51 Infections in the Immunocompromised Host
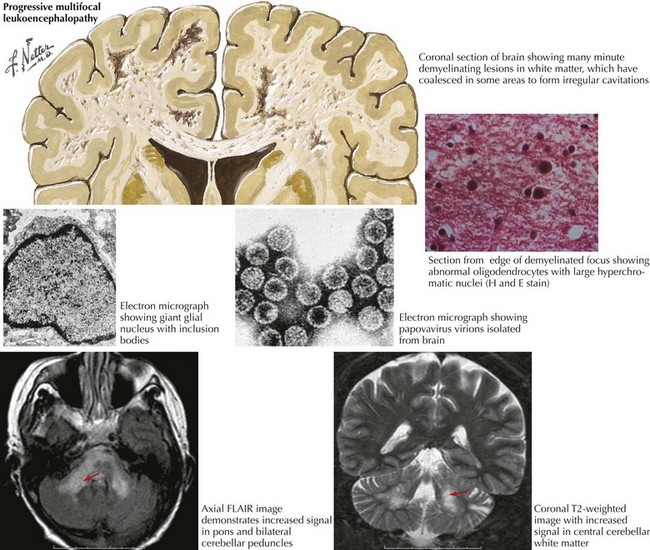
Progressive Multifocal Leukoencephalopathy (Jc Virus)
Epidemiology
PML occurs most commonly in systemic lupus erythematosus among the various rheumatologic disorders.
Clinical Presentation
Lesions may be primarily located in the cerebral white matter or sometimes in the cerebellum and brainstem (Fig. 51-1). Spinal cord involvement is rare but is reported. However, survival remains poor once PML is diagnosed. As there is no specific antiviral medication effective for PML, the main focus should be on prophylactic measures to avoid immunodeficiency.
Diagnosis
A definitive diagnosis of PML requires identification of the characteristic pathologic changes on brain biopsy: multiple asymmetric foci of demyelination at various stages of evolution in the cerebral white matter. The oligodendrocytes demonstrate characteristic cytopathic effects, including nuclear enlargement, loss of normal chromatin pattern, and intranuclear accumulation of deeply basophilic homogenous staining material. Electron microscopy reveals polyomavirus particles in enlarged oligodendrocyte nuclei (see Fig. 51-1).
Clinical Vignette
Epidemiology
This chronic, subacute, and, rarely, acute CNS infection is caused by Cryptococcus neoformans, a yeast-like fungus. Distributed worldwide in soil, fruits, and matter contaminated by pigeon excreta, this organism probably enters the body through the lungs and then disseminates to all organs (Fig. 51-2). Mild, self-limited infections are common.
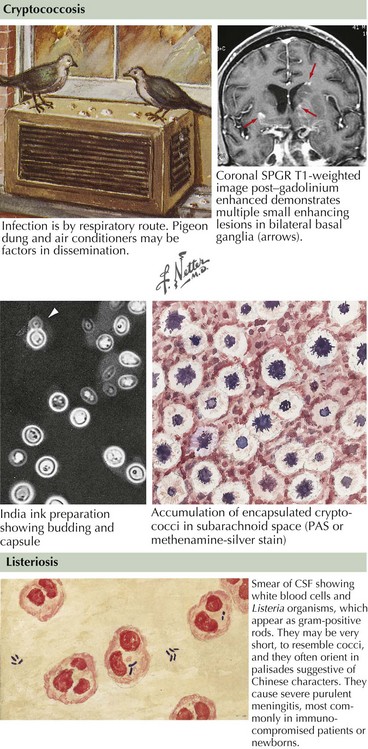
Listeriosis
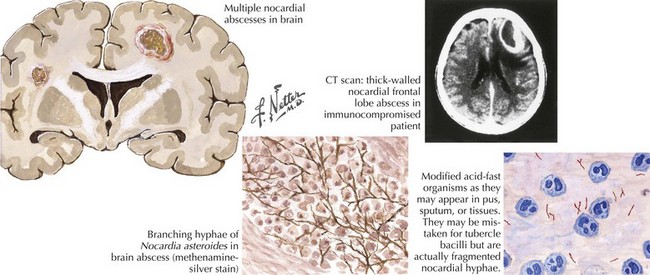
Nocardiosis
Diagnosis
Brain biopsy is the most reliable diagnostic technique if the diagnosis cannot be made by evaluation of pulmonary or skin lesions (Fig. 51-3). Nocardia are weakly acid-fast and can be stained with the modified Ziehl–Neelsen method. They may be isolated on Sabouraud’s medium or brain–heart infusion agar, but growth may not be visible for 2–4 weeks.
Toxoplasmosis
Epidemiology
Toxoplasma gondii is a parasite that infects most mammalian species (Fig. 51-4). Humans may acquire T. gondii infections by ingestion, transplacental transmission, blood transfusion, or organ transplantation. Oral route infection results from ingestion of T. gondii cysts in undercooked food (pork, lamb) or T. gondii oocysts found in the feces of 1% of cats. Human intestinal tract enzymes liberate T. gondii trophozoites, which cause clinical toxoplasmosis. Serologic evidence of Toxoplasma infection is present in 50% of the U.S. population. In most instances, T. gondii is a subclinical infection primarily manifested by cervical lymphadenopathy.

. Practice Guidelines of the Infectious Diseases Society of America. Available at http://www.idsociety.org/Content.aspx?id=9088 Accessed April 28, 2011. Evidence-based statements developed to assist practitioners and patients in making decisions about appropriate health care for specific clinical circumstances. Guidelines for treatment of infections by organ system and organism may be found here






