[level-membership-for-surgery-category]
CHAPTER 4 Inguinal Hernia Repair
INDICATIONS FOR INGUINAL HERNIA REPAIR
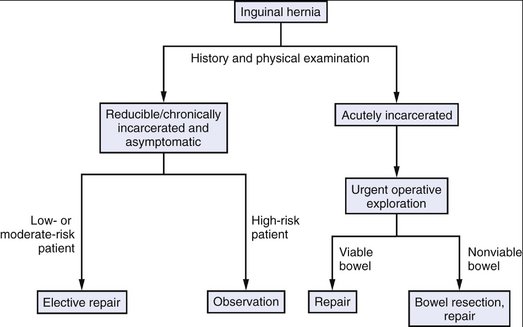
PREOPERATIVE EVALUATION
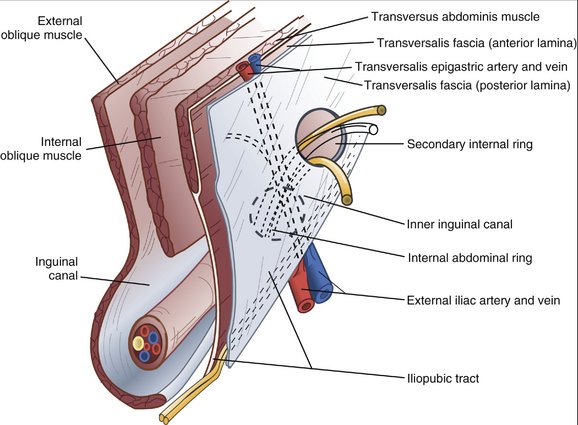
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Preoperative Considerations
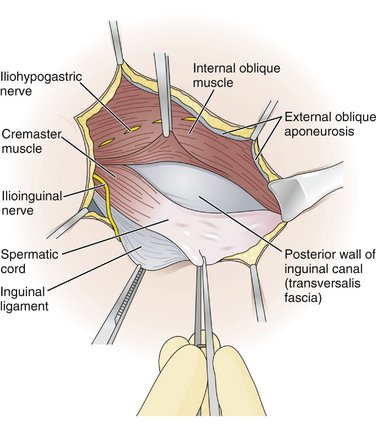
Incision and Exposure
High Ligation of the Hernia Sac
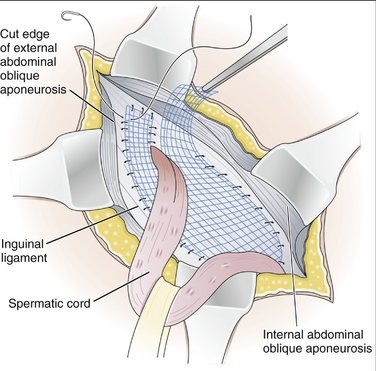
Reconstruction
Closure
Other Approaches
COMPLICATIONS
Eubanks WS. Hernias. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 16th ed. Philadelphia: Saunders; 2001:783-801.
Fitzgibbons RJJr, Giobbie-Hurder A, Gibbs JO, et al. Watchful waiting versus repair of inguinal hernia in minimally symptomatic men. JAMA. 2006;295:285-292.
Malangoni MA, Gagliardi RJ. Hernias. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 17th ed. Philadelphia: Saunders; 2004:1199-1218.
Neumayer L, Giobbie-Hurder A, Jonasson O, et al. Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med. 2004;350:1819-1827.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 4 Inguinal Hernia Repair
INDICATIONS FOR INGUINAL HERNIA REPAIR
PREOPERATIVE EVALUATION
[/not-level-membership-for-surgery-category]
