9
Lichen Planus and Lichenoid Dermatoses
Lichen Planus
• Flat-topped (lichenoid) papules that are often polygonal in shape and purple in color may coalesce into plaques (Fig. 9.1); lesions usually resolve with hyperpigmentation (Fig. 9.2).
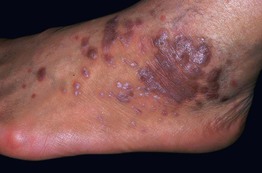
Fig. 9.1 Lichen planus. Violaceous papules and plaques with white scale and Wickham’s striae. Courtesy, Tetsuo Shiohara, MD.

Fig. 9.2 Lichen planus of the dorsal hand. Note the flat-topped nature of the lesions and the post-inflammatory hyperpigmentation. Courtesy, Frank Samarin, MD.
• A characteristic finding is Wickham’s striae, a network of fine white lines on the surface of papules and plaques (Fig. 9.3).

Fig. 9.3 Wickham’s striae in lichen planus. This patient has a hypertrophic lesion in addition to classic lesions. Courtesy, Julie V. Schaffer, MD.
• There are multiple variants of lichen planus, from exanthematous to hypertrophic (Table 9.1; Figs. 9.4 and 9.5).
Table 9.1
Variants of lichen planus.
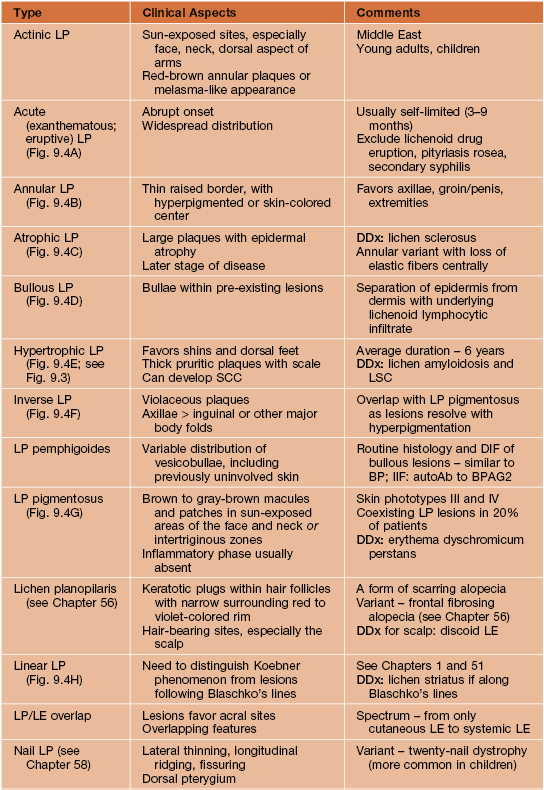
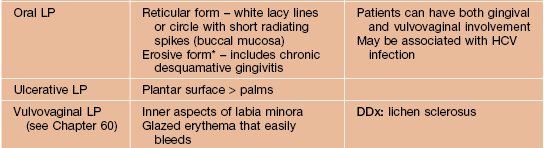
* If erosive variant plus lichenoid cutaneous lesions, DDx includes paraneoplastic pemphigus.
AutoAb, autoantibody; BP, bullous pemphigoid; BPAG2, bullous pemphigoid antigen 2 (type XVII collagen); DIF, direct immunofluorescence; HCV, hepatitis C virus; IIF, indirect immunofluorescence; LE, lupus erythematosus; LSC, lichen simplex chronicus; SCC, squamous cell carcinoma.








Fig. 9.4 Variants of lichen planus. A Exanthematous variant with multiple papulosquamous lesions. B Annular variant with thin elevated rim and central hyperpigmentation. C Atrophic variant with large, long-standing lesions. D Bullous variant with vesicobullae arising in pre-existing plaque. E Hypertrophic variant with thick plaques on the shins, a common location for this variant. F Inverse variant of the axillae; note the purple color. G Pigmentosus variant with only hyperpigmented lesions in an intertriginous zone. H Linear variant along Blaschko’s lines with follicular spines. B, Courtesy, Frank Samarin, MD; C, Courtesy, Tetsuo Shiohara, MD. F, Courtesy, Jeffrey Callen, MD.




Fig. 9.5 Lichen planus of the nails and oral mucosa. A Thinning of the nail plate with lateral loss. B Violaceous discoloration of the periungual area with pterygium formation. C Reticular oral form characterized by a white lacy pattern composed of rings with short radiating spikes; there is also an erosion of the buccal mucosa. D Erosions, lacy pattern, and scarring of the tongue. D, Courtesy, Louis Fragola, MD.
• DDx: lichenoid drug eruption, lupus erythematosus, pityriasis lichenoides chronica, lichen nitidus, GVHD and a lichenoid ‘id’ reaction due to acute contact dermatitis to nickel (children), as well as the entities in the comments section of Table 9.1.
• Rx: topical or intralesional CS, topical calcineurin inhibitors, phototherapy (NBUVB), and if severe, consider systemic therapy (e.g. oral CS, hydroxychloroquine [scalp disease], acitretin).
Lichenoid Drug Eruption
• A drug-induced eruption that has an appearance similar to lichen planus; often more generalized or in a photodistribution (e.g. HCTZ-induced [Fig. 9.6]).

Fig. 9.6 Lichenoid drug eruption in a photodistribution. The patient was taking hydrochlorothiazide (HCTZ).
• Often a latent period of months after instituting drug.
• Lesions tend to be more eczematous, psoriasiform, or pityriasis rosea-like.
Lichen Striatus
• Linear array of small, 2–4 mm, flat-topped (lichenoid) papules whose color ranges from skin-colored to pink to tan (i.e., hypopigmented, especially in darkly pigmented patients) (Fig. 9.7).


Fig. 9.7 Lichen striatus. A Linear array of pink flat-topped papules on the hand in association with splitting and fraying of the lateral aspect of R2 and the medial aspect of R3. B Single streak on the posterior lower extremity composed of multiple pink flat-topped papules. The differential diagnosis would include Blaschkitis and linear lichen planus.
• Lesions appear over several days to weeks along the lines of Blaschko (see Chapter 51) and are usually asymptomatic.
• Acral streaks associated with nail dystrophy (e.g. onycholysis, splitting).
• No consistently identified trigger and mosaicism for a particular gene not detected to date.
Lichen Nitidus
• Multiple, tiny, discrete, flat-topped papules that are uniform in size and usually skin-colored (Fig. 9.8); may occasionally be pink to brown in color or hypopigmented (darkly pigmented individuals).
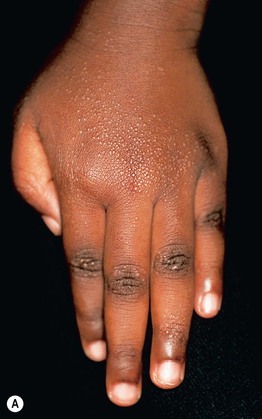

Fig. 9.8 Lichen nitidus. A Numerous tiny flat-topped papules on the hand. B A close-up view shows the shiny surface.
• A linear arrangement of papules may be seen, due to Koebner phenomenon (Table 9.2).
Table 9.2
Clinical entities that commonly display Koebner (isomorphic) phenomenon.
* Sometimes referred to as pseudo-Koebner phenomenon.
• No consistently identified trigger and persists for months to years.
Erythema Dyschromicum Perstans (EDP; Ashy Dermatosis)
• Symmetric distribution of multiple oval-shaped gray to gray-brown macules and patches (0.5–2.5 cm; Fig. 9.9); occasionally, a transient thin peripheral rim of erythema is present.

Fig. 9.9 Erythema dyschromicum perstans. Numerous, oval to polygonal, gray-brown (ashy-colored) macules on the lower extremities. Courtesy, Graham Dermatopathology Library Collection, Wake Forest University.
• Favors neck, trunk, and proximal upper extremities; as in pityriasis rosea, the long axis of lesions often follows skin cleavage lines, i.e. Langer’s lines (see Fig. 7.7).
• No consistently identified trigger.
• Idiopathic eruptive macular pigmentation is often considered to be a variant of EDP.
• Rx: no specific effective therapy; can try sunscreens and mild topical CS.
Keratosis Lichenoides Chronica
• Violaceous keratotic lichenoid papules are arranged in a linear or reticulated pattern (Fig. 9.10); can resemble Chinese characters.

Fig. 9.10 Keratosis lichenoides chronica. Symmetrical distribution of linear and reticulated keratotic plaques admixed with small violaceous lichenoid papules. Courtesy, Kathy Schwarzenberger, MD.
• Tends to be chronic, progressive, and difficult to treat; occasionally responds to phototherapy (NBUVB or PUVA) ± systemic retinoids.
Actinic Lichen Nitidus (Summertime Actinic Lichenoid Eruption)
Annular Lichenoid Dermatitis (of Youth)
• More commonly seen in children and young adults.
• DDx: inflammatory morphea, mycosis fungoides, inflammatory vitiligo, figurate erythemas.
For further information see Ch. 11. From Dermatology, Third Edition.






