Published on 19/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 2773 times
Neil H. Shear and Sandra R. Knowles
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
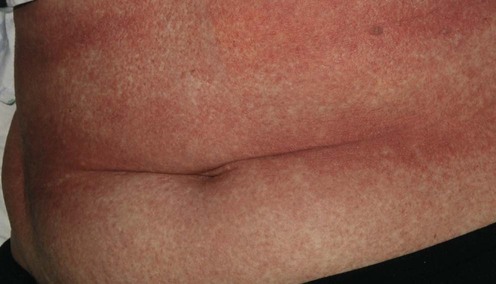
Drug eruptions are common drug-induced diseases, often with a known etiology but a poorly understood pathogenesis. Most cutaneous reactions are broadly classified as either allergic (immunologic) or idiosyncratic. Drug eruptions can range from a mild, simple exanthematous eruption to severe eruptions with systemic involvement, such as toxic epidermal necrolysis. The image above shows a widespread exanthematous eruption. This can be localized to skin or, in the presence of fever, may be part of a systemic reaction.
There are two steps in diagnosing drug eruptions. First, determine the morphology, e.g., exanthematous (‘maculopapular eruption’ – the most common), urticarial, blistering, or pustular. Second, look for signs of systemic involvement, such as fever, lymphadenopathy, or malaise. Examples of simple eruptions without systemic disease are maculopapular eruption, urticaria, fixed drug eruption, and drug-induced acne. Examples of complex eruptions with systemic disease are drug rash eosinophilia systemic syndrome (DRESS, also known as hypersensitivity drug reaction), serum sickness-like reaction, Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), and acute generalized exanthematous pustulosis (AGEP).
After a diagnosis is considered, it is important to try and identify the relevant drug exposure, consider a differential diagnosis, and remember that each drug exposure has a possible etiologic role. In general, most drug eruptions occur within 3 months of starting therapy, although some eruptions can develop after 1 to 2 years (e.g., drug-induced lupus).
Treatment involves stopping drugs that have a high probability of being the cause, while providing supportive therapy for symptoms. Laboratory investigations may identify internal organ toxicity, and systemic therapy may be considered. The patient should be advised of the interpretation of the adverse event, what drugs were likely causes, whether tests will help confirm the cause, and what drugs should be avoided in the future. For severe reactions relatives may need to be informed, because some systemic reactions (e.g., DRESS, TEN) have a genetic susceptibility.
Genetic testing (prior to initiation of therapy)
Skin biopsy
Vital signs
Hematologic profile
Liver enzymes
Urinalysis
Drug allergy testing (skin testing, patch testing) and drug challenge in carefully selected cases
Chung W, Hung S, Chen Y. Expert Opin Drug Saf 2010; 9: 15–21.
A strong association of HLA-B*1502 with carbamazepine-induced SJS/TEN has been reported in southeast Asian patients. Although the evidence is limited, it is recommended that clinicians avoid phenytoin and fosphenytoin as alternatives to carbamazepine in patients who test positive for the HLA-B*1502 allele.
The FDA in the US, as well as several other regulatory agencies, have included information in the product monograph that states that patients should be screened for HLA-B*1502 allele as well as the HLA-A*3101 allele prior to starting treatment with carbamazepine.
Barbaud A. Immunol Allergy Clin North Am 2009; 29: 517–35.
Skin tests (prick, intradermal tests and patch tests) have been used in the investigation of cutaneous adverse drug reactions. In general, it is recommended that drug skin tests be done within 6 months following the cutaneous adverse drug reaction. Patch tests are of potential value in patients with a history of a maculopapular rash, symmetric drug-related intertriginous and flexural exanthema, AGEP, and fixed drug reaction.
Patch tests and prick tests can be done with any form of the commercialized product, whereas intradermal tests can be done only if an injectable form of the drug is available commercially. A table summarizing the concentrations used for patch testing for various drugs is also included in this article.
Rerkpattanapipat T, Chiriac AM, Demoly P. Drug provocation tests in hypersensitivity drug reactions. Curr Opin Allergy Clin Immunol 2011; 11: 299–304.
Drug provocation testing is used as a tool to evaluate causality in drug-induced eruptions; it is often considered the ‘gold standard’ in the diagnosis of drug hypersensitivity. However, because of the potential risks, it is usually reserved when the implicated drug is required for treatment, alternative test methods have failed and there are no contraindications. Drug provocation tests are used for beta-lactam antibiotics (often in conjunction with negative skin tests), ASA/NSAIDs, glucocorticoids and local anesthetics.
Drug provocation test with the implicated drug is often done, although it can not be recommended for patients with histories of a severe reaction. The clinical question should be ‘What drug can the patient use in the future?’ not ‘What drug caused the reaction?’.
Bernstein I, Li JT, Berstein DI, Hamilton R, Spector SL, Tan R, et al. Ann Allergy Asthma Immunol 2008; 100: S1–S148 (see p. S109–115 for relevant drug testing guidelines).
This document provides guidelines for the management and diagnosis of patients with a history of allergic drug reactions, including cutaneous eruptions. Penicillin and cephalosporins, aspirin and NSAIDs, perioperative anaphylaxis, chemotherapeutics, local anesthetics, corticosteroids, and additives/preservatives are reviewed.
Drake LA, Dinehart SM, Farmer ER, Goltz RW, Graham GF, Hordinsky MK, et al. J Am Acad Dermatol 1996; 35: 458–61.
Treatment for mild cutaneous eruptions includes topical corticosteroids, antihistamines, topical antipruritic agents, baths (with or without additives), and emollients.
Exanthems and urticarial eruptions are often pruritic or burning. Topical corticosteroids and oral antihistamines (either sedating or non-sedating) can reduce symptoms. Febrile symptoms may be helped by ibuprofen. Acetaminophen (paracetamol) could compromise hepatic toxicity, but is often used to treat pyrexia. Clinical trials of therapy for most simple drug eruptions have not been conducted.
In complex reactions, severe discomfort or pending organ failure may require the use of oral corticosteroids. The optimal dose is unknown, but we use 1 mg/kg daily of prednisone to bring the reaction under control, usually within days, and prevent progression. If prednisone is used for complex systemic reactions, it may take months to withdraw the corticosteroid due to flares of symptoms. Without prednisone, the reaction may take weeks to settle.
Wu PA, Balagula Y, Lacouture ME, Anadkat MJ. Curr Opin Oncol 2011; 23: 343–51.
Various cutaneous eruptions, including papulopustular rash (‘acneiform eruption’), xerosis, pruritus, nail, hair and mucosal changes, occur in a large percentage of patients on epidermal growth factor receptor inhibitors. The papulopustular rash ranges from 44% in patients treated with gefinitib to up to 90% in those given cetuximab and panitumumab. The authors recommend starting patients on prophylactic doxycycline or minocycline. When a rash occurs, a mild to moderate corticosteroid is applied.
Despite the common occurrence of drug eruptions with the epidermal growth factor receptor inhibitors, a standardized treatment approach has not been studied. Options for treatment include topical antibiotics, oral antibiotics, topical immunomodulatory agents (e.g., pimecrolimus, tacrolimus), and topical corticosteroids. Although the rash is usually mild, it can lead to drug discontinuation or dose reduction.
Dredge DC, Parsons EC, Carter LP, Staley KJ. Pediatric Neurol 2010; 43: 65–9.
Corticosteroids and intravenous immunoglobulin (IVIG) have been used for treatment of anticonvulsant hypersensitivity syndrome in children and adults.
No randomized trial has compared standard therapy (with or without corticosteroids) to IVIG in the management of patients with DRESS. Controversy exists whether IVIG is beneficial for patients with SJS/TEN.
Valeyrie-Allanore L, Wolkenstein P, Brochard L, Ortonne N, Maitre B, Revuz J, et al. Br J Derm 2010; 163: 847–53.
Death rate and progression of detachment appeared lower than expected in 29 patients with a diagnosis of SJS or TEN who received cyclosporine (3 mg/kg/day for 10 days and tapered over a month). The treatment was well tolerated, although one patient developed complications that resulted in discontinuation of cyclosporine.
Schneck J, Fagot JP, Sekula P, Sassolas B, Roujeau JC, Mockenhaupt M. J Am Acad Dermatol 2008; 58: 33–40.
In this large retrospective study of 281 patients, neither IVIG nor corticosteroids had any significant positive effect on mortality compared with supportive care only. However, a trend for a beneficial effect of corticosteroids was noted.
There is no standardized treatment for patients with SJS/TEN. Previous studies have shown that IVIG can significantly reduce the mortality rate compared to a SCORTEN-predicted mortality rate. However, this study suggests that IVIG may not have a beneficial effect.
Chang YS, Huang FC, Tseng SH, Hsu CK, Ho CL, Sheu HM. Cornea 2007; 26: 123–9.
In this retrospective analysis, 60% of patients with SJS/TEN developed ocular manifestations. Topical antibiotic and corticosteroids and frequent lubrication were the most common treatment modalities. In patients with ocular adhesions, daily lysis, sweeping of the fornix, and debridement were necessary to prevent late complications. Therapeutic soft contact lenses can be tried in cases of persistent corneal epithelial defects.
In TEN it is important to be mindful of ocular scarring. Topical cleansing and use of a glass rod daily to prevent adhesions is very important.
Knowles SR, Dewhurst N, Shear NH. Expert Opin Drug Saf 2012; 11(5): 767–78.
Patients with a history of anticonvulsant hypersensitivity syndrome should be counseled about potentially cross-reacting medications. Family counseling is a critical part of patient management in serious idiosyncratic reactions. The patient should carry a notification of the sensitivity (e.g., a MedicAlert bracelet).
Patients need to have a clear understanding that they have had a drug eruption and the risk of sequelae, the drugs that they need to avoid in future, and the risks of future exposure.
Cernadas JR, Brockow K, Romano A, Aberer W, Torres MJ, Bricher A, et al. Allergy 2010; 65: 1357–66.
Desensitization, or the gradual reintroduction of small doses of the drug at fixed intervals, has been used for various medications, including antibiotics (usually β-lactams), aspirin and NSAIDs and chemotherapeutic agents.
Desensitization, also known as tolerance induction, can be successfully employed for many different reactions. However, patients need to continue the medication for the desensitization to be effective. Once the medication is discontinued, the state of ‘desensitization’ is lost and the patient may react when re-exposed to the offending medication.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us








 Topical corticosteroids
Topical corticosteroids Oral antihistamines
Oral antihistamines Non-steroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs Systemic corticosteroids
Systemic corticosteroids Cyclosporine
Cyclosporine Intravenous immunoglobulin G
Intravenous immunoglobulin G Ocular care
Ocular care Debridement and artificial skin membrane
Debridement and artificial skin membrane Pain control
Pain control Counselling
Counselling Desensitization
Desensitization Inform patient of support groups
Inform patient of support groups