Metastatic tumors and simulators
Breast carcinoma

Breast carcinoma is the most common cause of cutaneous metastatic disease in women. In general, metastases are seen on the chest wall, sometimes as a result of direct extension of the tumor. Various clinical and histologic presentations are possible. Distinct subtypes are discussed below.
Carcinoma en cuirasse
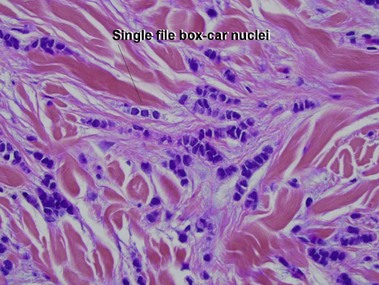
A cuirasse is a suit of armor made of leather. Carcinoma en cuirasse presents with woody induration of the skin. The skin is infiltrated by single files of hyperchromatic nuclei with prominent nuclear molding. Dense collagen is laid down between the tumor cells. Because the dermis is sclerotic, the punch is rectangular rather than tapered.
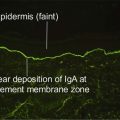
Inflammatory carcinoma (carcinoma erysipeloides)
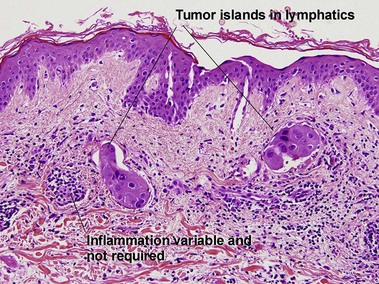
Clinically, the lesions present with skin erythema that ranges from faint macular erythema to an erysipelas-like presentation. Inflammation is usually absent histologically, and the erythema is likely secondary to blood vessel congestion.
Renal carcinoma
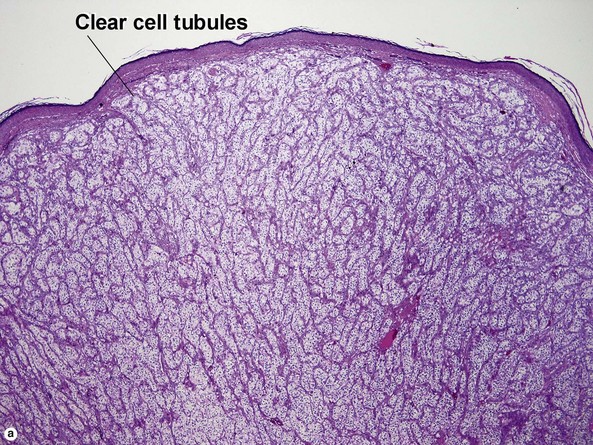
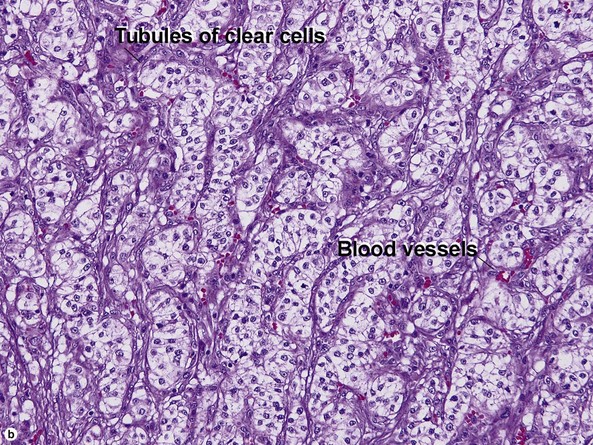
The scalp is a common site for metastatic renal cell carcinoma (RCC). The lesion is typically nodular. The vessels have a “chicken wire” pattern.
Colon carcinoma

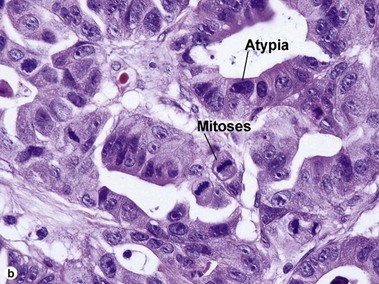
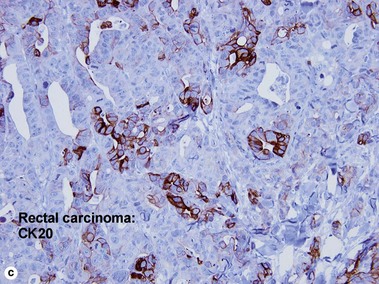
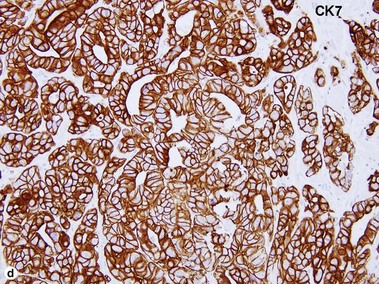
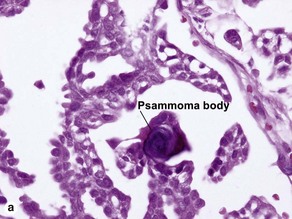
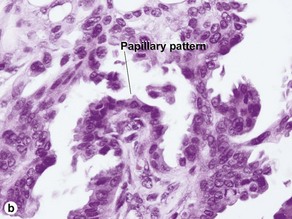
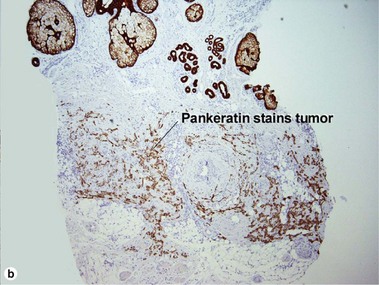
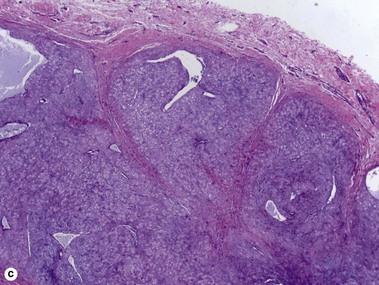
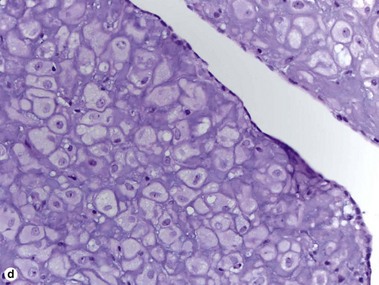
Fig 26.5 (a,b) Colon carcinoma. (c,d) Paradoxical immunostaining pattern in rectal carcinoma (CK20 weak, CK7+). Colon cancer is usually CK20+, CK7−
Colon carcinoma is typically CK20 positive and CK7 negative. Rectal carcinoma may stain with both, or with CK7 only. Figures 26.5c, d demonstrate this paradoxical immunostaining pattern in a rectal adenocarcinoma.
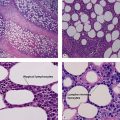
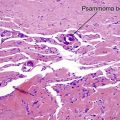
Thyroid carcinoma
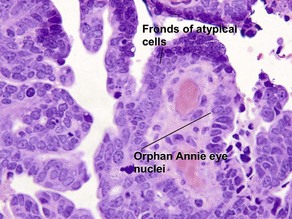
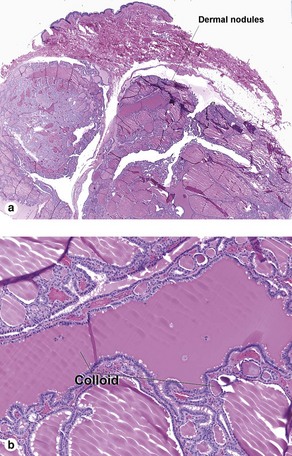
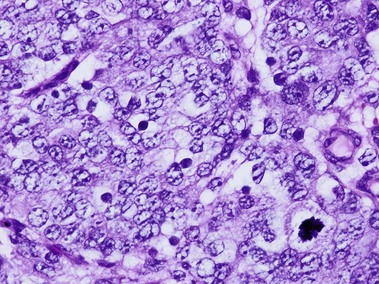
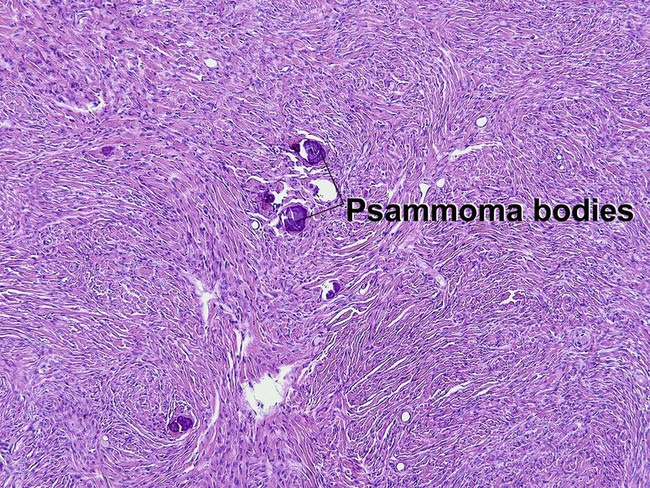
Metastases from the thyroid often spread hematogenously, allowing thyroid carcinoma to present at a variety of body sites. The scalp is a common site. Papillary thyroid carcinoma displays fronds of cells with occasional psammoma bodies and “Orphan Annie” eye nuclei. A follicular variant exists, but retains the characteristic “Orphan Annie” eye nuclei and pseudoinclusions. Follicular thyroid carcinoma is composed of thyroid follicles with colloid. Medullary thyroid carcinomas generally consist of sheets of atypical cells with amyloid; they may be sporadic but occasionally are markers for multiple endocrine neoplasia syndromes IIA (Sipple syndrome) and IIB.
Prostate carcinoma
Metastatic prostate carcinoma generally presents on the thighs/groin area, although it has been reported at other sites.
Metastatic squamous carcinoma
Metastatic squamous cell carcinoma most commonly originates from the oral cavity, lung, or esophagus. Other rare primary sites include the cervix and the male genitalia. Epidermotropic metastases may simulate primary cutaneous squamous cell carcinoma.
Meningioma
The cutaneous presentation of an intracranial meningioma may be secondary to direct extension of the intracranial tumor or true metastatic spread. Lesions are generally seen on the scalp.

Abrol, N, Seth, A, Chattergee, P. Cutaneous metastasis of prostate carcinoma to neck and upper chest. Indian J Pathol Microbiol. 2011; 54(2):394–395.
Marcoval, J, Penín, RM, Llatjós, R, et al. Cutaneous metastasis from lung cancer: retrospective analysis of 30 patients. Australas J Dermatol. 2012; 53(4):288–290.
Relles, D, Fong, Z, Burkhart, R, et al. Facial cutaneous metastasis of colon adenocarcinoma. Am Surg. 2012; 78(11):E454–E456.
Rollins-Raval, M, Chivukula, M, Tseng, GC, et al. An immunohistochemical panel to differentiate metastatic breast carcinoma to skin from primary sweat gland carcinomas with a review of the literature. Arch Pathol Lab Med. 2011; 135(8):975–983.
Somoza, AD, Bui, H, Samaan, S, et al. Cutaneous metastasis as the presenting sign of papillary thyroid carcinoma. J Cutan Pathol. 2013; 40(2):274–278.