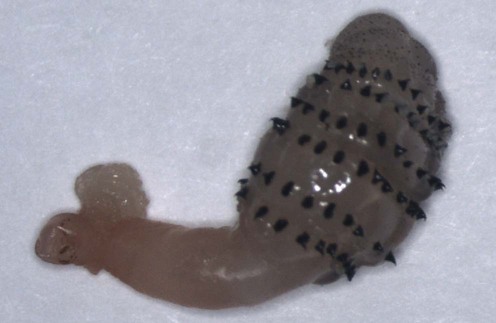
Myiasis





 Detailed travel history
Detailed travel history Morphologic identification of the parasite
Morphologic identification of the parasiteFirst-line therapies
 Local anesthesia with or without surgical incision
Local anesthesia with or without surgical incision Squeezing the skin surrounding the furuncle with fingers or wooden spatulas
Squeezing the skin surrounding the furuncle with fingers or wooden spatulas Vaseline® therapy
Vaseline® therapy Bacon therapy
Bacon therapy Pork fat therapy
Pork fat therapy Hair gel
Hair gel Occlusion with chimo (paste-like smokeless tobacco)
Occlusion with chimo (paste-like smokeless tobacco) Small wad of cotton soaked in sap of the Thevetia ahouai (Apocynaceae) tree
Small wad of cotton soaked in sap of the Thevetia ahouai (Apocynaceae) tree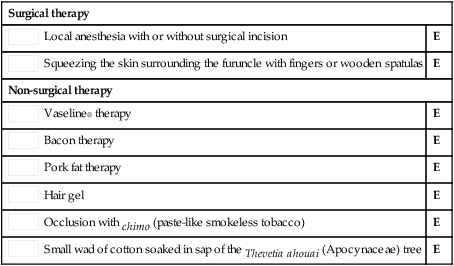
Surgical therapy
Second-line therapies
 Systemic ivermectin
Systemic ivermectin Topical ivermectin
Topical ivermectin Chloroform/ether
Chloroform/ether Ethanol spray
Ethanol spray Oil of betel leaf
Oil of betel leaf Mineral turpentine
Mineral turpentineLarvicidal effects of mineral turpentine, low aromatic white spirits, aqueous extracts of Cassia alata, and aqueous extracts, ethanolic extracts and essential oil of betel leaf (Piper betle) on Chrysomya megacephala.
Kumarasinghe SP, Karunaweera ND, Ihalamulla RL, Arambewela LS. Int J Dermatol 2002; 41: 877–80.

