[level-membership-for-dermatology-category]
Lyme borreliosis

(Courtesy of Daniel Caplivski MD. Mount Sinai School of Medicine, New York, NY.)
Specific investigations
Testing
First-line therapies
| Early localized disease (erythema migrans)* | |
 Doxycycline† 100 mg twice daily for 14 days Doxycycline† 100 mg twice daily for 14 days |
A |
 Amoxicillin 500 mg three times daily for 14 days Amoxicillin 500 mg three times daily for 14 days |
A |
 Cefuroxime axetil 500 mg twice daily for 14 days Cefuroxime axetil 500 mg twice daily for 14 days |
A |
| Early neurological (meningitis or radiculopathy) | |
 Ceftriaxone 2 g IV daily for 14 days Ceftriaxone 2 g IV daily for 14 days |
B |
 Penicillin G 18–24 million units IV daily (divided and dosed every 4 hours) for 14 days Penicillin G 18–24 million units IV daily (divided and dosed every 4 hours) for 14 days |
B |
| Cardiac disease including atrioventricular block | |
 Can be treated with oral or parenteral regimens recommended for early localized or early neurologic disease for 14 days‡ Can be treated with oral or parenteral regimens recommended for early localized or early neurologic disease for 14 days‡ |
C |
| Lyme arthritis without neurologic involvement | |
 Doxycycline† 100 mg twice daily for 14 days Doxycycline† 100 mg twice daily for 14 days |
B |
 Amoxicillin 500 mg three times daily for 14 days Amoxicillin 500 mg three times daily for 14 days |
B |
| Lyme arthritis with neurologic involvement | |
 Ceftriaxone 2 g IV daily for 14–28 days Ceftriaxone 2 g IV daily for 14–28 days |
B |
 Penicillin G 18—24 million units IV daily (divided and dosed every 4 hours) for 14–28 days Penicillin G 18—24 million units IV daily (divided and dosed every 4 hours) for 14–28 days |
B |
| Recurrent arthritis | |
 Re-treatment with a 28-day course of oral antibiotics Re-treatment with a 28-day course of oral antibiotics |
D |
| Late neuroborreliosis | |
 Ceftriaxone 2 g IV daily for 14-28 days Ceftriaxone 2 g IV daily for 14-28 days |
B |
 Penicillin G 18–24 million units IV daily (divided and dosed every 4 hours) for 14–28 days Penicillin G 18–24 million units IV daily (divided and dosed every 4 hours) for 14–28 days |
B |
| Acrodermatitis chronic atrophicans | |
 Doxycycline 100 mg twice daily for 21 days Doxycycline 100 mg twice daily for 21 days |
C |
 Amoxicillin 500 mg three times daily for 21 days Amoxicillin 500 mg three times daily for 21 days |
C |
 Cefuroxime axetil 500 mg twice daily for 21 days Cefuroxime axetil 500 mg twice daily for 21 days |
D |
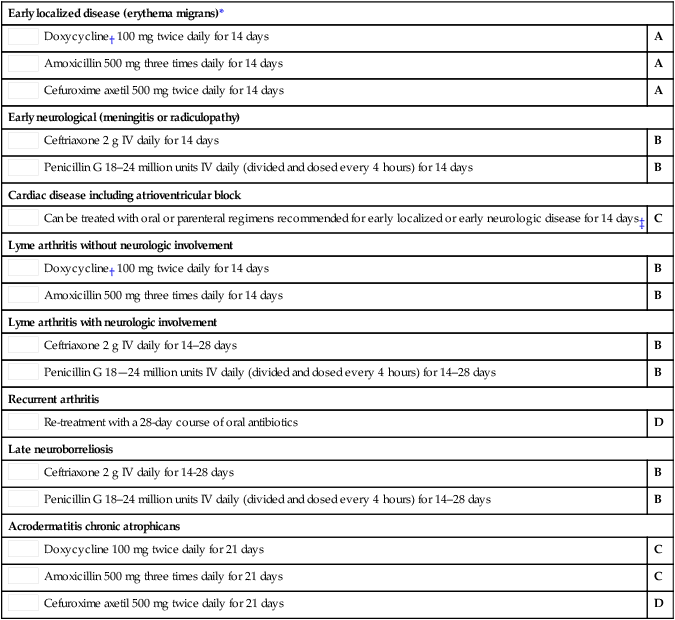
*Level B recommendation for Borrelia Lymphocytoma and early Lyme disease with isolated cranial nerve palsy.
†Doxycycline is contraindicated in pregnancy and in children <8 years old.
‡Initial treatment with parenteral regimen recommended in hospitalized patients.
Second-line therapies
 Erythromycin 250 mg orally four times daily for 14 days
Erythromycin 250 mg orally four times daily for 14 days Azithromycin 500 mg daily for 7 days
Azithromycin 500 mg daily for 7 days Doxycycline 100 mg twice a day for 10–28 days
Doxycycline 100 mg twice a day for 10–28 days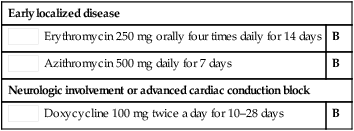
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Lyme borreliosis
(Courtesy of Daniel Caplivski MD. Mount Sinai School of Medicine, New York, NY.)
