[level-membership-for-dermatology-category]
Epidermal nevi
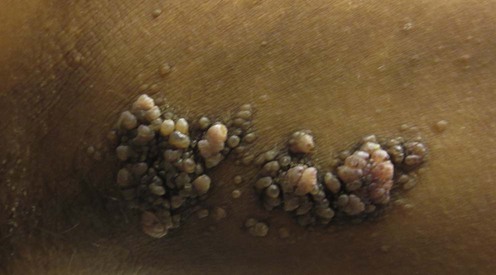
(Courtesy of Neil Fernandes, MD.)
Specific investigations


Verrucous epidermal nevi
First-line therapies
 Excision under local anesthetic
Excision under local anesthetic Shave or curettage under local anesthetic
Shave or curettage under local anesthetic Cryotherapy
CryotherapySecond-line therapies
 Laser ablation
Laser ablation Dermabrasion
Dermabrasion Ruby laser
Ruby laser Erbium : YAG laser
Erbium : YAG laserThird-line therapies
 Systemic retinoids
Systemic retinoids Topical retinoids plus 5-fluorouracil
Topical retinoids plus 5-fluorouracil Photodynamic therapy
Photodynamic therapyInflammatory/dysplastic epidermal nevi
 Topical corticosteroids
Topical corticosteroidsSecond-line therapies
 Topical calcipotriol/tacalcitol
Topical calcipotriol/tacalcitol Topical retinoids
Topical retinoids Systemic retinoids
Systemic retinoids Topical dithranol
Topical dithranolThird-line therapies
 Pulsed-dye laser
Pulsed-dye laser CO2 laser
CO2 laser Surgical excision
Surgical excision Etanercept
Etanercept Photodynamic therapy
Photodynamic therapy
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Epidermal nevi
(Courtesy of Neil Fernandes, MD.)
Specific investigations
Verrucous epidermal nevi
First-line therapies
Buy Membership for Dermatology Category to continue reading. Learn more here
[/not-level-membership-for-dermatology-category]
