FIG. 7.6 Caldwell-Luc operation. (From Ignatavicius DD, Workman ML: Medical surgical nursing: critical thinking for collaborative care, ed 5, St Louis, 2006, Mosby.)
Go ahead and use the template available on the Evolve Resources site to map the remaining procedures:
• Tympanoplasty
• Mastoidectomy
• Stapedectomy
• Cochlear implant
Nasal Procedures
Procedures
• Septoplasty
• Turbinectomy
• Nasal polypectomy
• Choanal atresia repair
• FESS (functional endoscopic sinus surgery)
• Caldwell-Luc antrostomy (a.k.a. nasal antrostomy; Fig. 7.6)
• Rhinoplasty
Additional Facts to Remember
• Cocaine 4% is used as a topical anesthetic; it also acts as a vasoconstrictor.
• Any surgery performed through the nose is considered nonsterile, with a wound classification of class III (contaminated).
• Repair of choanal atresia (congenital absence of an opening into the nasopharynx) is performed in pediatric patients. The condition is usually suspected if an 8F catheter cannot be inserted where the opening should be. A powered burr or microdebrider is used to make the repair.
• In Caldwell-Luc antrostomy, the incision is made above the canine and second molar.
• It is important to identify and avoid damaging the infraorbital nerve, which could result in blindness or infraorbital neuralgia, a painful disorder that may be misdiagnosed as migraine.
• Absorbable sutures are used in these procedures.
Mapping
Ready to map the remaining procedures? They are:
• Septoplasty
• Turbinectomy
• Polypectomy
• Choanal atresia repair
• Caldwell-Luc antrostomy (a.k.a. nasal antrostomy)
Use the template available on the Evolve Resources site.
Throat Surgeries
Procedures
• Tonsillectomy
• Laryngectomy
• Adenoidectomy
• UPPP (uvulopalatopharyngoplasty)
• Radical neck dissection with mandibulectomy (removal of mandible) or glossectomy (removal of tongue)
• Tracheostomy/tracheotomy
• TMJ (temporomandibular joint) arthroscopy
• Parotidectomy (Fig. 7.7)
• Thyroidectomy
Additional ENT Facts to Remember
• Tonsillectomy/adenoidectomy is performed in conjunction with UPPP if the tonsils or adenoids are hypertrophied.
• UPPP is performed to treat obstructive sleep apnea; it is reasoned that removal of this tissue will widen the patient’s airway, making breathing easier.
• Radical neck dissection is mainly performed to treat metastatic squamous cell carcinoma. Mandibulectomy and tracheostomy are performed in conjunction with this procedure. Two setups and two teams are required: one for radical neck dissection (sterile part, class I [clean]) and the other for oromaxillofacial surgery (nonsterile part, class III [dirty]). Most cases of radical neck dissection involve a combination of glossectomy and mandibulectomy.
• TMJ arthroscopy is similar in concept to any other arthroscopic procedure (discussed later in chapter). Lactated Ringer solution is used for irrigation. Wound classification is class I (clean).
• During parotidectomy, it is important to identify and avoid injuring the facial nerve (cranial nerve VII). This nerve controls facial expression; injury results in facial nerve palsy.
• Use of a harmonic scalpel is preferred for removal of a diseased thyroid gland because it is as safe as conventional methods of hemostasis and quicker because the need for repetitive “clip, cut, tie” routines is eliminated.
• A handheld Green loop retractor and Weitlaner clamp are part of the normal instrument tray for this procedure.
• A transverse incision following the Langer line is performed in radical neck dissection.
• The superior and recurrent laryngeal nerves are important surgical landmarks to be preserved during throat surgeries. They innervate the vocal cord.
• For blunt dissection in throat surgery, cotton peanuts (Kitners) are used.
• The superior thyroid artery is double-clamped, divided, and ligated.
Mapping
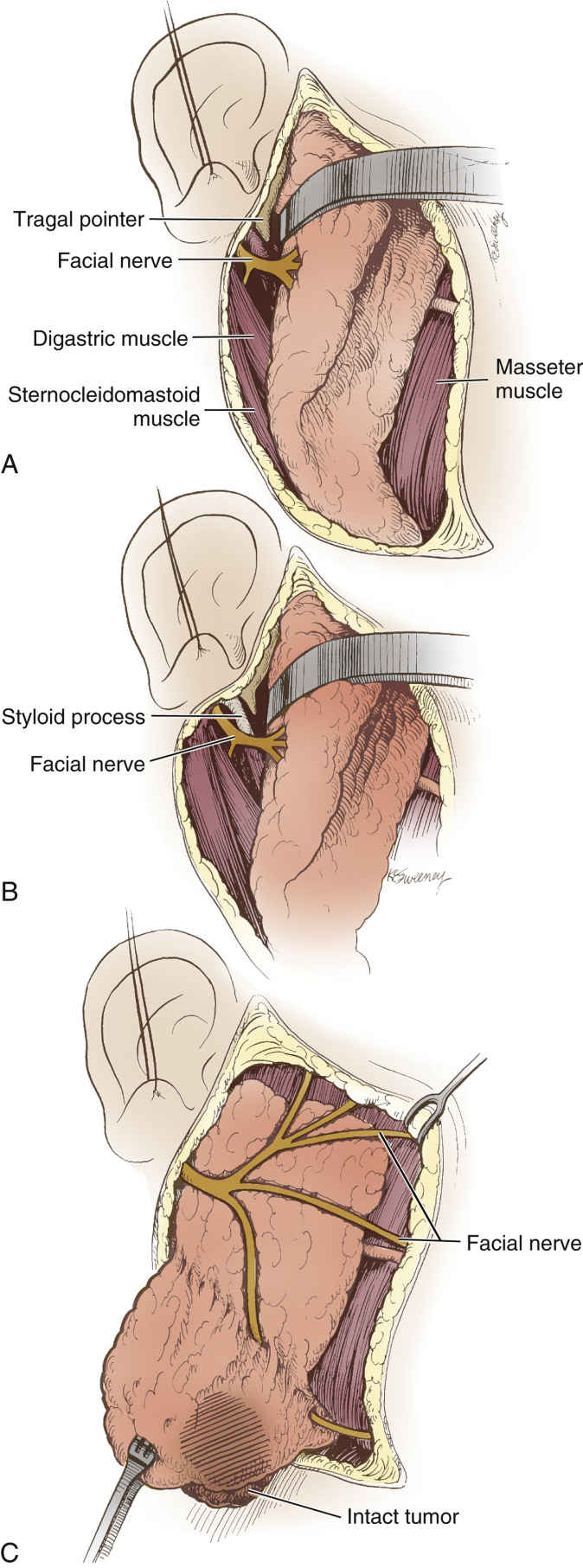
FIG. 7.7 Parotidectomy. Operative technique for parotidectomy. A, Blunt dissection of parotid gland from external auditory canal cartilage exposes tragal pointer. Facial nerve lies approximately 1 cm deep and slightly anteroinferior to pointer and 6 to 8 mm deep to tympanomastoid suture line. B,Facial nerve exits stylomastoid foramen to run anteriorly between styloid process and attachment of digastric muscle to digastric ridge. C, Nearly completed process with tumor within intact superficial parotidectomy specimen. (From Cummings CW et al: Otolaryngology: head and neck surgery, ed 3, St Louis, 1993, Mosby.)
OK, it’s your turn! Use the template available on the Evolve Resources site to map the remaining procedures:
• UPPP (uvulopalatopharyngoplasty)
• Radical neck dissection with mandibulectomy or glossectomy
• Tracheostomy/tracheotomy
• TMJ (temporomandibular joint) arthroscopy
• Parotidectomy






