[level-membership-for-surgery-category]
CHAPTER 10 Enteral Access Procedures
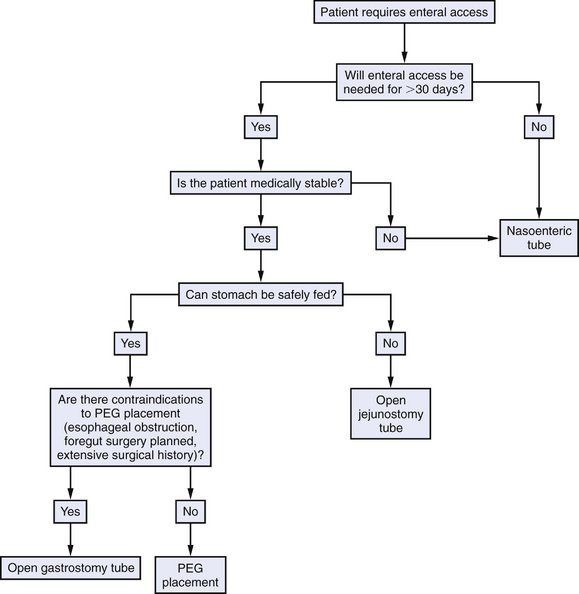
INDICATIONS FOR SURGERY
PREOPERATIVE EVALUATION
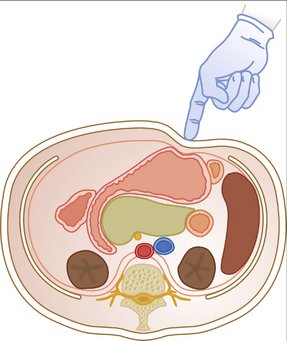
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Preoperative Considerations
Positioning and Preparation
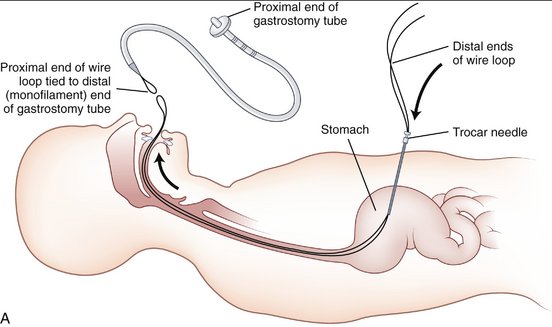
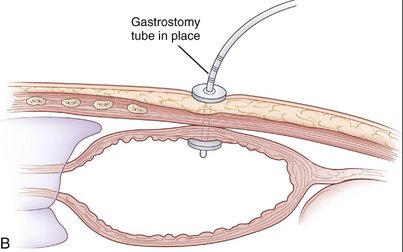
PEG Tube
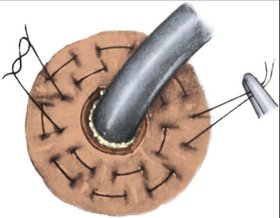
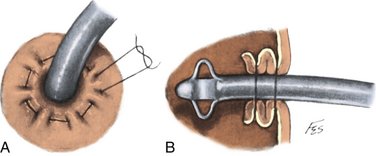
Open Tube Gastrostomy
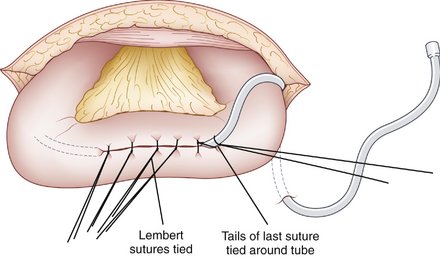
Open Tube Jejunostomy
COMPLICATIONS
Gorman R, Nance ML, Morris JB. Enteral feeding techniques [[ed]]. Torosian MH, editor. Nutrition for the Hospitalized Patient: Basic Science and Principles of Practice. CRC Press, New York, 1995, 329-351.
Mullen JL, Morris JB, Yu JC. Enterostomies. In: Daly JM, Cady B, editors. Atlas of Surgical Oncology. Philadelphia: Mosby-Year Book; 1993:19-37.
Tapia J, Murguia R, Garcia G, et al. Jejunostomy: techniques, indications, and complications. World J Surg. 1999;23:596-602.
Weltz CR, Morris JB, Mullen JL. Surgical jejunostomy in aspiration risk patients. Ann Surg. 1992;215:140-145.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 10 Enteral Access Procedures
INDICATIONS FOR SURGERY
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Preoperative Considerations
Positioning and Preparation
PEG Tube
[/not-level-membership-for-surgery-category]
