But focal sinusoidal or periportal fibrosis can be seen
• Inflammation is absent
Bile ducts and hepatic arterioles are normal
Top Differential Diagnoses
• Cirrhosis
• Focal nodular hyperplasia
• Adenomatosis
• Partial nodular transformation
Diagnostic Checklist
• Reticulin stain should be obtained in all cases of unexplained portal hypertension
Ill-Defined Nodules Nodular regenerative hyperplasia (NRH) is characterized by diffuse replacement of liver by small nodules . Nodules are typically 1-3 mm in size but can be as large as 1 cm.
Reticulin Stain Reticulin stain highlights the nodules . The reticulin network is compressed in the parenchyma between the nodules . Reticulin stain is very useful for the diagnosis as the nodularity in NRH can be subtle.
Trichrome Stain Trichrome stain highlights the nodules . By definition, there are no fibrous septa between the nodules in nodular regenerative hyperplasia.
No Fibrous Septa Trichrome stain shows absence of fibrous septa at the periphery of the nodules. This distinguished NRH from cirrhosis. Focal sinusoidal dilatation can be seen in NRH . The hepatocytes between the nodules are compressed and atrophic .
TERMINOLOGY
Abbreviations
• Nodular regenerative hyperplasia (NRH)
Definitions
• Pattern of liver injury, associated with many underlying causes, that does not represent specific entity
Formation of nodules with minimal or no fibrosis
Believed to be related to ischemic atrophy with secondary nodular hyperplasia in areas with good blood flow
ETIOLOGY/PATHOGENESIS
Mechanism
• Results from changes in hepatic blood flow resulting from obliteration of small portal vein radicles
• Obliterative changes in some portal vein radicles lead to localized areas of decreased blood flow and atrophy
• Portal hypertension results from obliterative portal venopathy or sinusoidal compression by nodules
CLINICAL ISSUES
Presentation
• More prevalent in elderly population but can occur in children
• Underlying disease is often clinically evident long before NRH becomes symptomatic
• Symptomatic NRH manifests as portal hypertension and its sequelae: Variceal bleeding, ascites, and splenomegaly
• NRH should always be considered in the setting of portal hypertension without cirrhosis
Laboratory Tests
• Liver transaminases and serum bilirubin levels usually normal; alkaline phosphatase elevated in 25% of cases
Treatment
• Identification and treatment of underlying etiology
• Portosystemic shunt for portal hypertension
IMAGING
Radiographic Findings
• Imaging can be normal or show diffuse nodularity mimicking cirrhosis
MACROSCOPIC
General Features
• Diffuse replacement of liver parenchyma by small nodules
Most nodules are 1-3 mm but can be larger
MICROSCOPIC
Histologic Features
• Diagnosis may be difficult in small biopsies
• Vague, ill-defined, diffuse parenchymal nodules
Hepatocytes in nodule arranged in plates that are 1-2 cells thick
Hepatocytes between nodules are small and atrophic; often compressed into thin, parallel plates
– Variation in hepatocytes within and between nodules is best demonstrated on reticulin stain
Regenerative features (large nuclei, binucleation) may be seen
• Sinusoidal dilation in areas of hepatocellular atrophy
• There are no fibrous septa between the nodules, but focal sinusoidal or periportal fibrosis can be seen
• Occlusion of small portal vein radicals occlusion can occur; larger portal veins are generally normal
• Inflammation is absent; bile ducts and hepatic arterioles are normal
DIFFERENTIAL DIAGNOSIS
Cirrhosis
• Fibrous septa around nodules distinguishes cirrhosis from NRH
Focal Nodular Hyperplasia
• Usually solitary, < 5 cm
• Central scar and fibrous septa with aberrant arterioles and ductular reaction
Adenomatosis
• Varying sized nodules, typically larger than nodules in NRH (several cm)
• Multiple lesions but generally do not involve liver diffusely and uniformly
Partial Nodular Transformation
• Single or multiple nodules at or close to hepatic hilum
• Size of nodules larger than nodules in NRH (3-5 cm)
DIAGNOSTIC CHECKLIST
Pathologic Interpretation Pearls
• Reticulin stain should be obtained in all cases of unexplained portal hypertension


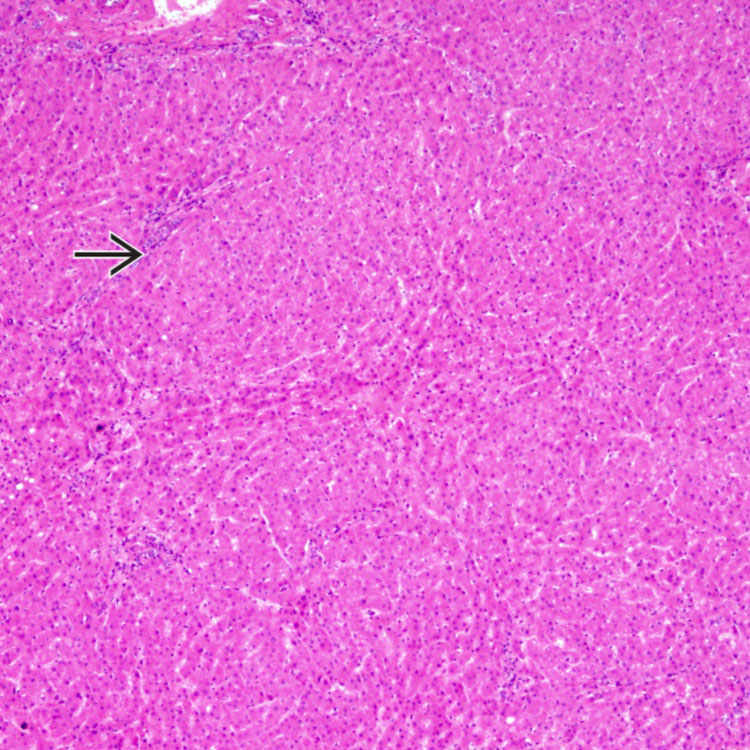
 . Nodules are typically 1-3 mm in size but can be as large as 1 cm.
. Nodules are typically 1-3 mm in size but can be as large as 1 cm.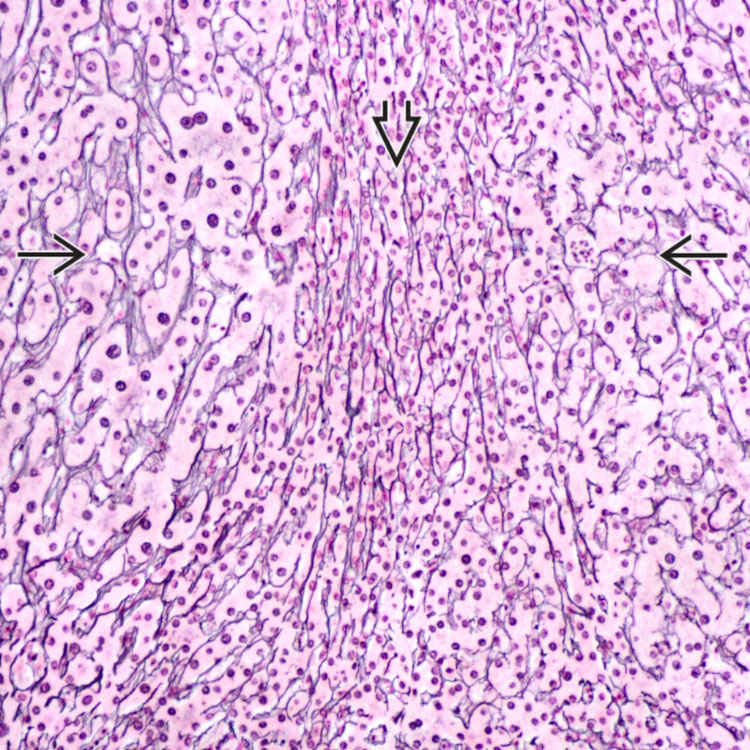
 . The reticulin network is compressed in the parenchyma between the nodules
. The reticulin network is compressed in the parenchyma between the nodules  . Reticulin stain is very useful for the diagnosis as the nodularity in NRH can be subtle.
. Reticulin stain is very useful for the diagnosis as the nodularity in NRH can be subtle.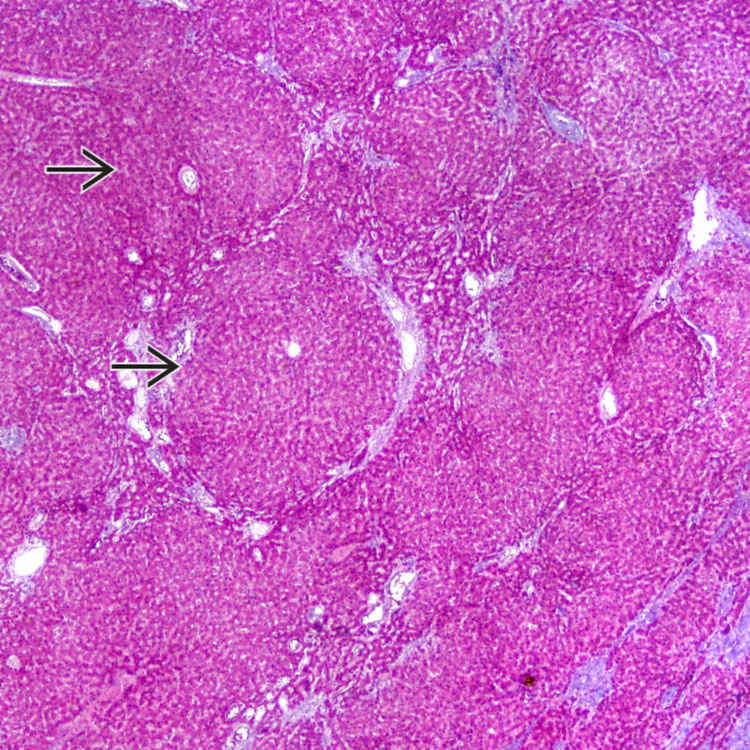
 . By definition, there are no fibrous septa between the nodules in nodular regenerative hyperplasia.
. By definition, there are no fibrous septa between the nodules in nodular regenerative hyperplasia.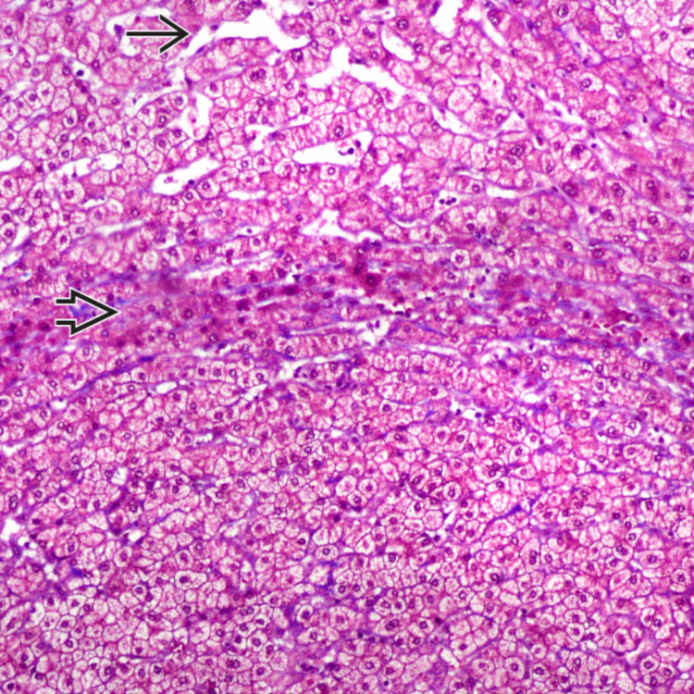
 . The hepatocytes between the nodules are compressed and atrophic
. The hepatocytes between the nodules are compressed and atrophic  .
.