Used to describe ductopenia related to drugs but not specific term
Etiology/Pathogenesis
• Many medication classes implicated
Antiinflammatory, antibiotics, antiepileptics, psychiatric drugs, tranquilizers, hypoglycemics, and others
• Also occurs with herbal or toxin exposure or genetic disposition
Clinical Issues
• Jaundice
Temporal relationship between drug administration and onset of signs and symptoms
Most patients recover fully with discontinuation of drug
Few cases develop chronic cholestatic injury
Microscopic
• Generally, no specific features indicating injury is drug related
Cholestasis, usually zone 3
Bile duct epithelial cell injury
– Cytoplasmic eosinophilia &/or vacuolization
– Nuclear pleomorphism and uneven nuclear spacing
– Apoptosis and atrophy of ductal epithelium
Bile ductular proliferation
Lymphocytic or mixed cell cholangitis
• Some cases show changes of progression/chronicity
Progressive ductopenia
Periportal hepatocyte swelling and copper accumulation
Bile Duct Injury Secondary to ACE Inhibitor This example of drug-induced cholangitis due to an ACE inhibitor shows a damaged duct with eosinophilic cytoplasm, irregular spaces between nuclei, and variation in nuclear size and shape.
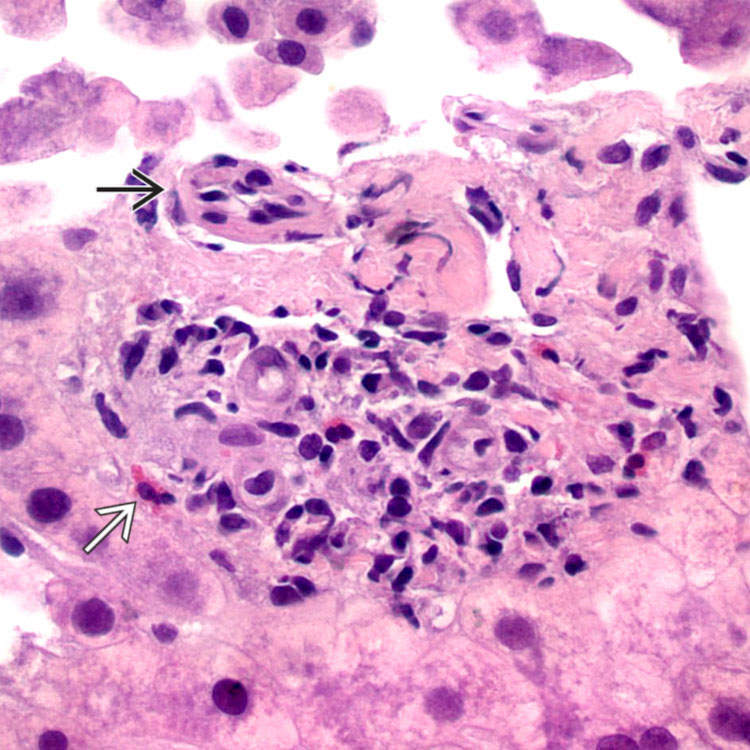
Cholangitis With Neutrophils and Eosinophils This example of drug-related cholangitis due to antibiotics shows a duct with cholangitis surrounded by portal edema and an infiltrate that is rich in eosinophils.
Drug-Related Bile Duct Injury This severely injured duct shows marked cytoplasmic vacuolization and eosinophilia as well as irregularly spaced nuclei.
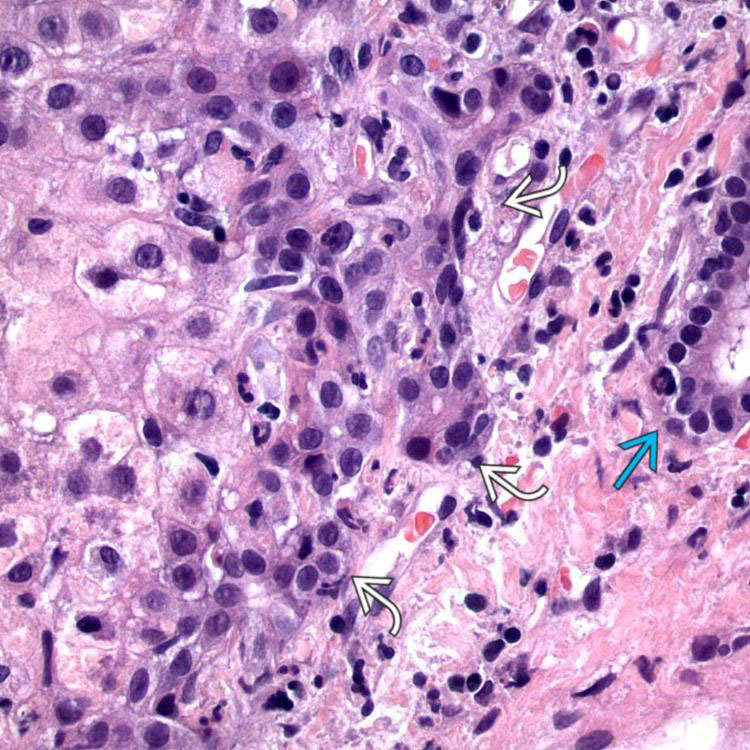
Ductular Reaction Numerous proliferating bile duct profiles are seen at the edge of this portal tract in a case of drug-related cholangitis. The native bile duct is distinct from these proliferating bile duct profiles.
TERMINOLOGY
Synonyms
• Cholangiodestructive cholestasis
• Vanishing bile duct syndrome: Ductopenia related to drugs but not specific entity, ductopenia in graft-vs.-host disease and chronic ductopenic rejection
• Stevens-Johnson syndrome
Drug reaction associated with severe mucocutaneous manifestations and vanishing bile duct syndrome
Definitions
• Bile duct injury, cholangitis, &/or ductopenia related to adverse drug reactions
Often accompanied by cholestasis
ETIOLOGY/PATHOGENESIS
2 Categories of Injury
• Predictable: Dose related, reproducible, and related to intrinsic toxicity of drug or its metabolites
• Idiosyncratic: Unpredictable, unrelated to dose, not reproducible in animal models
Allergic or autoimmune responses to drug or its metabolite may be involved
• Clinical context of liver transplantation, presence of endothelialitis
DIAGNOSTIC CHECKLIST
Clinically Relevant Pathologic Features
• Histologic features usually cannot provide definite diagnosis of drug-related injury but can assist in excluding other etiologies
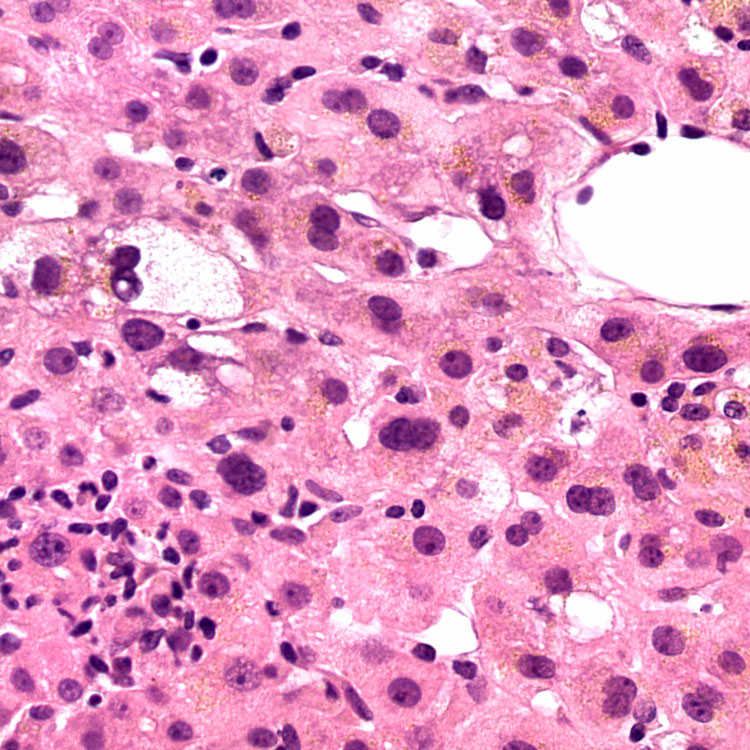
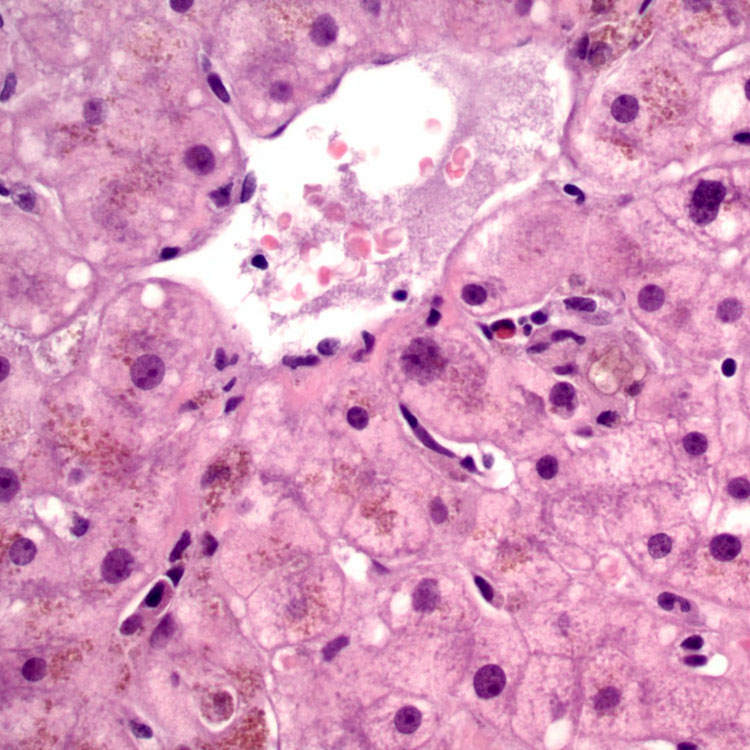
Centrilobular Cholestasis Due to NSAIDs Centrilobular cholestasis and varying degrees of lobular inflammation, hepatocyte damage, and reactive hepatocellular changes can be seen in drug-induced cholangitis. This case is due to NSAID injury.
Canalicular Cholestasis A high-power view shows canalicular cholestasis in zone 3, which is a common finding in drug-associated cholangitis.
Mild Portal Inflammation and Duct Injury This example of duct injury due to NSAIDs shows mild portal edema, a mild portal mononuclear cell infiltrate, and a damaged duct with eosinophilic cytoplasm and variation in nuclear size.
Lymphocytic Infiltrate and Duct Injury Portal tracts may be edematous, and the inflammatory infiltrate may be predominantly mononuclear or contain eosinophils. Note the damaged duct with eosinophilic cytoplasm and “jumbled” nuclei.
Mixed Portal Inflammation The portal infiltrate may contain prominent eosinophils and plasma cells. Note the cholangiolar proliferation at the edges of the portal tract.
Ductular Reaction Patchy ductular reaction is a common finding in drug-associated cholangitis and duct injury.
Ductular Reaction Extensive bile ductular reaction is seen at the edge of this portal tract . The native bile duct is seen at the edge of the image.
Injured Bile Ducts Mild Portal Inflammation The 2 bile ducts in this portal tract exhibit variation in nuclear shape and size and uneven spacing of nuclei . One bile duct is also infiltrated by lymphocytes .
Centrilobular Cholestasis Secondary to Augmentin This case of Augmentin-associated vanishing bile duct syndrome showed zone 3 cholestasis, a common finding in drug-related duct injury.
Bile Duct Loss This portal tract in vanishing bile duct syndrome lacks a duct altogether. Note the unaccompanied hepatic arteriole and the mononuclear cell portal infiltrate with admixed eosinophils .
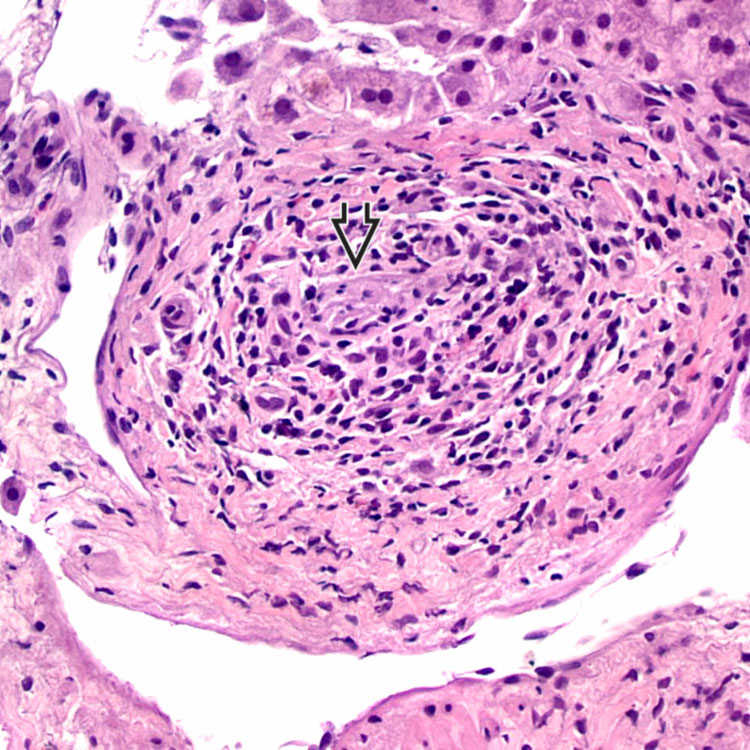
Markedly Damaged Duct This portal tract from a case of Augmentin-associated vanishing bile duct syndrome shows a barely discernible bile duct remnant surrounded by mononuclear cells.
Duct Destruction A high-power view of a portal tract from a case of Augmentin-associated vanishing bile duct syndrome shows duct destruction and a predominantly mononuclear portal inflammatory infiltrate.











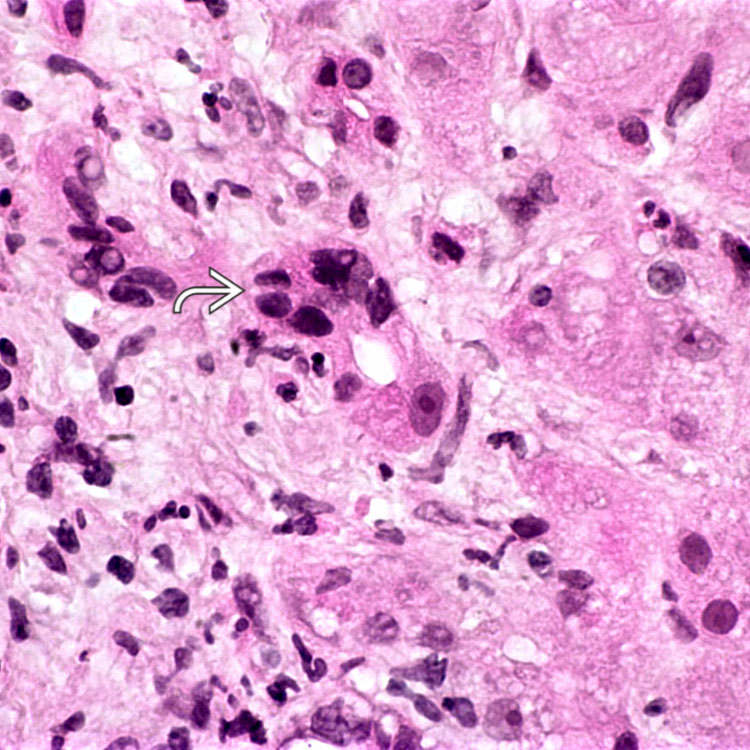
 with eosinophilic cytoplasm, irregular spaces between nuclei, and variation in nuclear size and shape.
with eosinophilic cytoplasm, irregular spaces between nuclei, and variation in nuclear size and shape.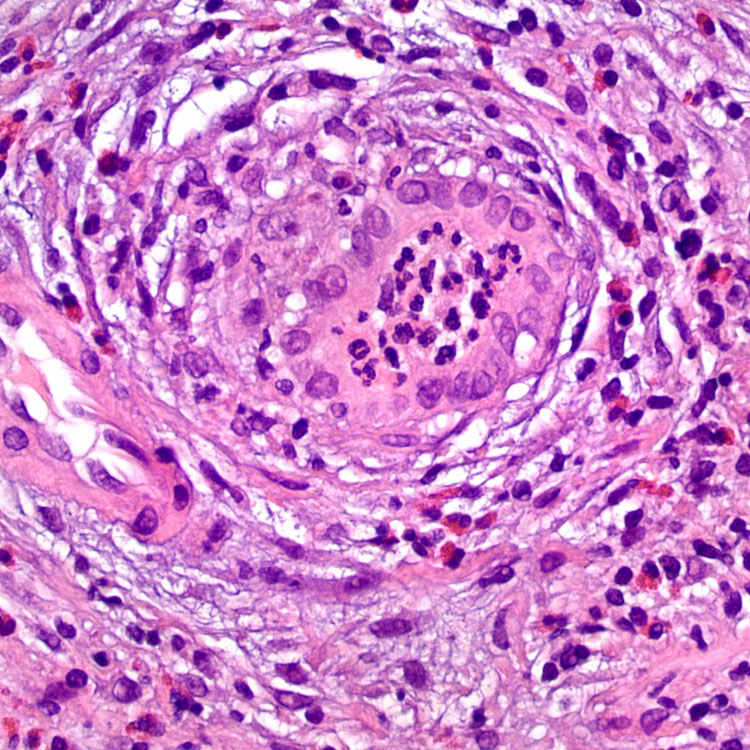
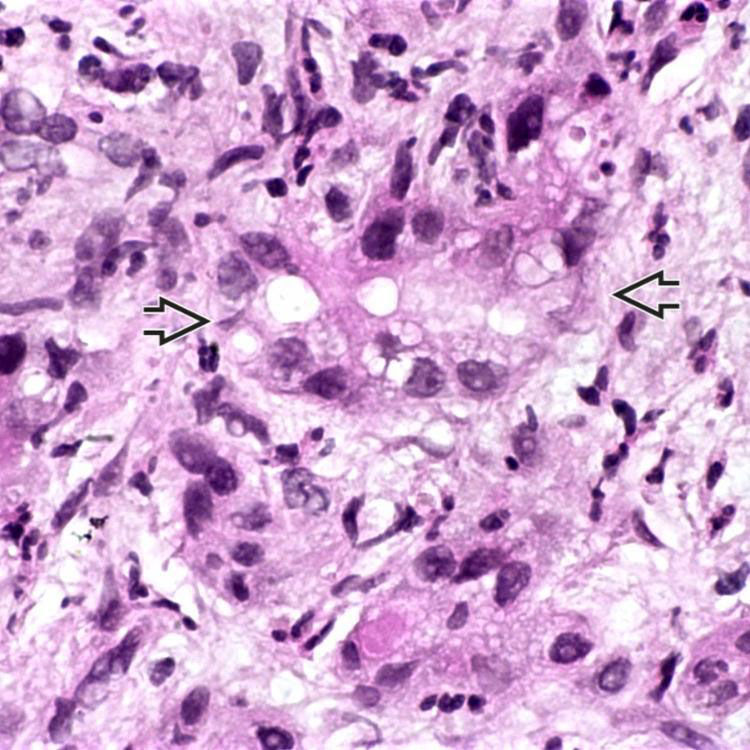
 shows marked cytoplasmic vacuolization and eosinophilia as well as irregularly spaced nuclei.
shows marked cytoplasmic vacuolization and eosinophilia as well as irregularly spaced nuclei.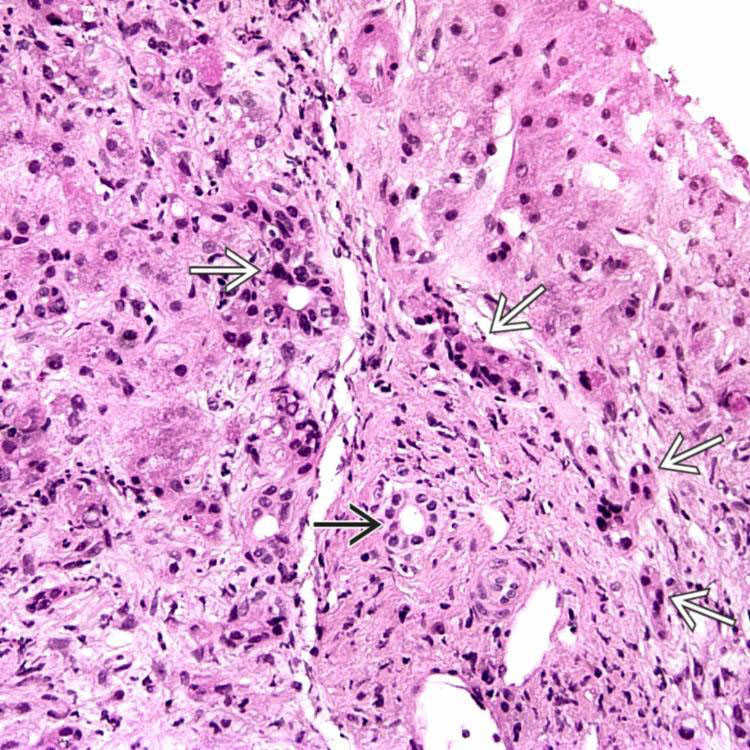
 are seen at the edge of this portal tract in a case of drug-related cholangitis. The native bile duct is distinct
are seen at the edge of this portal tract in a case of drug-related cholangitis. The native bile duct is distinct  from these proliferating bile duct profiles.
from these proliferating bile duct profiles.























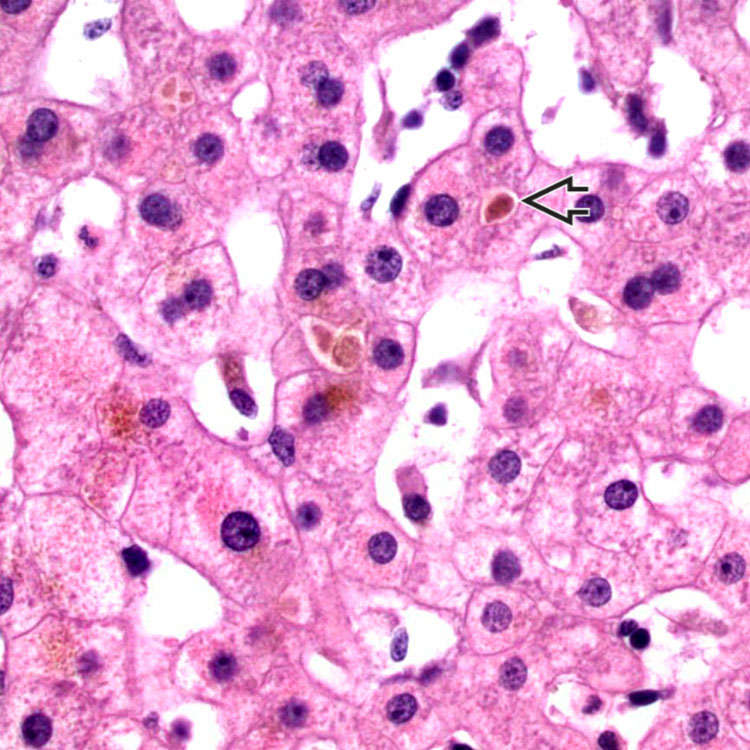
 in zone 3, which is a common finding in drug-associated cholangitis.
in zone 3, which is a common finding in drug-associated cholangitis.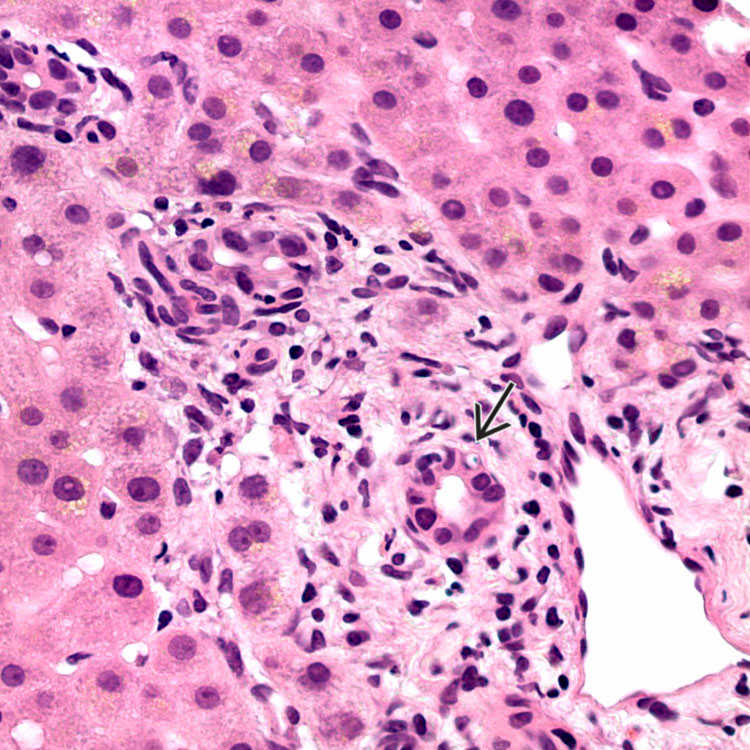
 with eosinophilic cytoplasm and variation in nuclear size.
with eosinophilic cytoplasm and variation in nuclear size.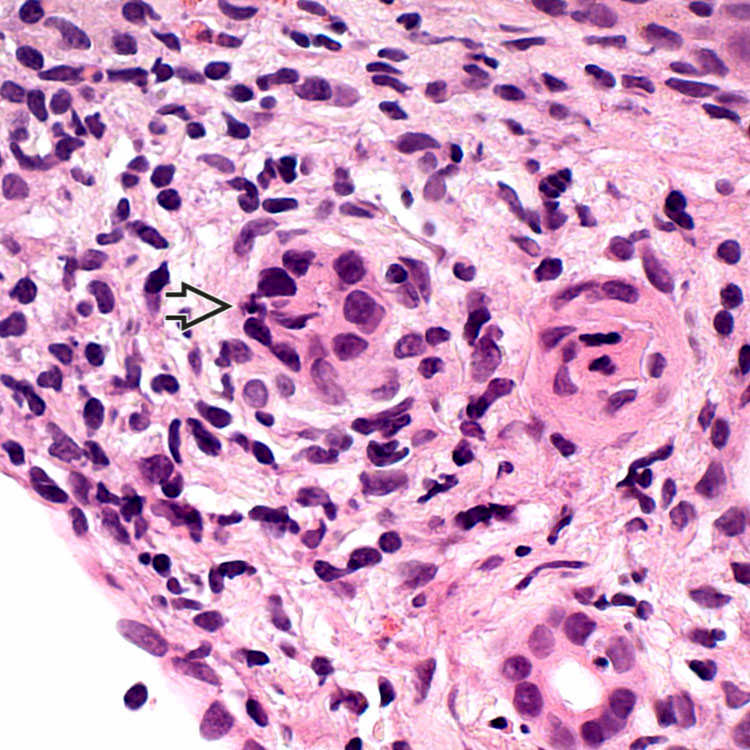
 with eosinophilic cytoplasm and “jumbled” nuclei.
with eosinophilic cytoplasm and “jumbled” nuclei.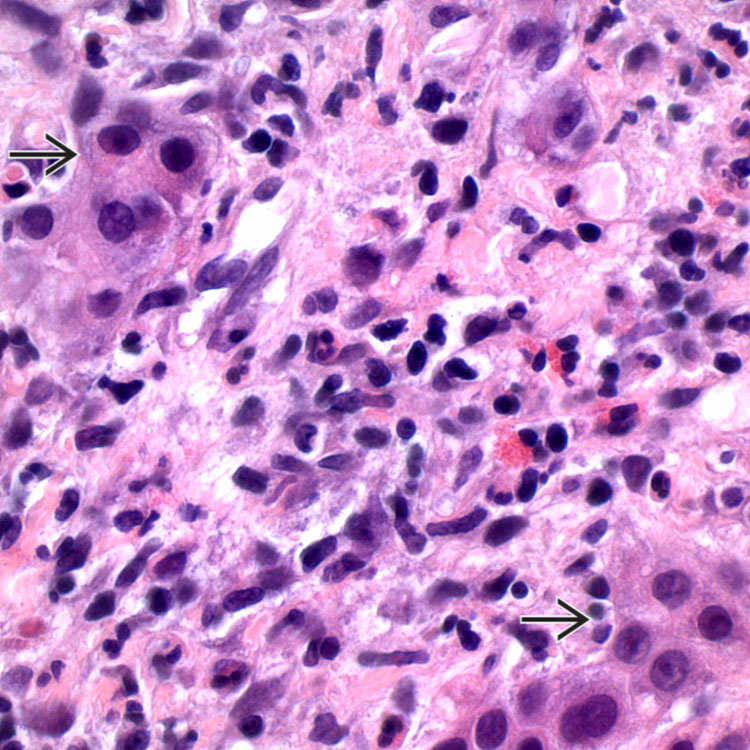
 at the edges of the portal tract.
at the edges of the portal tract.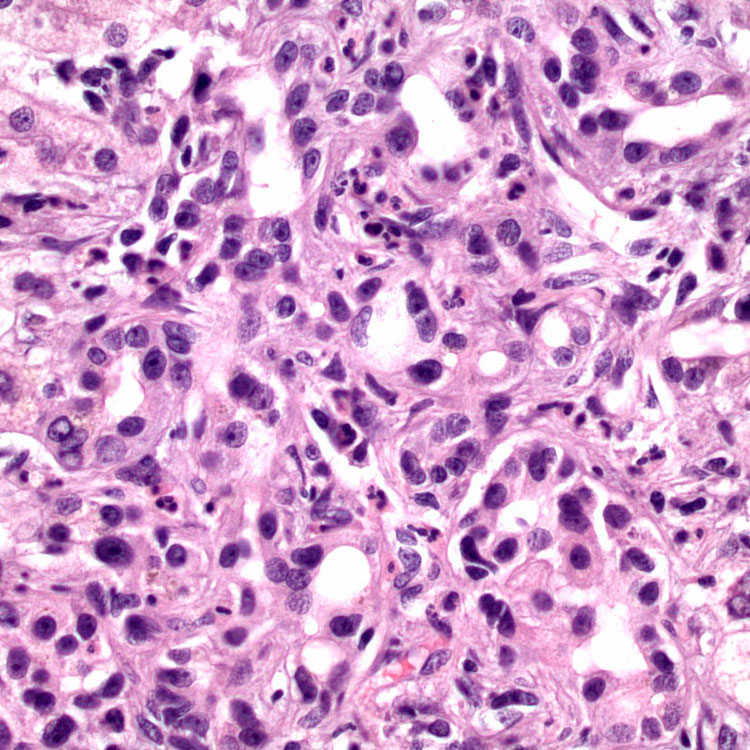
 . The native bile duct
. The native bile duct  is seen at the edge of the image.
is seen at the edge of the image.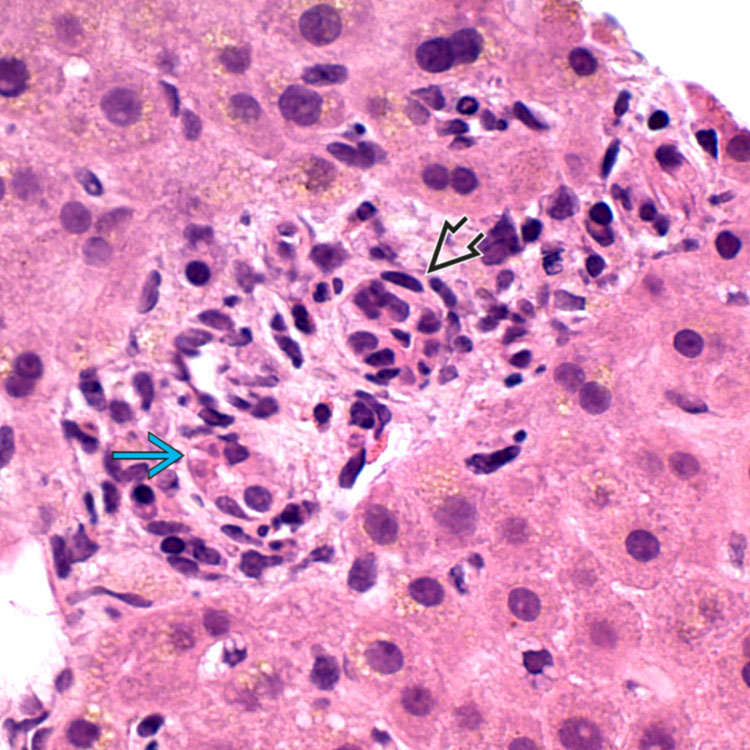
 . One bile duct is also infiltrated by lymphocytes
. One bile duct is also infiltrated by lymphocytes  .
.
 and the mononuclear cell portal infiltrate with admixed eosinophils
and the mononuclear cell portal infiltrate with admixed eosinophils  .
.
 surrounded by mononuclear cells.
surrounded by mononuclear cells.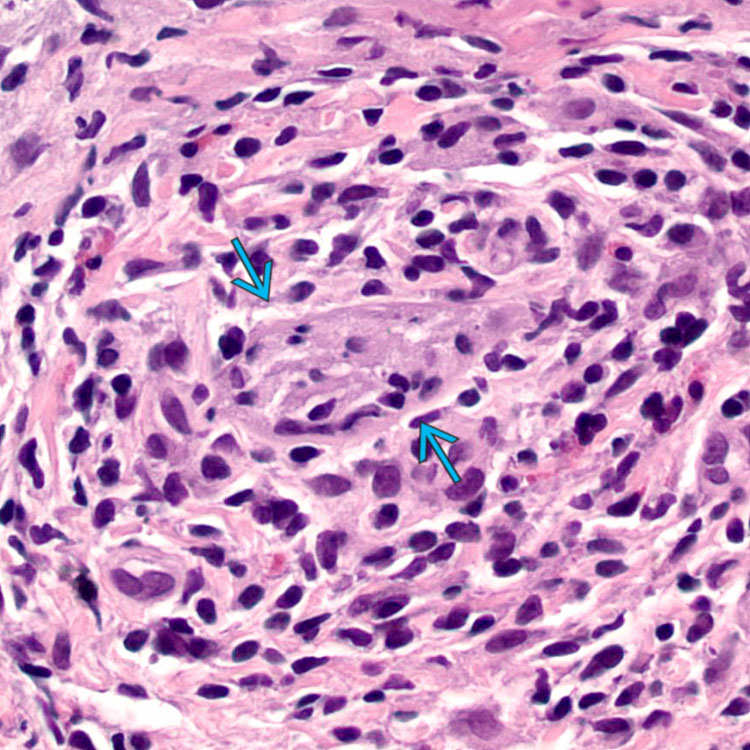
 and a predominantly mononuclear portal inflammatory infiltrate.
and a predominantly mononuclear portal inflammatory infiltrate.