Oxygen transport
The amount of O2 delivered to tissues is equal to the amount contained in the blood (the arterial O2 content) times the cardiac output (CO): CO = stroke volume × the heart rate (Figure 21-1). The arterial O2 content is a product of the hemoglobin (Hb) concentration in grams per deciliter times the amount of O2 in each gram of Hb times the O2 saturation, expressed as a fraction, usually given as 1.39 mL of O2 for every gram of Hb. The affinity of Hb for O2 (Figure 21-1) determines the characteristics of the oxyhemoglobin (HbO2) dissociation curve, with pH, temperature, and concentration of 2,3-diphosphoglycerate (2,3-DPG) having the greatest impact on the affinity of Hb for O2. Five variables affect O2 delivery: (1) Hb concentration, (2) Hb affinity for O2 (P50), (3) percent O2 saturation of Hb (SaO2), (4) CO, and (5) the amount of O2 dissolved in blood (usually trivial amounts).
< ?xml:namespace prefix = "mml" />

For example, if Hb is 15 g/dL, SaO2 is 100%, and PaO2 is 100 mm Hg, then

 ) to the tissues is the product of CO and Ca
) to the tissues is the product of CO and Ca is
is



 )O2, usually achieved by increasing tissue O2 extraction. Conversely, if
)O2, usually achieved by increasing tissue O2 extraction. Conversely, if 
 )O2, or both CO and C(a −
)O2, or both CO and C(a −  )O2 must increase.
)O2 must increase.The oxyhemoglobin dissociation curve
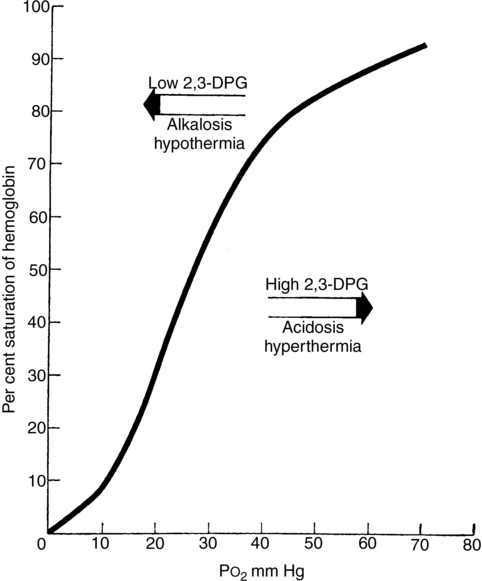
The HbO2 dissociation curve is the measured relationship between PO2 and SO2 (see Figure 21-1). The position of this curve is best described by the position at which Hb is 50% saturated, which is normally 26.7 mm Hg in adult humans. Shifting this curve to the left or right has little effect on SO2 greater than 90%, at which point the curve is relatively horizontal; a much greater effect is seen for values in the steeper parts of the curve (SO2 < 90%).
Variables shifting the HbO2 dissociation curve are listed in Table 21-1. A left-shifted HbO2 dissociation curve indicates a higher affinity of Hb for O2 and, thus, a higher saturation at a given PaO2 (e.g., fetal hemoglobin). This increased affinity of Hb for O2 may require higher tissue perfusion to produce the same O2 unloading. Note that banked blood is markedly depleted of 2,3-DPG within 1 to 2 weeks, which can affect O2 delivery after massive transfusion.
Table 21-1
Variables That Shift the Oxyhemoglobin Dissociation Curve
| Left | Right |
| Alkalosis | Acidosis |
| Hypothermia | Hyperthermia |
| Decreased 2,3-diphosphoglycerate | Increased 2,3-diphosphoglycerate |
| Abnormal hemoglobin (fetal) | Abnormal hemoglobin |
| Carboxyhemoglobin | Increased CO2 |
| Methemoglobin |




