Chapter 641 Ectodermal Dysplasias
Anhidrotic (Hypohidrotic) Ectodermal Dysplasia
The syndrome known as anhidrotic ectodermal dysplasia manifests as a triad of defects: partial absence (hypohidrosis) or complete absence of sweat glands, anomalous dentition, and hypotrichosis. There are 4 recognized types of anhidrotic ectodermal dysplasia (Table 641-1). The X-linked form is most common.
Table 641-1 FOUR RECOGNIZED TYPES OF ANHIDROTIC ECTODERMAL DYSPLASIA
| TYPE | INHERITANCE | GENE DEFECT |
|---|---|---|
| ED-1 | X-linked recessive | Ectodysplasin A (EDA) |
| ED-anhidrotic | Autosomal recessive | Ectodyplasin A anhidrotic receptor (EDAR) |
| EDAR-associated death gene (EDARADD) | ||
| ED-3 | Autosomal dominant | EDAR |
| ED-anhidrotic with immune deficiency |
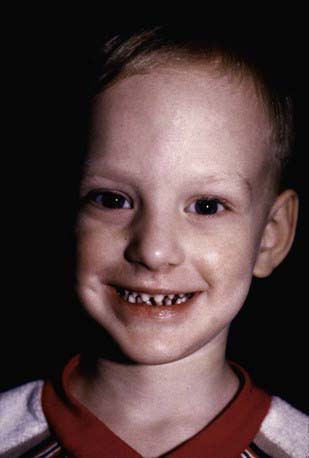
In ED-1, affected males are unable to sweat and may experience episodes of high fever in warm environments, which may be mistakenly considered to be fevers of unknown origin. This error is particularly common in infancy, when the facial changes are not easily appreciated. Diagnosis at this time may be made using the starch-iodine test or palmar or scalp biopsy. Scalp biopsy is the most sensitive and is 100% specific. The typical facies is characterized by frontal bossing; malar hypoplasia; a flattened nasal bridge; recessed columella; thick, everted lips; wrinkled, hyperpigmented periorbital skin; and prominent, low-set ears (Fig. 641-1). The skin over the entire body is dry, finely wrinkled, and hypopigmented, often with a prominent venous pattern. Extensive peeling of the skin is a clinical clue to diagnosis in the newborn period. The paucity of sebaceous glands may account for the dry skin. The scalp hair is sparse, fine, and lightly pigmented, and eyebrows and lashes are sparse or absent. Other body hair is also sparse or absent. Sexual hair growth is normal. Anodontia or hypodontia with widely spaced, conical teeth is a consistent feature (see Fig. 641-1). Otolaryngeal and ophthalmologic abnormalities secondary to decreased saliva and tear production are seen. The incidence of atopic diseases in children with ED-1 is high. Gastroesophageal reflux is common and may play a role in failure to thrive, which is seen in 20% of cases. Sexual development is usually normal. Historically, the infant mortality rate has been 30%. Carrier females have no or variable clinical manifestations.
Baris HN, Zlotogorski A, Peretz-Amit G, et al. A novel GJB6 mutation in hidrotic ectodermal dysplasia 2 (Clouston syndrome) broadens its genotypic basis. Br J Dermatol. 2008;159:1373-1376.
Gunadi, M K, Ohta M, et al. Two novel mutations in the ED1 gene in Japanese families with X-linked hypohidrotic ectodermal dysplasia. Pediatr Res. 2009;65:453-457.
Lu PD, Schaffer JV. Hypohidrotic ectodermal dysplasia. Dermat Online J. 2008;14:22.





