58
Nail Disorders
• The nail matrix, which is the growth area, has proximal and distal components (Fig. 58.1).
– The proximal nail matrix forms the top (surface) of the nail plate.
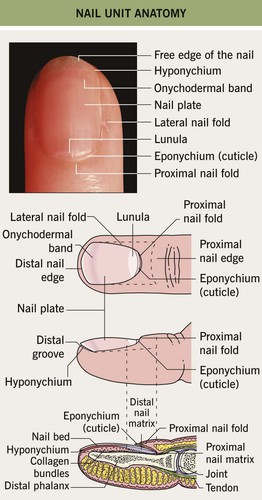
Fig. 58.1 Nail unit anatomy.
• Fingernails grow ~1 mm per month and are replaced every 6 months.
• Toenails grow ~0.5 mm per month and are replaced every 12 months.
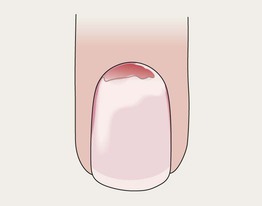
Onycholysis
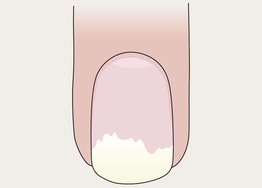

• Distal nail plate detachment, causing nail to look white to yellow-white (Fig. 58.2).
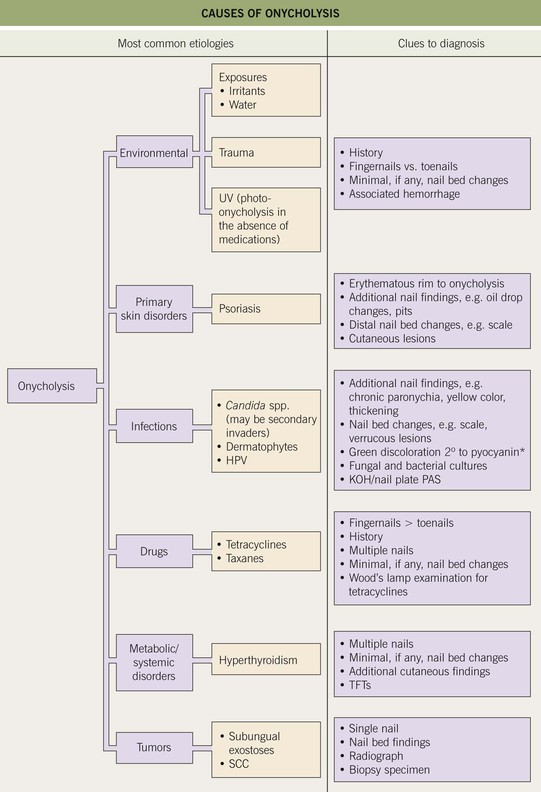
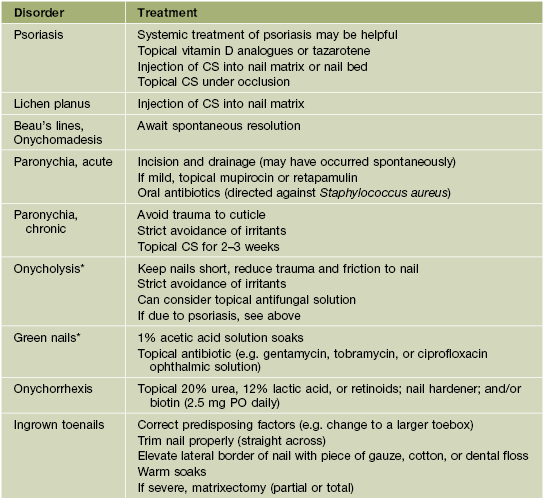
Fig. 58.2 Causes of onycholysis. *Due to secondary colonization with Pseudomonas aeruginosa. SCC, squamous cell carcinoma; TFTs, thyroid function tests.
• Chronic exposure to water and irritants (e.g. soaps) is a common cause.
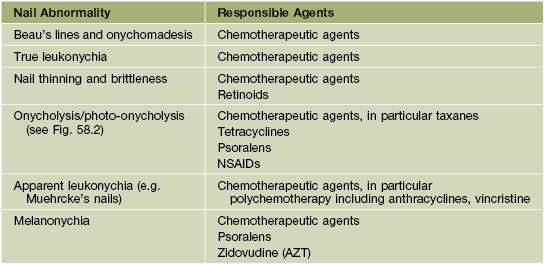
• Associated with psoriasis, onychomycosis, hyperthyroidism, and medications (Table 58.2).

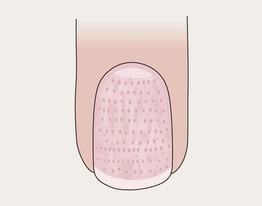
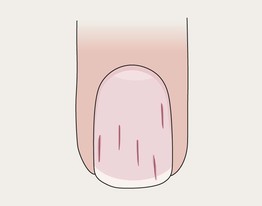
Pitting in Psoriasis


Darier Disease

Trachyonychia

Lichen Planus


True Leukonychia
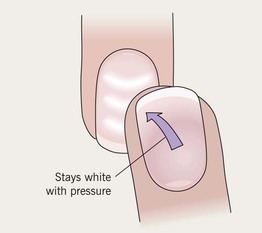
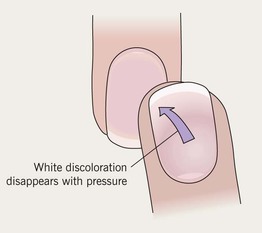
Apparent Leukonychia

Koilonychia

Beau’s Lines

Longitudinal Melanonychia
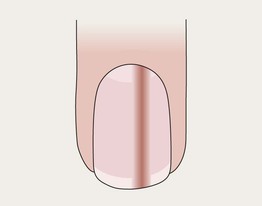

• Longitudinal brown-to-black band.
• Multiple bands common in darker skin types (physiologic); also can be due to trauma (Table 58.3).
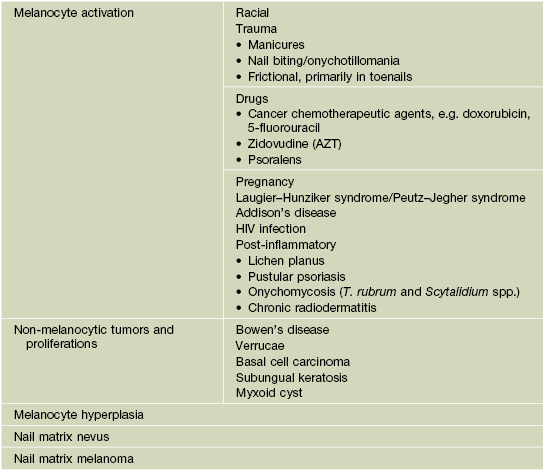
• Single band may be a sign of nail melanoma (Table 58.4).
Table 58.4
ABCDEF rule for clinical suspicion of nail melanoma.
Adapted from Levit EK, et al. The ABC rule for clinical detection of subungual melanoma. J. Am. Acad. Dermatol. 2000;42:269–274.
• When melanoma is suspected, the nail matrix must be biopsied (see Fig. 58.1).
Onychoschizia
Pitting in Alopecia Areata
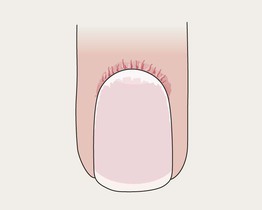
Proximal Nail Fold Telangiectasias
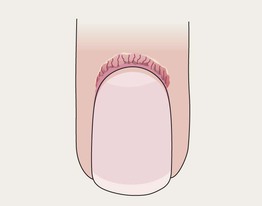
Proximal Nail Fold Telangiectasias with Capillary Dropout

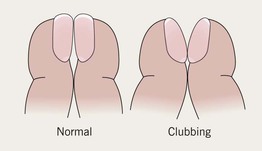
Clubbing
Splinter Hemorrhages
Subungual Hematoma

Green Nail

Paronychia, Acute

Paronychia, Chronic
Pustular Psoriasis
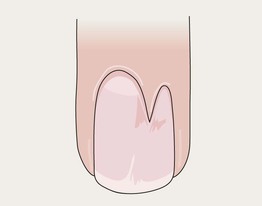
Median Nail Dystrophy (Tic Deformity)

Malalignment
Nail Patella Syndrome

Ingrown Toenails
Onychogryphosis



Yellow Nail Syndrome
Tumors
• Various cysts, hyperplasias, and tumors may be seen on the distal digits, including fibromas (Fig. 58.3), myxoid cysts (Fig. 58.4), pyogenic granuloma (Fig. 58.5), glomus tumor (associated with paroxysmal pain) (see Chapter 94), Bowen’s disease (Fig. 58.6), keratoacanthoma (symptoms include pain, rapid growth), melanoma (signs include longitudinal melanonychia [Fig. 58.7], Hutchinson’s sign = pigmentation of proximal cuticle).

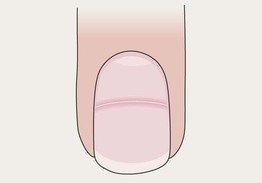
Fig. 58.3 Periungual fibroma producing a longitudinal groove due to matrix compression. Courtesy, Antonella Tosti, MD.

Fig. 58.4 Myxoid cyst. The longitudinal nail groove is a result of the compression of the nail matrix by the cyst (arrow). Courtesy, Antonella Tosti, MD.

Fig. 58.5 Multiple periungual pyogenic granulomas in a patient taking indinavir. Similar lesions can be seen in patients receiving systemic retinoids or epidermal growth factor receptor inhibitors. Courtesy, Antonella Tosti, MD.

Fig. 58.6 Bowen’s disease. The lateral portion of the nail plate is absent. The nail bed shows hyperkeratosis with scaling and fissuring of the epithelium. Courtesy, Antonella Tosti, MD.

For further information see Ch. 71. From Dermatology, Third Edition.
Additional details: onycholysis due to psoriasis; onychomadesis after an episode of acute paronychia; apparent leukonychia represents Muehrcke’s lines; multiple Beau’s lines were due to repeated cycles of systemic chemotherapy; proximal nail fold telangiectasias and ragged cuticles due to dermatomyositis.
Additional courtesies: Antonella Tosti, Julie V Schaffer, and Jean L Bolognia.






