Phytobezoar: Undigested vegetable matter












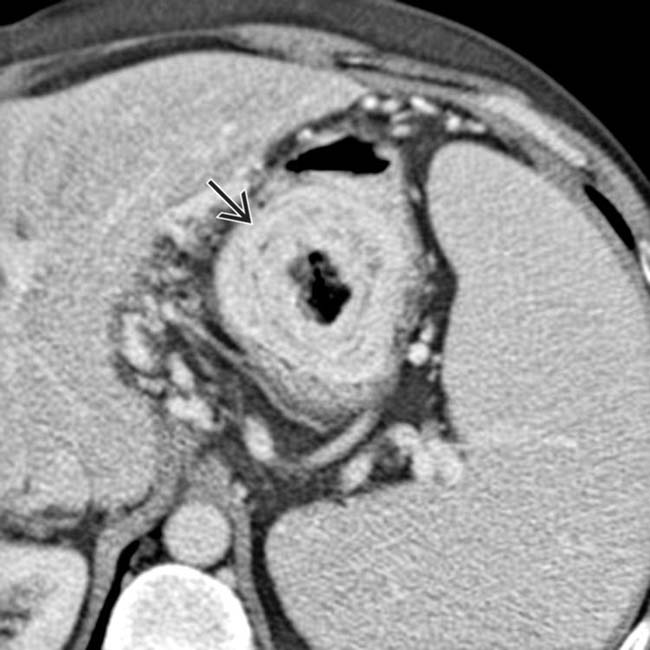
 in the stomach due to a phytobezoar.
in the stomach due to a phytobezoar.

IMAGING
General Features






























CLINICAL ISSUES
Presentation



















Natural History & Prognosis
• Bezoars of any type most often occur in background of altered motility or anatomy of gastrointestinal tract














 of the bezoar. Prior gastric surgery is a predisposing factor for developing a bezoar.
of the bezoar. Prior gastric surgery is a predisposing factor for developing a bezoar.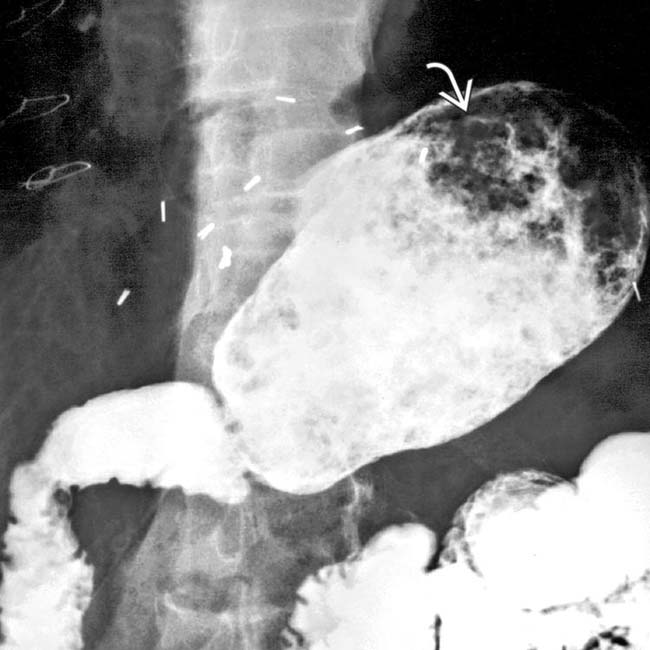
 in the stomach.
in the stomach.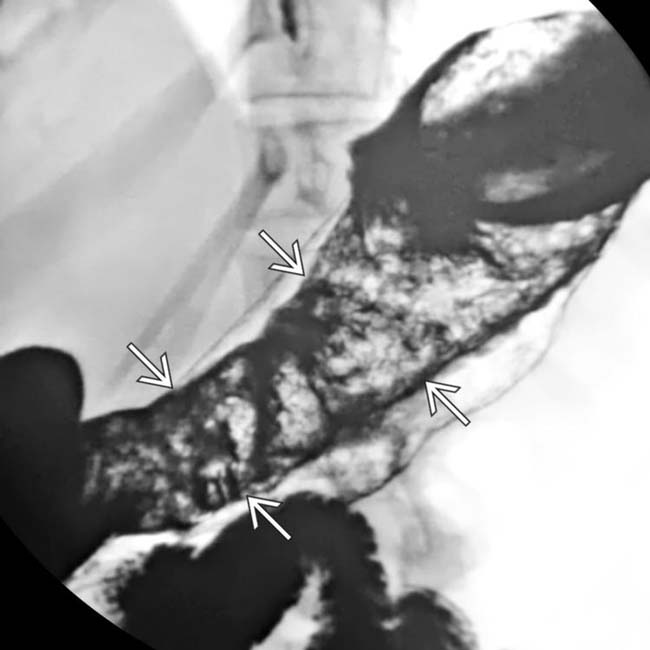
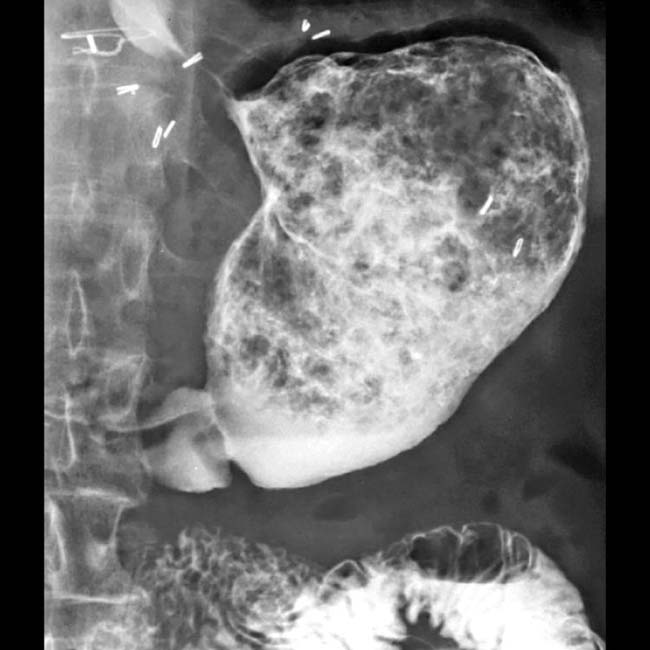
 corresponds to the shape of the stomach.
corresponds to the shape of the stomach.
 within the stomach that conform to the shape of the stomach. Notice that the rounded top of the mass is floating within the stomach.
within the stomach that conform to the shape of the stomach. Notice that the rounded top of the mass is floating within the stomach.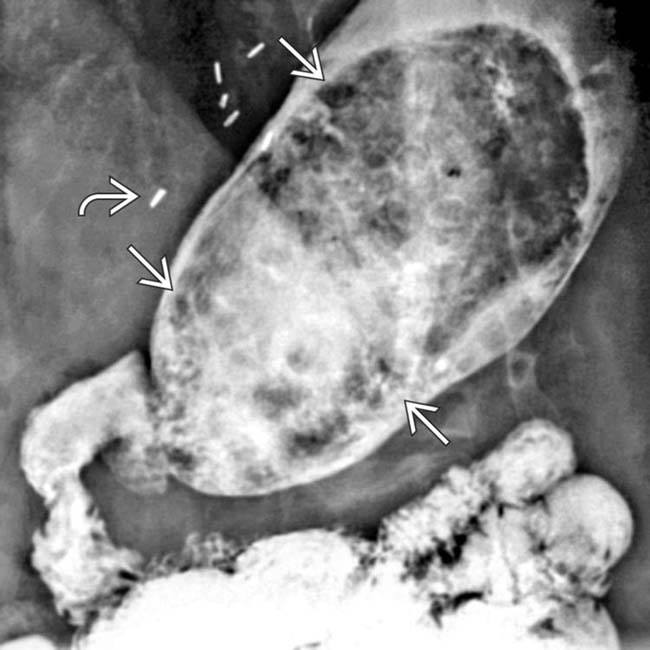
 from a vagotomy and the antrectomy with duodenal anastomosis (Billroth 1 procedure) are shown in a middle-aged man with phytobezoar. There is a solid mass
from a vagotomy and the antrectomy with duodenal anastomosis (Billroth 1 procedure) are shown in a middle-aged man with phytobezoar. There is a solid mass  with a gastric shape composed of gas and undigested plant material.
with a gastric shape composed of gas and undigested plant material.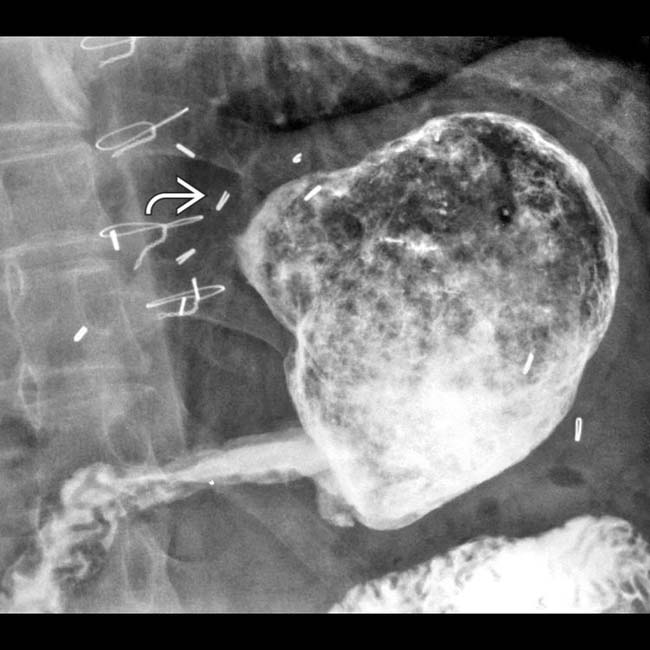
 as well as the bezoar.
as well as the bezoar.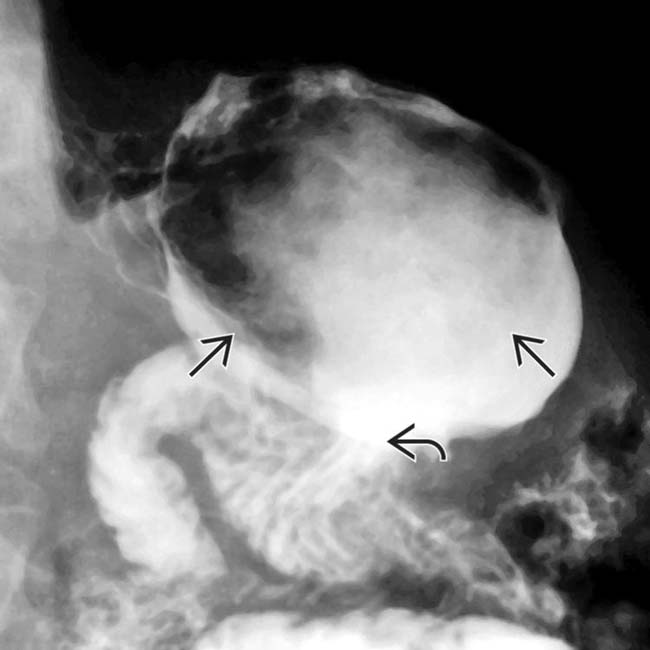
 . The bezoar
. The bezoar  is the fixed filling defect within the stomach.
is the fixed filling defect within the stomach.



