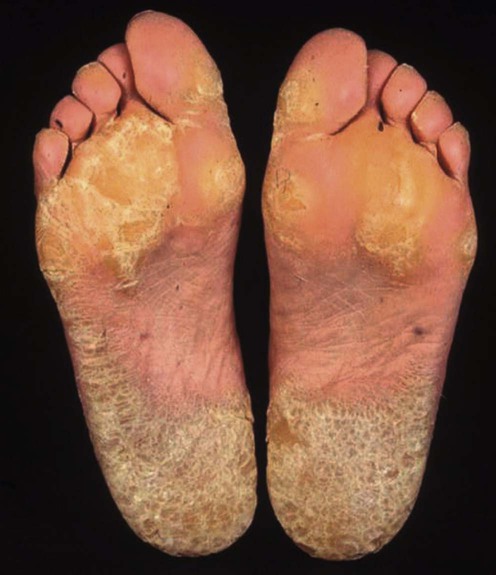
Palmoplantar keratodermas (PPKs) consist of a heterogeneous group of disorders characterized by thickening of the palms and soles. The condition may be subdivided into hereditary keratodermas, acquired forms, and conditions in which PPK is an associated feature of a specific dermatosis.
PPK may be localized to the hands and feet, or develop as part of a more generalized skin disorder. It is important when making a diagnosis to establish its morphology and the presence of any associated ectodermal disease at sites other than the palms and soles. Biopsy may be necessary to distinguish between some hereditary forms of PPK. PPK can be associated with infections (dermatophytes, human papillomavirus, HIV, syphilis, and scabies), drugs (arsenic exposure), and internal malignancy, or may be a cutaneous manifestation of systemic disease (myxedema, diabetes mellitus, or cutaneous T-cell lymphoma). Hyperkeratosis of the palms and soles can also be a feature of eczema, psoriasis, and cutaneous T-cell lymphoma.
The treatment of PPK is difficult. Most therapeutic options produce only short-term improvement and are frequently complicated by unwanted adverse effects. Treatment options range from simple measures such as salt-water soaks with paring and use of topical keratolytics, to systemic retinoids and reconstructive surgery with total excision of the hyperkeratotic skin followed by grafting.
In patients with limited disease, topical keratolytics containing salicylic acid, lactic acid, or urea in a suitable base may be tried. Examples include 5–10% salicylic acid, 10–40% propylene glycol, or 10% lactic acid in aqueous cream or a combination therapy using 10% urea and 5% lactic acid in aqueous cream to be applied twice daily. These formulations can be made up on an individual basis, or the closest proprietary product prescribed. The efficacy of these agents may be increased by occlusion at night. Topical retinoids such as tretinoin (0.01% gel and 0.1% cream) may also be tried; treatment is however often limited by skin irritation. Potent topical corticosteroids, such as clobetasol propionate 0.05%, with or without keratolytics, are occasionally of value in the management of inflammatory PPK. 5-Fluorouracil 5% has produced dramatic results in spiny keratoderma, but its use in other keratodermas has not been evaluated.
The efficacy of the oral retinoids in keratoderma is well established. Good responses have been seen in mal de Meleda, Papillon–Lefèvre syndrome, and erythrokeratoderma variabilis. In some types of PPK, particularly epidermolytic forms, hyperesthesia may limit the usefulness or practicality of treatment with retinoids. The potential risk of bone toxicity should also be assessed in patients on long-term therapy, although the risks are small. Periodic radiologic bone monitoring and, when possible, prescription of pulsed (intermittent) therapy are recommended. The optimal dosage of acitretin is 25–35 mg daily in adults or 0.7 mg/kg daily in children, which may be adjusted after 4 weeks of therapy.
Psoralen plus UVA (PUVA) therapy or re-PUVA (a synergistic combination of oral retinoids and PUVA) may be effective in PPK secondary to psoriasis or eczema. In oculocutaneous tyrosinemia (an autosomal recessive condition characterized by focal palmoplantar keratosis, corneal ulceration, and mental retardation), dietary restriction of phenylalanine and tyrosine has led to resolution of PPK. Oral administration of 1α,25-dihydroxyvitamin D3 and topical calcipotriol ointment has been reported to be effective. Regular podiatry, careful selection of footwear, and treatment of secondary fungal infections is an integral part of management of all PPK. Regular intermittent use of terbinafine cream and other topical antifungals can reduce skin maceration and improve comfort. Surgical or laser dermabrasion is an option for some patients, with potential amelioration of symptoms and improved penetration of topical agents.
For severe refractory PPK excision and skin grafting may be considered. Excision should remove hyperkeratotic skin, including dermis, epidermis, and subcutis, to prevent any risk of recurrence.
Scrapings for mycology
Thyroid function tests
Gamborg Nielson P. Mykosen 1984; 27: 203–10.
In a 5-year survey of dermatophyte infections in Norbotten, Sweden, the frequency of dermatophytosis among patients with hereditary PPK was shown to be 35%, corresponding to a prevalence of 36.7%. The predominant feature of dermatophytosis in patients with hereditary PPK was scaling and fissuring. Treatment improved the clinical signs after 2 to 3 months.
Gamborg Nielson P. Acta Derm Venereol Suppl (Stockh) 1994; 188: 1–60.
In relatives of the original propositi, dermatophytosis was found in 65% of men, 22% of women, and 21% of children, resulting in a total frequency of 36.2%. Statistically, it was proved that Trichophyton mentagrophytes occurred more often in patients with hereditary PPK. Vesicular eruptions along the hyperkeratotic border occurred significantly more often in patients with dermatophytosis and were considered pathognomonic of secondary dermatophytosis.
Hodak E, David M, Feuerman EJ. Acta Derm Venereol 1986; 66: 354–5.
A patient with myxedema and intractable PPK showed improvement after treatment with thyroid replacement therapy. The possibility of a causal relationship between hypothyroidism and PPK was questioned.
Tan OT, Sarkany I. Clin Exp Derm 1977; 2: 287–8.
A patient with myxedema and PPK showed rapid improvement in PPK after thyroxine treatment.
Takayama M, Okuyama R, Sasaki Y, Ohura T, Tagami H, Aiba S. Dermatology 2005; 211: 302.
Aluminum chloride solution was used to reduce plantar sweating, which may exacerbate blistering and hyperkeratosis in this condition.
Gunther SH. Arch Dermatol 1972; 106: 854–7.
Nine patients with PPK were treated with retinoic acid 0.1% in petroleum jelly and all improved within 4 months. Permanent remission ensued in two patients. Recurrence was observed in the majority of cases 8 weeks after the withdrawal of treatment. This was avoided by the topical application of vitamin A acid once or twice weekly.
Touraine R, Revuz J. Acta Derm Venereol Suppl (Stockh) 1975; 74: 152–3.
Six patients were treated for 2 months with either tretinoin 0.1% lotion or 0.05% cream. Improvement was seen in most patients. Better results were achieved with the use of occlusive dressings, mechanical paring prior to topical application, and when a higher concentration of topical tretinoin was used (0.3%).
Bergfeld WF, Derbes VJ, Elias PM, Frost P, Greer KE, Shupack JL. J Am Acad Dermatol 1982; 6: 727–31.
Five of six patients with PPK were safely and effectively treated with isotretinoin, with dramatic clearing of the keratoderma within the first 4 weeks of therapy. The mean dose was 1.95 mg/kg daily, and mean duration of therapy was 113 days.
Blanchet-Bardon C, Nazzaro VV, Rognin C, Geiger JM, Puissant A, et al. J Am Acad Dermatol 1991; 24: 983–6.
An open, non-comparative study to evaluate the clinical response to acitretin in patients with non-psoriatic disorders of keratinization, and to establish the optimal dosage for efficacy and tolerance. Thirty-three patients with ichthyoses, PPK, or Darier disease were treated for 4 months. Most showed a marked improvement. The optimal acitretin dosage providing the best efficacy with minimal side effects varied from patient to patient. The mean daily dose (± SD) was 27 ± 11 mg in adults and 0.7 ± 0.2 mg/kg in children.
Capella GL, Fracchiolla C, Frigerio E, Altomare G. J Dermatolog Treat 2004; 15: 88–93.
A single-blind, matched-sample investigation was carried out in 42 patients with chronic hyperkeratotic palmoplantar dermatitis, who were administered acitretin 25–50 mg daily for 1 month controlled versus a conventional topical treatment (betamethasone/salicylic acid ointment). Acitretin was significantly better than the conventional treatment after 30 days (two-sided, p<0.0001). The authors suggested that acitretin should be considered a first-choice treatment.
Van de Kerkhof PC, Dooren-Greebe RJ, Steijlen PM. Br J Dermatol 1992; 127: 191–2.
Two patients with mal de Meleda treated with acitretin experienced a marked reduction of PPK. The optimal dosage was found to be 10–30 mg daily. Higher dosages resulted in hyperesthesia. Discontinuation of acitretin resulted in relapse within days.
Deschamps P, Leroy D, Pedailles S, Mandard JC. Dermatologica 1986; 172: 258–62.
Etretinate 0.7–0.8 mg/kg daily brought about partial or total remission of hyperkeratosis in 10 cases of keratoderma climactericum.
Wereide K. Acta Derm Venereol 1984; 64: 556–9.
Three patients with mutilating keratodermas were successfully treated with oral etretinate. All had constriction of one or more digits, with impending pseudoamputation. Treatment resulted in disappearance of the pseudo-ainhum and normalization of the digital blood circulation.
It is assumed that acitretin would provide a similar outcome.
Farina R. Aesthet Plast Surg 1987; 11: 249–53.
Five cases of PPK were treated successfully by grafting skin taken from the calves and thighs.
Bédard MS, Powell J, Laberge L, Allard-Dansereau C, Bortoluzzi P, Marcoux D. Pediatr Dermatol 2008; 25: 223–9.
A 6- and 10-year follow-up of successful surgical correction of mutilating keratoderma.
Pisoh T, Bhatia A, Oberlin C. J Hand Surg [Br] 1995; 20: 338–41.
Successful surgical correction of constricting rings in a patient with Vohwinkel syndrome.
Peled IJ, Weinrauch L, Cohen HA, Wexler MK. J Dermatol Surg Oncol 1981; 7: 142–3.
A patient with Papillon–Lefèvre syndrome underwent successful surgical correction of hyperkeratosis of the palms.
Lucker GP, Van de Kerkhof PC, Steijlen PM. Br J Dermatol 1994; 130: 543–5.
A patient with hereditary epidermolytic PPK of Vorner was successfully treated with topical calcipotriol.
Kragballe K, Steijlen PM, Ibsen HH, van de Kerkhof PC, Esmann J, Sorensen LH, et al. Arch Dermatol 1995; 131: 556–60.
Twenty patients with PPK showed no therapeutic benefit with topical calcipotriol.
Katayama H, Yamane Y. Arch Dermatol 1989; 125: 1713.
A patient with acquired PPK was successfully treated with oral 1α,25-dihydroxyvitamin D, 0.5 µg daily for 3 months, with no side effects.
Mobacken H, Rosen K, Swanbeck G. Br J Dermatol 1983; 109: 205–8.
PUVA was found to be effective in five patients with chronic hyperkeratotic dermatitis of the palms.
Daoud MS, Randle HW, Yarborough JM. Dermatol Surg 1995; 21: 243–4.
A patient with acquired PPK treated with dermabrasion and then 2% crude coal tar and 5% salicylic acid in petrolatum showed no evidence of recurrence after 6 months. The indications for dermabrasion include dry, fissured hyperkeratotic heels, psoriatic keratoderma before PUVA therapy, punctate keratoderma, and generalized keratoderma.
Babaev OG, Bashilov VP, Zakharov AK. Khirurgiia (Mosk) 1993; 4: 74–9.
Five hundred and two patients with limited hyperkeratosis were treated, with a favorable clinical effect. Recurrences were noted in only 4% of cases
Ney D, Bay C, Scheider JA, Kelts D, Nyhan WL. Am J Dis Child 1983; 137: 995–1000.
An 11-year-old girl with oculocutaneous tyrosinemia with plantar keratosis and keratitis demonstrated resolution of her keratitis and improvement of her plantar keratosis with dietary restriction of phenylalanine and tyrosine to less than 100 mg/kg.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us



 Topical keratolytics
Topical keratolytics Topical retinoids
Topical retinoids Systemic retinoids
Systemic retinoids Reconstructive surgery with total excision of hyperkeratotic skin followed by grafting
Reconstructive surgery with total excision of hyperkeratotic skin followed by grafting Topical calcipotriol
Topical calcipotriol Oral vitamin D3 analogs
Oral vitamin D3 analogs Topical corticosteroids with or without keratolytics
Topical corticosteroids with or without keratolytics PUVA or re-PUVA
PUVA or re-PUVA Dermabrasion
Dermabrasion CO2 laser
CO2 laser 5-Fluorouracil
5-Fluorouracil Tyrosine-restricted diet in oculocutaneous keratoderma
Tyrosine-restricted diet in oculocutaneous keratoderma