Published on 19/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 3430 times
Jane C. Sterling
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
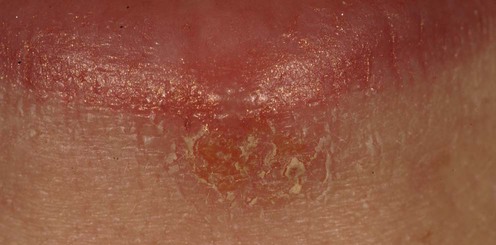
Herpes simplex virus (HSV) infects skin and mucous membranes damaging keratinocytes and causing intense inflammation, seen as small blisters on a background of erythema. Infections around the mouth or elsewhere on the skin are almost always due to HSV-1, whilst genital infection is most commonly caused by HSV-2. The primary infection may be obvious or subclinical; once latency is established in sensory ganglia, the virus may reactivate at variable intervals to produce visible lesions. In immunosuppression, disease can be chronic and antiviral resistance can develop.
Both primary and reactivation episodes are usually self-limiting and may require no treatment. Soothing antiseptic creams, alcohol-based tinctures or surface dressings may be used as self-help remedies. Antiviral therapy, in the form of acyclovir and related drugs, is available for topical and systemic use and is usually the most effective form of treatment. Although anogenital herpes will frequently respond to topical acyclovir applied five times daily for 5 days, its efficacy in cutaneous herpes is less certain, resulting in marginal benefit. Acyclovir 5% in combination with 1% hydrocortisone cream, appears to reduce the risk of ulceration. Oral acyclovir, 200 mg five times daily for 5 days, will usually reduce the time to healing and duration of virus shedding and is more effective than topical treatment. Shorter treatment courses with higher dose acyclovir produce similar effects. Topical or systemic treatment for an acute episode should be started early in the episode to have most benefit. In addition, pain relief may be necessary.
A failure of response to acyclovir may be due to the poor absorption and rapid clearance following ingestion or to the emergence of acyclovir resistance. Valacyclovir, a prodrug of acyclovir, and famciclovir, a prodrug of penciclovir, have improved bioavailability and are alternatives to acyclovir with the additional benefit of a once or twice daily dosing. Short course (single day) treatment with oral famciclovir can hasten healing if taken at the start of a reactivation episode. Efficacy of oral valacyclovir can be as good as intravenous acyclovir.
In frequently recurrent disease, or in immunosuppressed individuals when episodes may be severe, prophylactic antiviral treatment can be considered and measures taken to avoid any precipitating factors. UV protection may help to reduce viral reactivation in herpes labialis. To reduce frequency and severity of attacks, antiviral treatment needs to be continuous for several weeks or months. The dose of 400 mg twice daily for acyclovir is most likely to produce a decrease in the frequency of reactivation episodes. Oral valacyclovir or famciclovir can also be used for long-term suppression of viral reactivation. There is a potential risk of selection of resistant strains of virus with long-term therapy, but this is rare even in immunosuppressed patients. Oral antivirals may be taken as a relatively short-term course to reduce the risk of a reactivation episode before and during intense sun exposure, or before dental or cosmetic procedures.
In immunosuppressed individuals, with spreading or persistent infection, intravenous therapy with acyclovir, or the more toxic foscarnet or cidofovir, may be necessary. Topical preparations of cidofovir have been shown to have effect but are not commercially available. Vidarabine, interferons, and interleukin-2 and other agents have also been used, but without reliable effect. Herpes simplex is a common precipitating cause of episodes of recurrent erythema multiforme (see chapter on erythema multiforme), which can be reduced in frequency by prophylactic antiviral therapy.
Other treatments reported to have some effect in acute attacks include the antivirals idoxuridine, trifluorothymidine (TFT) and docosanol used topically and low-level laser light therapy.
Electron microscopy of blister fluid
PCR of blister fluid or biopsy
Viral culture from swab of lesion
Immunocytology of blister floor cells
Skin biopsy of atypical lesion
Herpes simplex serology
Assessment of immune function
The diagnosis is usually obvious clinically. In atypical disease, laboratory confirmation is essential. In unexplained persistent or severe disease, immunodeficiency should be excluded.
Amir J, Harel L, Smetana Z, Varsano I. BMJ 1997; 314: 1800–3.
A total of 61 children with herpetic gingivostomatitis were treated with acyclovir suspension 15 mg/kg or placebo five times daily for 7 days. Acyclovir reduced the duration of lesions from 10 to 4 days and reduced the period of viral shedding.
Spruance SL, Nett R, Marbury T, Wolff R, Johnson J, Spaulding T. Antimicrob Agents Chemother 2002; 46: 2238–43.
In two studies of a total of 1385 patients with recurrent herpes labialis, acyclovir 5% cream applied five times a day for 4 days reduced time to healing to an average of 4.4 days compared to 5.0 days when placebo was used.
Hull CM, Harmenberg J, Arlander E, Aoki F, Bring J, Darpö B, et al. J Am Acad Dermatol 2011; 64, 696. e1–e11.
Over 2400 patients randomized to use placebo vehicle, acyclovir 5% cream or acyclovir 5% with hydrocortisone 1% cream five times a day for 5 days demonstrated that the combination treatment slightly reduced lesion size and chance of ulceration compared with the acyclovir alone.
Spruance SL, Stewart JCB, Rowe NH, McKeough MB, Wenerstrom G, Freeman DJ. J Infect Dis 1990; 161: 185–90.
Herpes labialis was less painful and quicker to heal in 114 patients treated before the development of blistering with 400 mg acyclovir, five times daily for 5 days, compared to 60 given placebo treatment. The development of blisters and the size of the lesion were not affected by treatment.
Femiano F, Gombos F, Scully C. Oral Dis 2001; 7: 31–3.
Acyclovir 5% cream or penciclovir 1% cream was applied every 2 hours during waking hours for 4 days. Penciclovir treatment reduced the duration of symptoms by 1 day.
Spruance SL, Jones TM, Blatter MM, Vargas-Cortez M, Barber J, Hill J, et al. Antimicrob Agents Chemother 2003; 47: 1072–80.
Treatment at the start of an attack with either 2 g twice daily for 1 day or 2 g twice daily for 1 day plus 1 g twice daily for 1 day reduced the duration of the episode (5–5.5 days with placebo) by 0.5–1 day. The chance of an aborted episode was increased.
Spruance SL, Bodsworth N, Resnick H, Conant M, Oeuvray C, Gao J, et al. J Am Acad Dermatol 2006; 55: 47–53.
A total of 375 patients with recurrent herpes labialis completed the study. They were randomized into three groups to self-administer placebo, famciclovir 750 mg twice daily for 1 day or famciclovir 1500 mg as a single dose. Lesions healed in approximately 4 days in both groups taking famciclovir compared to 6 days for the placebo group.
Meyers JD, Wade JC, Mitchell CD, Saral R, Lietman PS, Durack DT, et al. Am J Med 1982; 73: 229–35.
Acyclovir given intravenously (250 mg/m2, three times per day for 7 days) to immunocompromised patients with active HSV infection (85% oral disease) was superior to placebo in reduction of pain and quicker healing, with a significant reduction in duration of virus shedding.
Hardy WD. Am J Med 1992; 92(Suppl 2A): 30s–5s.
Twenty-five patients with AIDS and acyclovir-resistant HSV infection were treated with foscarnet infusions for 2 weeks and then either for a further 8 weeks with 40 mg/kg daily or without further maintenance therapy. Healing of lesions was quickest in those treated for a total of 10 weeks.
Safrin S, Crumpacker C, Chatis P, Davis R, Hafner R, Rush J, et al. N Engl J Med 1991; 325: 551–5.
Foscarnet 40 mg/kg every 8 hours produced healing of acyclovir-resistant herpetic lesions within 4 weeks in eight patients with AIDS, while no improvement occurred in six similar patients treated with vidarabine 15 mg/kg daily.
Lalezari JP, Drew WL, Glutzer E, Miner D, Safrin S, Owen WF, et al. J Infect Dis 1994; 170: 570– 2.
Treatment with four intravenous infusions of 5 mg/kg/week of HPMPC (cidofovir) produced 95% healing in a patient with severe resistant herpetic lesions.
Lalezari J, Schacker T, Feinberg J, Gathe J, Lee S, Cheung T, et al. J Infect Dis 1997; 176: 892–8.
Twenty patients with AIDS applied 0.3% or 1% cidofovir gel once daily for 5 days; 50% healed or improved compared to 0% of the 10 placebo-treated patients. Cidofovir produced local inflammation in a quarter of patients.
Rooney JF, Bryson Y, Mannix ML, Dillon M, Wohlenberg CR, Banks S, et al. Lancet 1991; 338: 1419–22.
Using an experimental system of UV exposure to induce reactivation of herpes, 71% of 38 patients using a placebo developed lesions, whereas none developed in 35 patients using sunscreen.
Rooney JF, Straus SE, Mannix ML, Wohlenberg CR, Alling DW, Dumois JA, Notkins AL. Ann Intern Med 1993; 118: 268–72.
Twenty patients completed a randomized 4-month cross-over study receiving acyclovir 400 mg twice daily or placebo. During active treatment, there were an average of 0.85 reactivation episodes compared to 1.8 during placebo treatment.
Baker D, Eisen D. Cutis 2003; 71: 239–42.
Pooling results from two studies, 500 mg valacyclovir once daily for 4 months reduced relapse compared to placebo, with 60% of patients receiving antiviral therapy having no attack compared to 38% of those receiving placebo.
Dignani MC, Mykietiuk A, Michelet M, Intile D, Mammana L, Desmery P, et al. Bone Marrow Transplant 2002; 29: 263–7.
Comparison of intravenous acyclovir, oral valacyclovir, or no prophylaxis following bone marrow transplantation in over 100 patients showed equal efficacy of the two antivirals.
Alster TS, Nanni CA. Dermatolog Surg 1999; 25: 242–6.
The expected rate of HSV reactivation after facial cosmetic laser or chemical peel procedures is approximately 10%. With oral famciclovir, 250 or 500 mg twice daily for 10 days, the reactivation rate was similar, but the therapy was well tolerated.
Miller CS, Cunningham LL, Lindroth JE, Avdiushko SA. J Am Dent Assoc 2004; 135: 1311–8.
In a placebo-controlled trial of 125 adult patients with recurrent herpes labialis, valacyclovir (2 g twice daily on the day of dental treatment, with 1 g twice daily the following day) reduced the incidence of reactivation episodes from 20% (placebo) to 11% of treated individuals.
Spruance SL, Stewart CB, Freeman DJ, Brightman VJ, Cox JL, Wenerstrom. G, et al. J Infect Dis 1990; 161: 191–7.
Idoxuridine 15% solution, applied six times daily for 4 days starting within 1 hour of the onset of symptoms of a recurrence, significantly reduced pain and time to healing compared to 2% idoxuridine or dimethylsulfoxide alone.
Amin AR, Robinson MR, Smith DD, Swenson CF, Luque AE. AIDS 1996; 10: 1051–3.
Three patients responded to topical TFT applied five times daily for 14 days and then maintenance twice daily. Healing of previously acyclovir-resistant lesions occurred within 3 weeks.
Sacks SL, Thisted RA, Jones TM, Barbarash RA, Mikolich DJ, Ruoff GE, et al. J Am Acad Dermatol 2001; 45: 222–30.
Docosanol 10% cream applied five times a day until healing reduced symptoms and healing by approximately 1 day.
Hargate G. Clin Exp Dermatol 2006; 31, 638–41.
Twenty-seven patients with recurrent herpes labialis received placebo light or low level laser light treatment three times daily for 2 days and were followed up until complete healing. The mean time to healing in the placebo group was 9 days compared to 6 days in the active group.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us








 Topical acyclovir
Topical acyclovir Oral acyclovir
Oral acyclovir Topical penciclovir
Topical penciclovir Oral valacyclovir
Oral valacyclovir Oral famciclovir
Oral famciclovir Intravenous acyclovir
Intravenous acyclovir Intravenous vidarabine
Intravenous vidarabine Intravenous foscarnet
Intravenous foscarnet Intravenous cidofovir
Intravenous cidofovir Topical cidofovir
Topical cidofovir Suncreen
Suncreen Oral acyclovir
Oral acyclovir Oral valacyclovir
Oral valacyclovir Oral famciclovir
Oral famciclovir