Diuretics
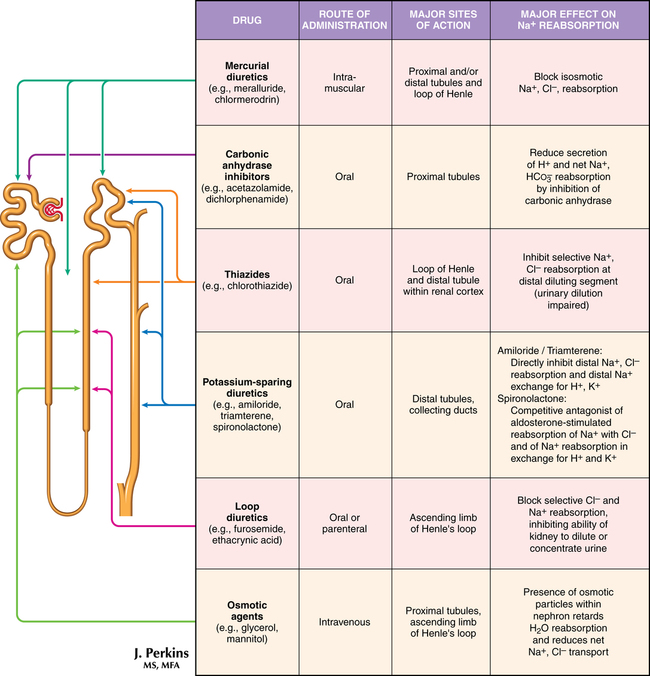
Drugs that increase the excretion of sodium and water through the kidneys, termed diuretics, are classified on the basis of their site (Figure 99-1) or mechanism of action in the nephron. Diuretics are the recommended drugs for initial treatment of hypertension and are used in a variety of relative fluid-overload conditions, including heart failure, renal disease, and liver cirrhosis. Despite the lack of evidence that diuretic therapy prevents acute renal injury or improves outcome following injury or that diuretics reduce morbidity or mortality risk when used in chronic heart failure, they do provide symptomatic relief from fluid-overload syndromes.
 , and
, and  . Cl− excretion exceeds Na+ excretion. Excessive losses of K+, H−,
. Cl− excretion exceeds Na+ excretion. Excessive losses of K+, H−,  , and Cl−, as well as rapid contraction of extracellular fluid volume, may result in metabolic alkalosis.
, and Cl−, as well as rapid contraction of extracellular fluid volume, may result in metabolic alkalosis. is reabsorbed in the proximal tubule via an exchange with H+. Because Na+ is normally reabsorbed in exchange for H+, more Na+ and
is reabsorbed in the proximal tubule via an exchange with H+. Because Na+ is normally reabsorbed in exchange for H+, more Na+ and  remain within the tubules. A diuresis is produced by the Na+ excretion, and the urine is alkaline from the retained
remain within the tubules. A diuresis is produced by the Na+ excretion, and the urine is alkaline from the retained  . Acetazolamide is a weak diuretic because its main action is in the proximal tubule, where only a small percentage of the total filtered Na+ is absorbed.
. Acetazolamide is a weak diuretic because its main action is in the proximal tubule, where only a small percentage of the total filtered Na+ is absorbed.



