[level-membership-for-dermatology-category]
Molluscum contagiosum


 Await spontaneous resolution
Await spontaneous resolution Manual extrusion with gloved fingers or fine forceps
Manual extrusion with gloved fingers or fine forcepsSecond-line therapies
 Topical 5% acidified nitrite co-applied with 5% salicylic acid
Topical 5% acidified nitrite co-applied with 5% salicylic acid Topical salicylic acid gel 12%
Topical salicylic acid gel 12% Topical 10% povidone-iodine and 50% salicylic acid
Topical 10% povidone-iodine and 50% salicylic acid Topical 40% silver nitrate paste
Topical 40% silver nitrate paste Topical 0.5% podophyllotoxin
Topical 0.5% podophyllotoxin Cryotherapy
Cryotherapy
Third-line therapies
 Curettage with EMLA cream
Curettage with EMLA cream Pulsed dye laser
Pulsed dye laser Photodynamic therapy
Photodynamic therapy Application of duct tape
Application of duct tape 10% potassium hydroxide solution
10% potassium hydroxide solution Topical 1–5% imiquimod
Topical 1–5% imiquimod Cantharidin
Cantharidin Diphencyprone
Diphencyprone Australian lemon myrtle
Australian lemon myrtle Topical cidofovir
Topical cidofovir Tretinoin
Tretinoin Adapalene
Adapalene Melaleuca alternifolia and iodine
Melaleuca alternifolia and iodine Candida antigen – intralesional
Candida antigen – intralesional Cimetidine
Cimetidine Interferon-α – subcutaneous
Interferon-α – subcutaneous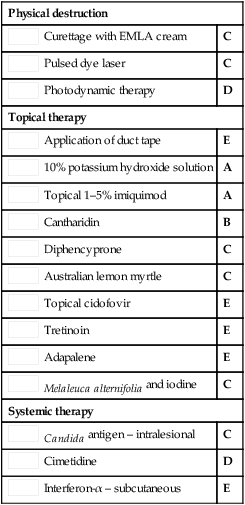
Curettage of molluscum contagiosum in children: analgesia by topical application of a lidocaine/prilocaine cream (EMLA).
Rosdahl L, Edmar B, Gisslen H, Nordin P, Lillieborgs S. Acta Derm Venereol 1988; 68: 149–53.
EMLA cream provided effective local anesthesia for the curettage of MC in 55 children.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Molluscum contagiosum
Second-line therapies
Buy Membership for Dermatology Category to continue reading. Learn more here
[/not-level-membership-for-dermatology-category]
