[level-membership-for-opthalmology-category]
CHAPTER 14 Irrigation and aspiration
Removal of viscoelastic with I and A following implantation of the IOL is considered, in the modular teaching method, to represent the least risky step in cataract surgery1. For experienced surgeons even cortical I and A may therefore be taken for granted. However, there are still some valuable lessons to be learned from considering the techniques and technology employed.
Anatomical considerations
The target of I/A is the peripheral cortex, the thin layer of soft lens fibers directly apposed to the lens capsule. With the use of cortical cleaving hydrodissection, in which this thin envelope of tissue is separated from the capsule, often the peripheral cortex is loose enough that it can be consumed with the phaco needle as part of the management of the epinucleus. ‘Throw away your I and A!’ became the mantra of early adopters of cortical cleaving hydrodissection. Nevertheless, the I/A is still required, albeit a minority of the time, even with impeccable cortical cleavage2.
Anatomically, the cortex is most adherent to the anterior capsule and equator because lens epithelial cells in these locations form the capsule as their basement membrane. This consideration explains the fundamental technique of I and A, which consists of grasping the exposed anterior fronds of cortex at or just below the level of the capsulorrhexis and stripping them with a combined tangential and centripetal motion. The force applied is counteracted by the zonular apparatus, which holds the capsule firm and allows the cortex to come free. In cases of zonular weakness (e.g. trauma or PXF) a capsular tension ring (CTR) may help insure that the capsule is not aspirated along with the cortex. However, the CTR, which is appropriately placed into the golden ring or cleavage plane between the peripheral cortex and the epinucleus, also traps cortical material against the capsule. A recent modification of the standard CTR by Henderson adds ripples to the structure to permit some wiggle room that facilitates cortical clean-up3.
Bimanual I and A
The development of bimanual or biaxial I and A also alleviates the crisis of subincisional cortex. By creating two identical paracentesis type incisions 60 to 180° apart the surgeon can employ separate irrigation and aspiration cannulae that are completely interchangeable. The additional incision, less than 1.5 mm in diameter, does not measurably alter the corneal astigmatism4, and the added ease and grace of the I/A procedure far outweigh the additional time it takes to make the incision and switch hands.
Recent innovations
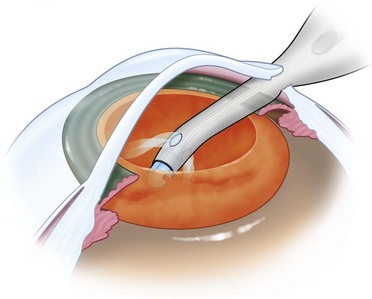
Because many surgeons in the United States in particular have remained resistant to the bimanual approach, manufacturers have focused on improvements in coaxial instrumentation. Barrett has developed one such enhanced coaxial instrument (Fig. 14.1). It is designed to increase irrigation flow for a give bottle height by reducing the lumen of the aspiration tip. Greater inflow augments chamber stability. In addition the coaxial sleeve is designed to eliminate competing irrigation, and aspiration flow at the tip by employing a tighter sleeve. Irrigation fluid flows only from the side ports of the sleeve, not from the end. Finally, the hand piece is designed to permit more maneuverability in the wound, particularly with smaller incisions, to prevent the oar locking that frustrates removal of subincisional cortex. The goals of this design demonstrate an attempt to mitigate the limitations of coaxial systems.
1 Smith JH. Teaching phacoemulsification in US ophthalmology residencies: can the quality be maintained? Curr Opin Ophthalmol. 2005;16(1):27-32.
2 Fine IH. Cortical cleaving hydrodissection. J Cataract Refract Surg. 1992;18(5):508-512.
3 Henderson BA, Kim JY. Modified capsular tension ring for cortical removal after implantation. J Cataract Refract Surg. 2007;33(10):1688-1690.
4 Alió J, Rodríguez-Prats JL, Galal A, et al. Outcomes of microincision cataract surgery versus coaxial phacoemulsification. Ophthalmology. 2005;112(11):1997-2003. Epub 2005 Sep 23
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]
CHAPTER 14 Irrigation and aspiration
Removal of viscoelastic with I and A following implantation of the IOL is considered, in the modular teaching method, to represent the least risky step in cataract surgery1. For experienced surgeons even cortical I and A may therefore be taken for granted. However, there are still some valuable lessons to be learned from considering the techniques and technology employed.
