Typically transmitted vertically, parenterally, or sexually





Top Differential Diagnoses

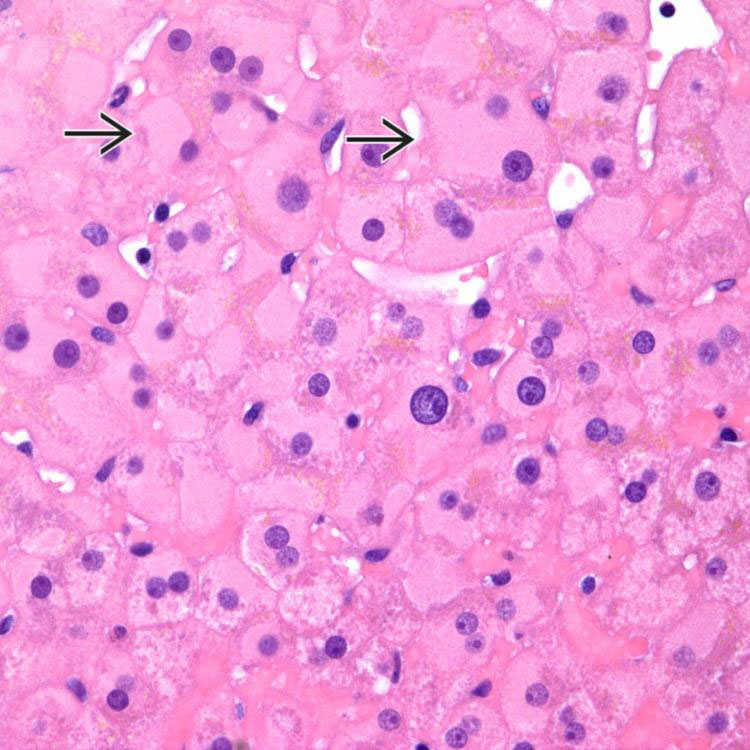
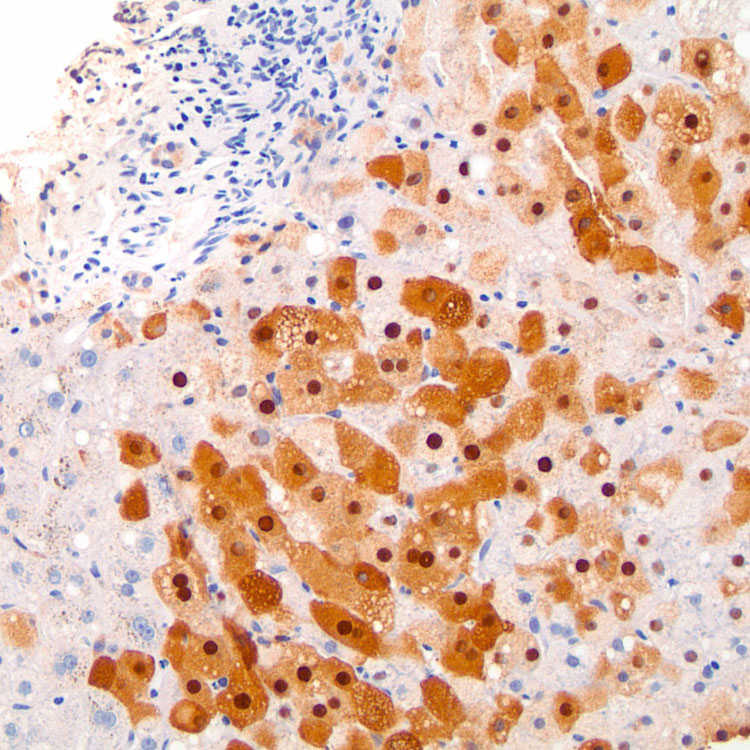
Ground-glass hepatocytes
 have glassy eosinophilic cytoplasm representing proliferation of smooth ER in response to HBsAg.
have glassy eosinophilic cytoplasm representing proliferation of smooth ER in response to HBsAg.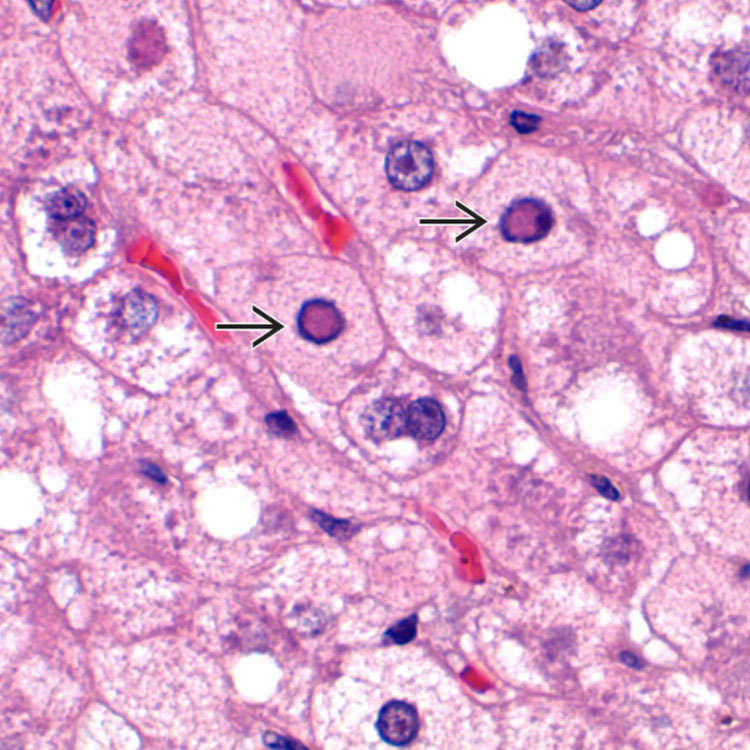
Hepatitis B-infected hepatocytes may have pale pink, finely granular intranuclear inclusions (sanded nuclei
 ) representing nuclear accumulation of HBcAg. These may be hard to detect on routine H&E staining.
) representing nuclear accumulation of HBcAg. These may be hard to detect on routine H&E staining.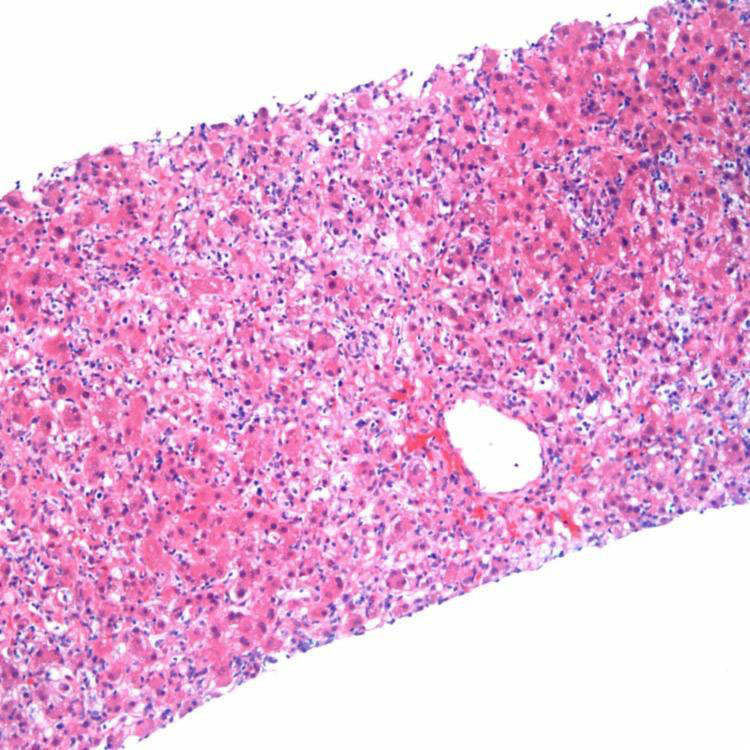
 into the periportal parenchyma.
into the periportal parenchyma.













MICROSCOPIC
Histologic Features





• Chronic hepatitis B
 Portal-based inflammation
Portal-based inflammation
Portal-based inflammation




















DIAGNOSTIC CHECKLIST
Pathologic Interpretation Pearls


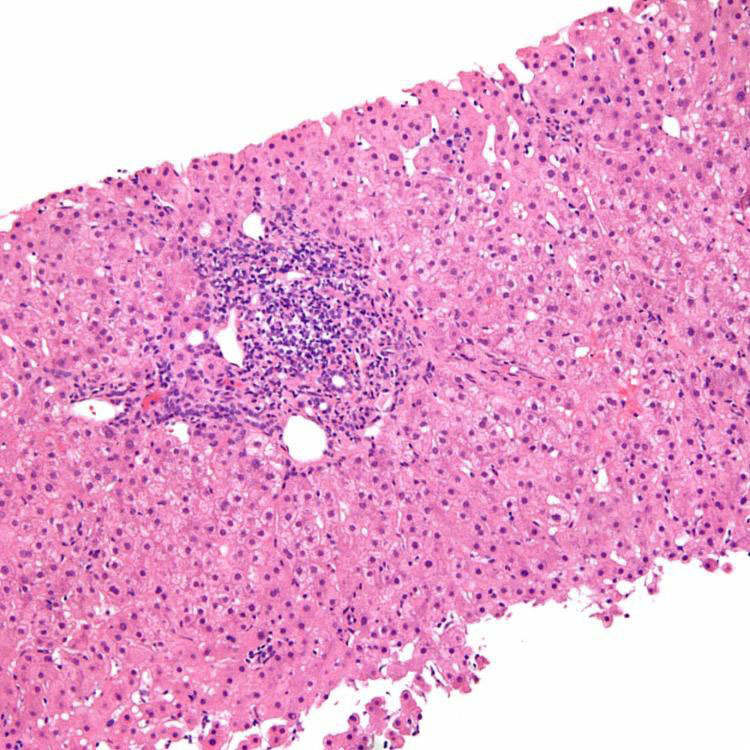
The features of chronic hepatitis B are often nonspecific, as seen in this biopsy with portal-based mononuclear cell inflammation. HBV and HCV can appear quite similar histologically and may also coexist.
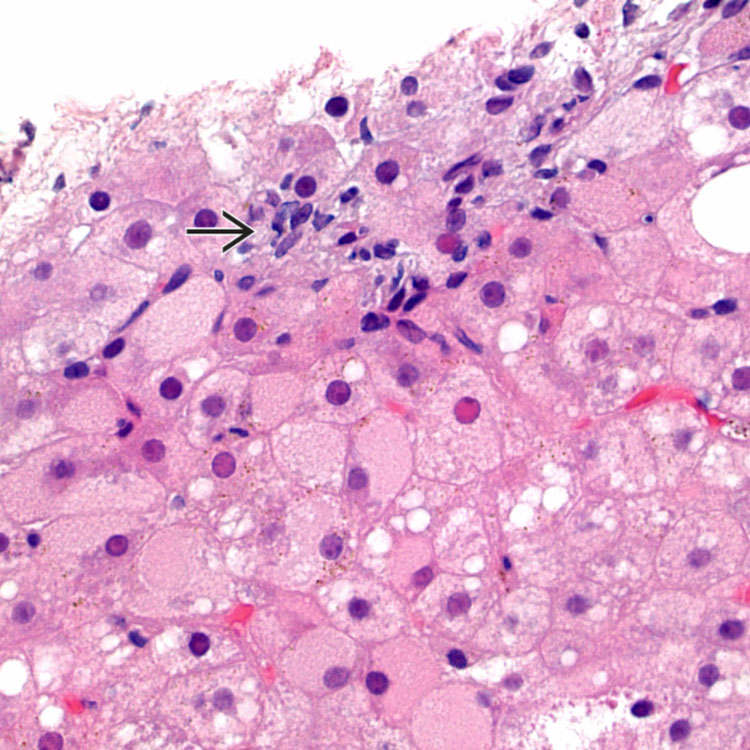
H&E section demonstrates a focus of lobular inflammation composed of lymphocytes and Kupffer cells
 . Ground-glass cells and sanded nuclei are present in surrounding hepatocytes.
. Ground-glass cells and sanded nuclei are present in surrounding hepatocytes.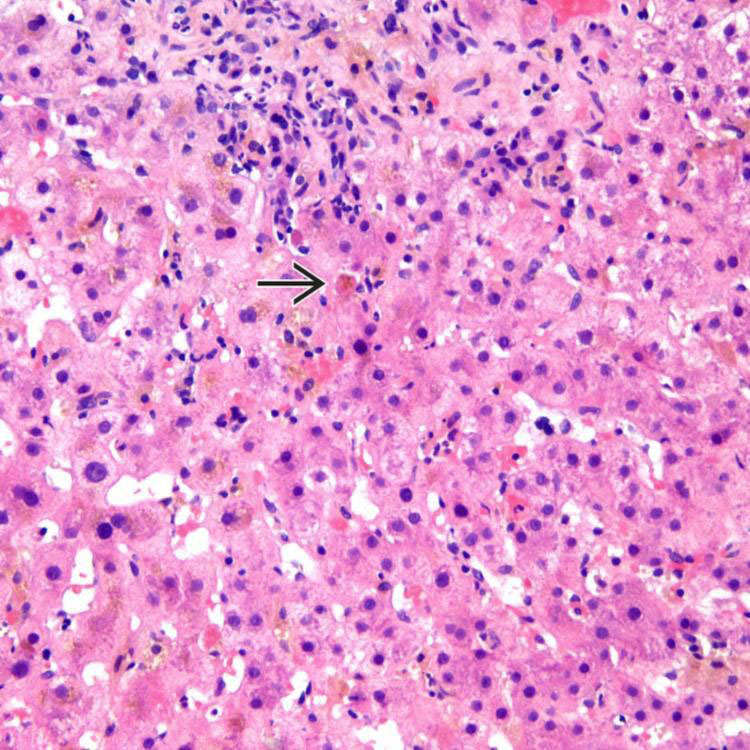
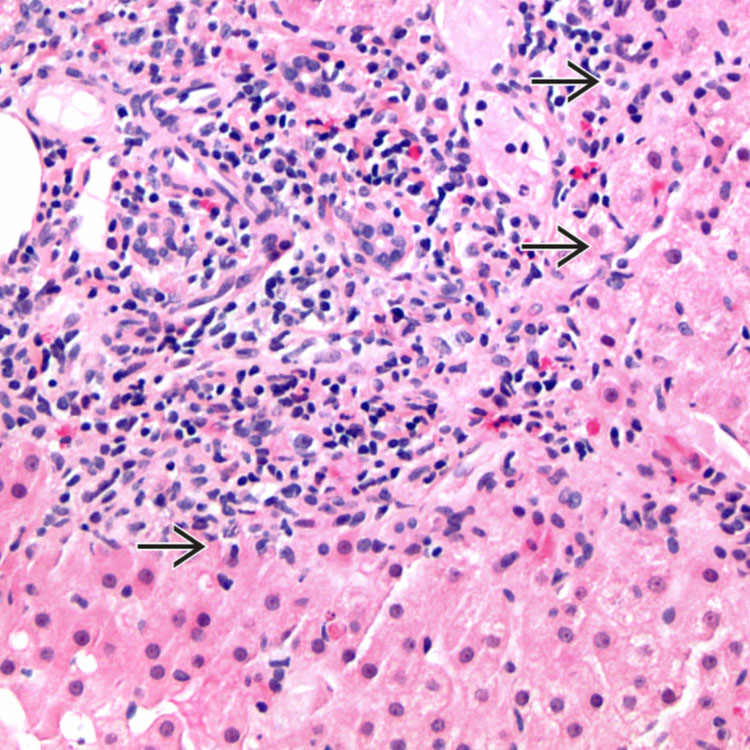
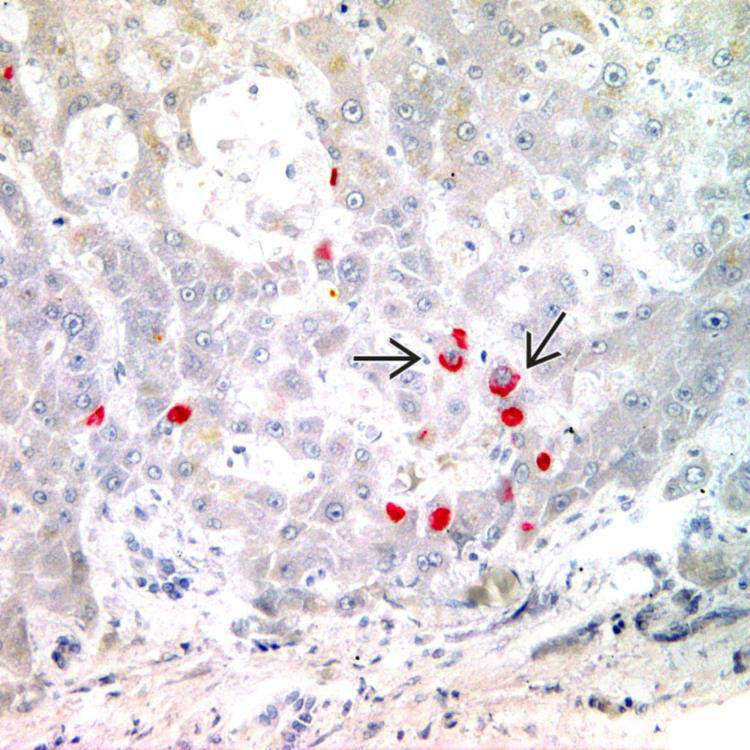
This case of acute hepatitis B shows lobular inflammation and scattered apoptotic hepatocytes
 . This case also has cholestatic features, which are occasionally seen in acute HBV infection.
. This case also has cholestatic features, which are occasionally seen in acute HBV infection.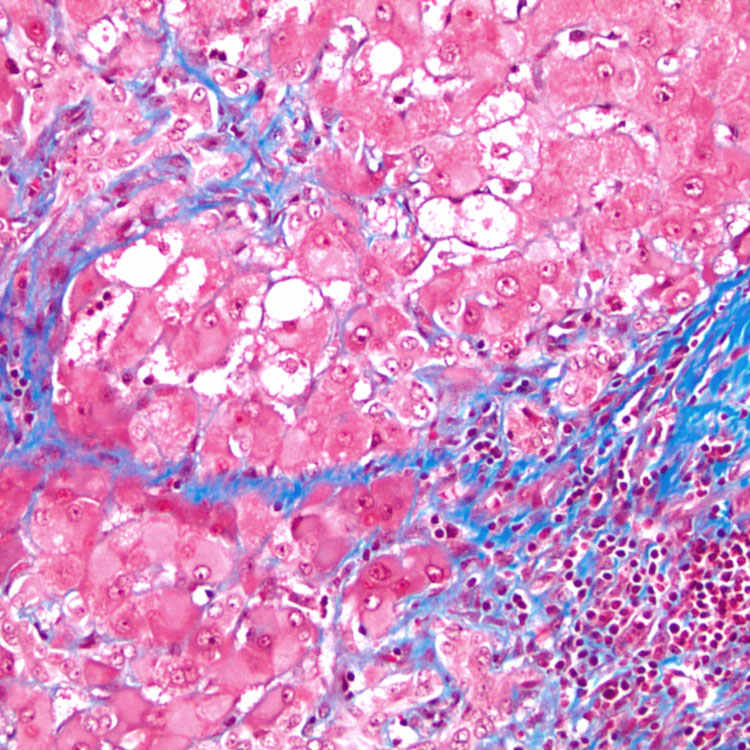
Masson trichrome stain shows collagen strands that extend beyond portal tracts to reach the central region and form bridging septa in chronic hepatitis B.
 .
.