Neural tumors

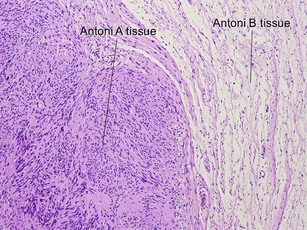
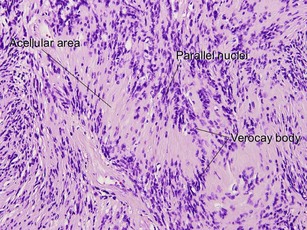
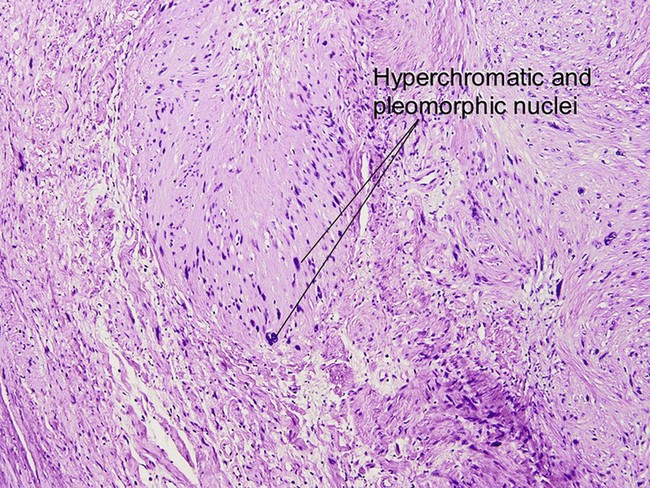
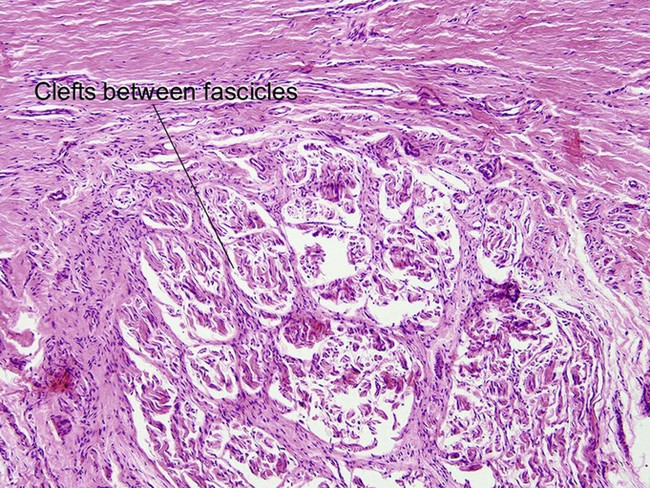
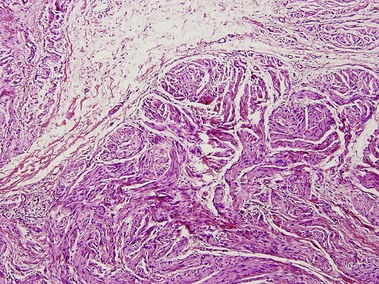
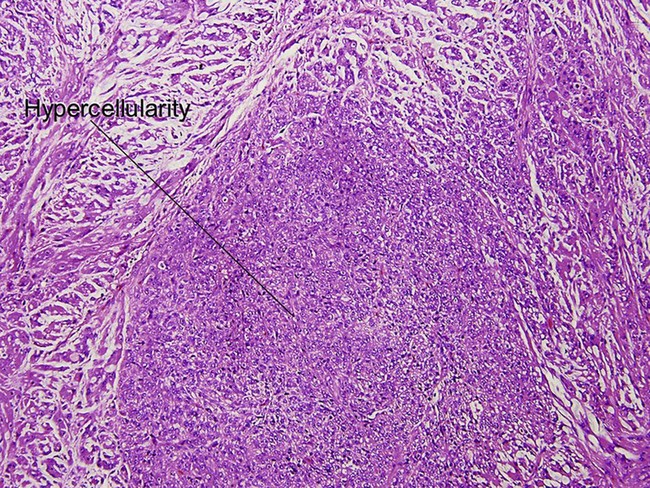
Schwannoma (neurilemmoma)
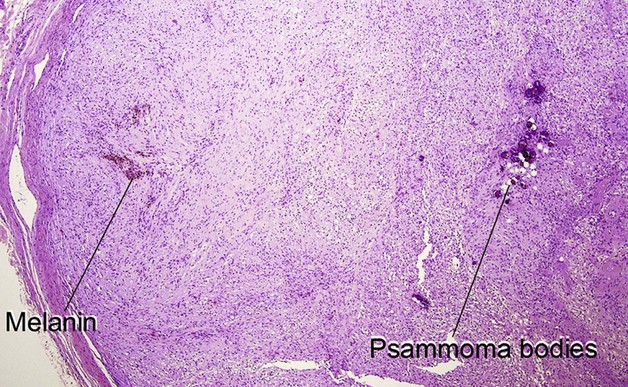
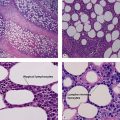
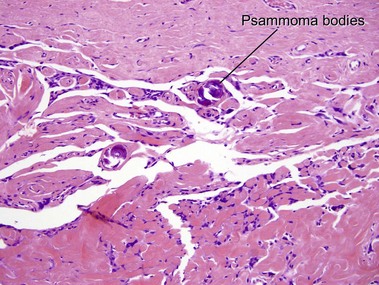
Psammomatous melanotic schwannoma is a variant with psammoma bodies and melanin. It is associated with Carney’s complex (myxomas, spotty pigmentation, and endocrinopathy).
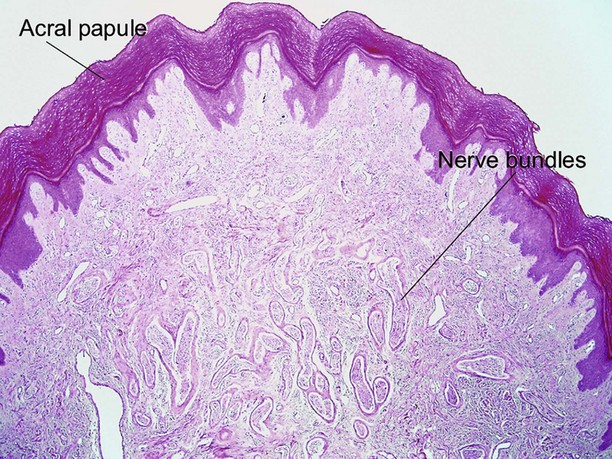
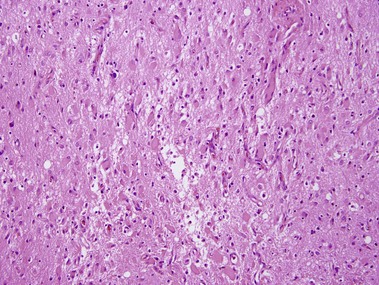
Neuromas
Neuromas are nerve sheath tumors with a roughly 1 : 1 ratio of axons to Schwann cells.


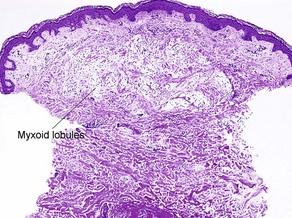
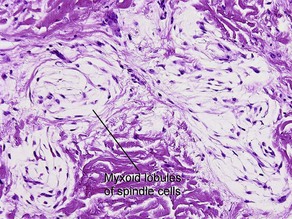
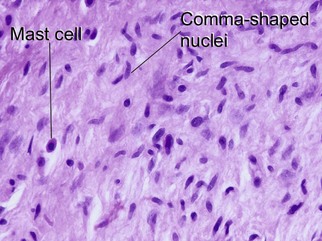
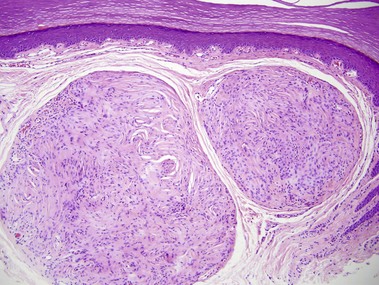
Neurothekeoma
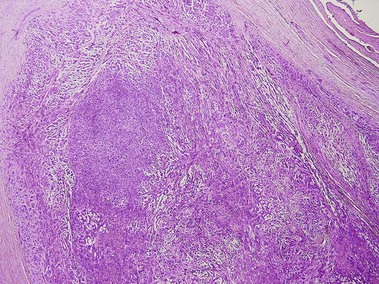
Cellular neurothekeoma
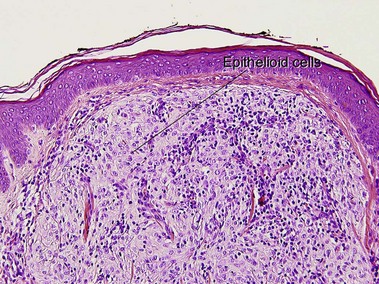
The cellular variant is negative for S100 and desmin, but sometimes positive for smooth muscle actin, neuron-specific enolase, and factor XIIIa. It is frequently positive for NK1/C-3, S100A6, and PGP9.5 with antigen retrieval. S100A6 also stains histiocytic tumors, including atypical fibroxanthoma, as well as Spitz nevi.
Malignant peripheral nerve sheath tumor (MPNST) (neurofibrosarcoma, malignant schwannoma)

Argenyi, ZB. Cutaneous neural heterotopias and related tumors relevant for the dermatopathologist. Semin Diagn Pathol. 1996; 13(1):60–71.
Argenyi, ZB, Balogh, K, Abraham, AA. Degenerative (“ancient”) changes in benign cutaneous schwannoma. A light microscopic, histochemical and immunohistochemical study. J Cutan Pathol. 1993; 20(2):148–153.
Argenyi, ZB, Kutzner, H, Seaba, MM. Ultrastructural spectrum of cutaneous nerve sheath myxoma/cellular neurothekeoma. J Cutan Pathol. 1995; 22(2):137–145.
Calonje, E, Wilson-Jones, E, Smith, NP, et al. Cellular “neurothekeoma”: an epithelioid variant of pilar leiomyoma? Morphological and immunohistochemical analysis of a series. Histopathology. 1992; 20(5):397–404.
Carney, JA, Stratakis, CA. Epithelioid blue nevus and psammomatous melanotic schwannoma: the unusual pigmented skin tumors of the Carney complex. Semin Diagn Pathol. 1998; 15(3):216–224.
Chambers, PW, Schwinn, CP. Chordoma. A clinicopathologic study of metastasis. Am J Clin Pathol. 1979; 72(5):765–776.
Dewit, L, Albus-Lutter, CE, de Jong, AS, et al. Malignant schwannoma with a rhabdomyoblastic component, a so-called triton tumor. A clinicopathologic study. Cancer. 1986; 58(6):1350–1356.
Ducatman, BS, Scheithauer, BW. Malignant peripheral nerve sheath tumors with divergent differentiation. Cancer. 1984; 54(6):1049–1057.
Kluwe, L, Friedrich, RE, Mautner, VF. Allelic loss of the NF1 gene in NF1-associated plexiform neurofibromas. Cancer Genet Cytogenet. 1999; 113(1):65–69.
Macarenco, RS, Ellinger, F, Oliveira, AM. Perineurioma: a distinctive and underrecognized peripheral nerve sheath neoplasm. Arch Pathol Lab Med. 2007; 131(4):625–636.
Miedema, JR, Zedek, D. Cutaneous meningioma. Arch Pathol Lab Med. 2012; 136(2):208–211.
Wallace, CA, Hallman, JR, Sangueza, OP. Primary cutaneous ganglioneuroma: a report of two cases and literature review. Am J Dermatopathol. 2003; 25(3):239–242.
Wang, AR, May, D, Bourne, P, et al. PGP9. 5: a marker for cellular neurothekeoma. Am J Surg Pathol. 1999; 23(11):1401–1407.