[level-membership-for-anesthesiology-category]
Evaluation of the coagulation system
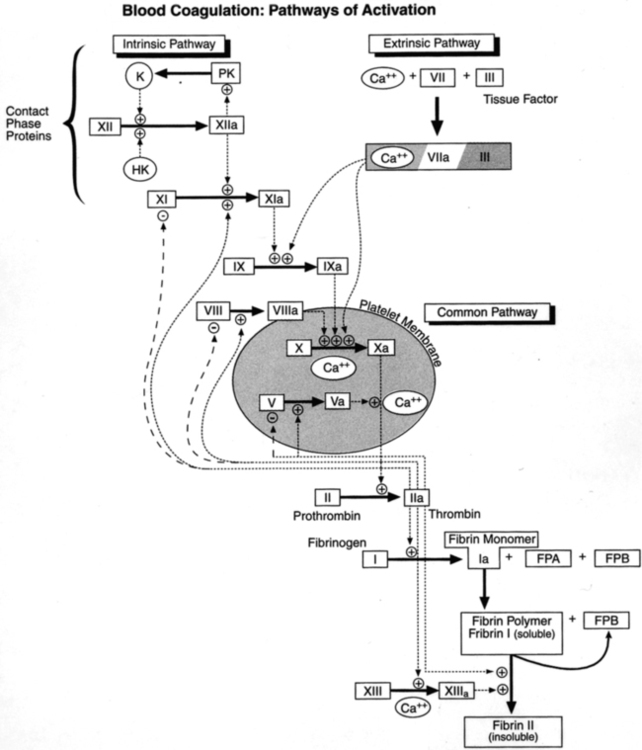
Evaluation of the coagulation system may be useful for the preoperative assessment of coagulation status and measurement of anticoagulation therapy, as well as the diagnosis and management of intraoperative coagulopathy. The dual-cascade concept of coagulation, which involves the intrinsic and extrinsic pathways, is now understood to be an inadequate and incomplete representation of in vivo coagulation. The three-stage process of actual in vivo coagulation (activation, amplification, and propagation) involves complex interactions among the vascular endothelium, tissue factor, platelets, and soluble clotting factors. However, the classic dual-cascade view may still be beneficial in providing a reasonable model of in vitro coagulation tests, that is, the activated partial thromboplastin time (aPTT) and prothrombin time (PT) (Figure 147-1).
Preoperative assessment
The best method to screen patients preoperatively for bleeding disorders remains a thorough clinical history. Routine coagulation testing is not warranted without indications. Clinical indications for testing include congenital or acquired bleeding disorders, excessive bleeding during previous operations, liver disease, and the use of drugs or supplements with anticoagulant properties. Table 147-1 summarizes the most common preoperative coagulation studies used for assessing the coagulation status of patients.
Table 147-1
Studies Commonly Used Preoperatively for Assessing Patients’ Coagulation Status
| Test | Measured Aspect | Comments |
| PT | Extrinsic pathway and common pathway | The PT is prolonged if any of factors VII, X, V, II, and I are deficient, abnormal, or inhibited. The coagulant activity of these factors must be <30% of normal and the fibrinogen concentration must be <100 mg/dL for the PT to be prolonged. The PT may be used as a screening test for patients on oral anticoagulant therapy. The PT may be used to assess the synthetic function of the liver. |
| aPTT | Intrinsic pathway and common pathway | The aPTT is prolonged when any of factors XII, XI, IX, VIII, X, V, II, and I are deficient, abnormal, or inhibited. The coagulant activity of these factors must be <30% of normal and the fibrinogen concentration must be <100 mg/dL for the PT to be prolonged. The aPTT is prolonged by heparin therapy. The aPTT is prolonged in hemophiliacs and, usually, in people with von Willebrand disease. |
| Fibrinogen | Fibrinogen level; common pathway | Levels <100 mg/dL may be associated with the inability to form a clot and severe bleeding. |
| Platelet count | Quantitative platelet assessment | The platelet count does not provide information regarding platelet function. Thrombocytopenia is defined as a platelet count <150,000/μL. Bleeding during surgery may be severe in patients with platelet counts of 40,000-70,000/μL. Spontaneous bleeding is unlikely to occur if the platelet count is >10,000-20,000/μL. |
| Bleeding time | Platelet function assessed by evaluating the time for a platelet plug to form after vascular injury | Bleeding times are prolonged in patients with platelet dysfunction (e.g., patients on aspirin therapy or those who are uremic). Owing to the techniques used for the test, reproducibility is poor, and results are imprecise. The bleeding time is not useful for routine screening. |
| Platelet aggregometry | Assesses the ability of platelets to aggregate after exposure to ADP, epinephrine, collagen, or ristocetin | Only qualitative results (clot retraction versus no clot retraction) are reported. Quantitative results are difficult to obtain. |
ADP, Adenosine diphosphate; aPTT, activated partial thromboplastin time; PT, prothrombin time.
Common point-of-care tests of coagulation
Viscoelastic measures of coagulation
Thromboelastography and the sonoclot
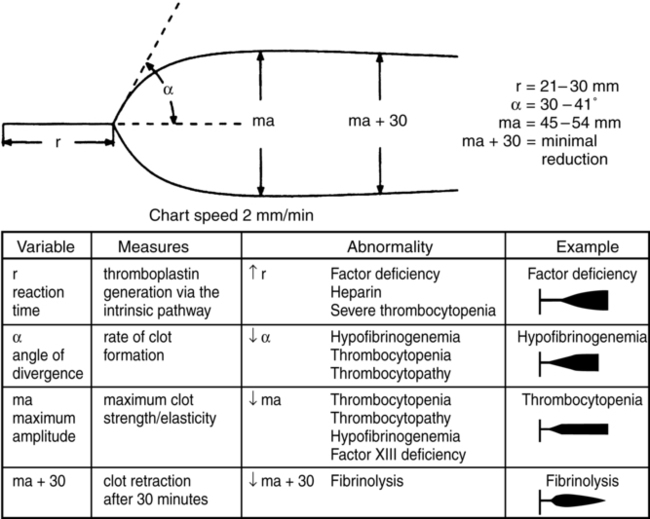
The thromboelastograph (TEG) (Haemascope, Niles, IL), like other viscoelastic measures of coagulation, is capable of measuring the complete coagulation process, from initial fibrin formation through fibrinolysis. The changes in viscoelasticity at all stages are both measured and displayed graphically. Even though the various TEG parameters do not directly correlate with other laboratory-based coagulation tests, they do correlate with specific abnormalities throughout the coagulation process. Figure 147-2 displays the variables measured by the TEG, as well as common abnormalities. Although the TEG is occasionally used in cardiac and trauma surgery, it is most frequently utilized during liver transplantation. The amounts of packed red blood cells and fresh frozen plasma that are transfused are lower when the TEG is used to guide transfusion, compared with transfusing based on routine coagulation tests.
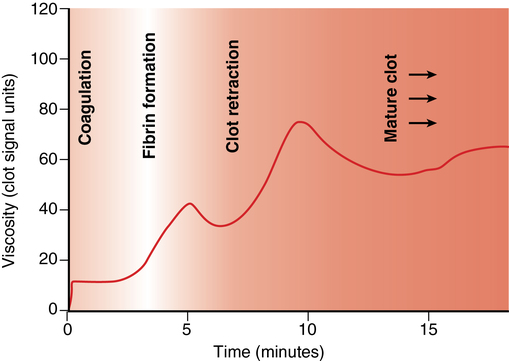
The Sonoclot Analyzer (Sienco, Inc., Arvada, CO) is another device used to monitor the viscoelastic properties of blood. It provides information on the entire hemostatic process in both a qualitative and quantitative fashion. The qualitative graph is known as the Sonoclot Signature (Figure 147-3), and the quantitative results measured are the ACT, the clot rate, and platelet function.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
Evaluation of the coagulation system
Evaluation of the coagulation system may be useful for the preoperative assessment of coagulation status and measurement of anticoagulation therapy, as well as the diagnosis and management of intraoperative coagulopathy. The dual-cascade concept of coagulation, which involves the intrinsic and extrinsic pathways, is now understood to be an inadequate and incomplete representation of in vivo coagulation. The three-stage process of actual in vivo coagulation (activation, amplification, and propagation) involves complex interactions among the vascular endothelium, tissue factor, platelets, and soluble clotting factors. However, the classic dual-cascade view may still be beneficial in providing a reasonable model of in vitro coagulation tests, that is, the activated partial thromboplastin time (aPTT) and prothrombin time (PT) (Figure 147-1).
Preoperative assessment
The best method to screen patients preoperatively for bleeding disorders remains a thorough clinical history. Routine coagulation testing is not warranted without indications. Clinical indications for testing include congenital or acquired bleeding disorders, excessive bleeding during previous operations, liver disease, and the use of drugs or supplements with anticoagulant properties. Table 147-1 summarizes the most common preoperative coagulation studies used for assessing the coagulation status of patients.
Table 147-1
Studies Commonly Used Preoperatively for Assessing Patients’ Coagulation Status
| Test | Measured Aspect | Comments |
| PT | Extrinsic pathway and common pathway | The PT is prolonged if any of factors VII, X, V, II, and I are deficient, abnormal, or inhibited. The coagulant activity of these factors must be <30% of normal and the fibrinogen concentration must be <100 mg/dL for the PT to be prolonged. The PT may be used as a screening test for patients on oral anticoagulant therapy. The PT may be used to assess the synthetic function of the liver. |
| aPTT | Intrinsic pathway and common pathway | The aPTT is prolonged when any of factors XII, XI, IX, VIII, X, V, II, and I are deficient, abnormal, or inhibited. The coagulant activity of these factors must be <30% of normal and the fibrinogen concentration must be <100 mg/dL for the PT to be prolonged. The aPTT is prolonged by heparin therapy. The aPTT is prolonged in hemophiliacs and, usually, in people with von Willebrand disease. |
| Fibrinogen | Fibrinogen level; common pathway | Levels <100 mg/dL may be associated with the inability to form a clot and severe bleeding. |
| Platelet count | Quantitative platelet assessment |
