Disorders of skin appendages
Non-inflammatory alopecia
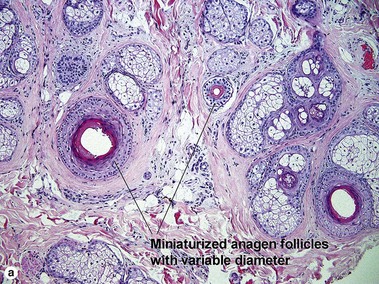

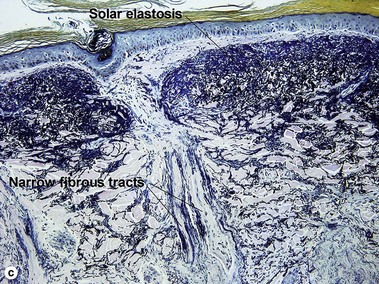
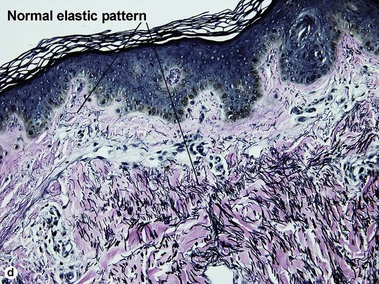
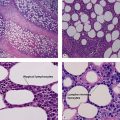
Fig 15-1 (a,b) Pattern alopecia. (c) Solar elastosis and narrow fibrous tract remnants in pattern alopecia (Verhoeff–van Gieson stain). (d) Normal elastic tissue pattern for comparison (Verhoeff–van Gieson stain)

Inflammatory non-scarring alopecia
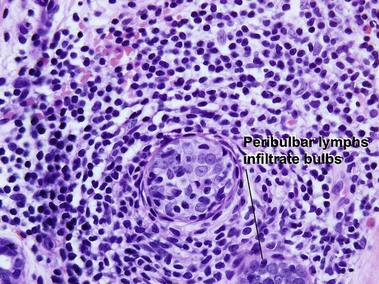
Alopecia areata
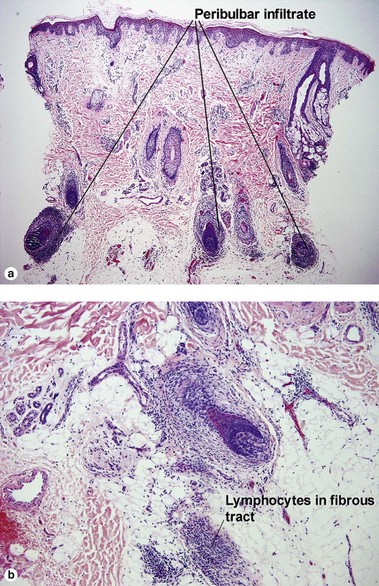
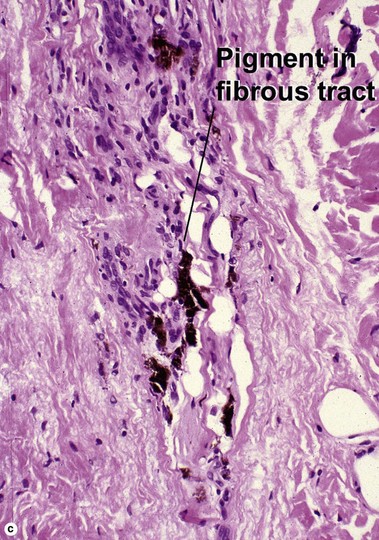
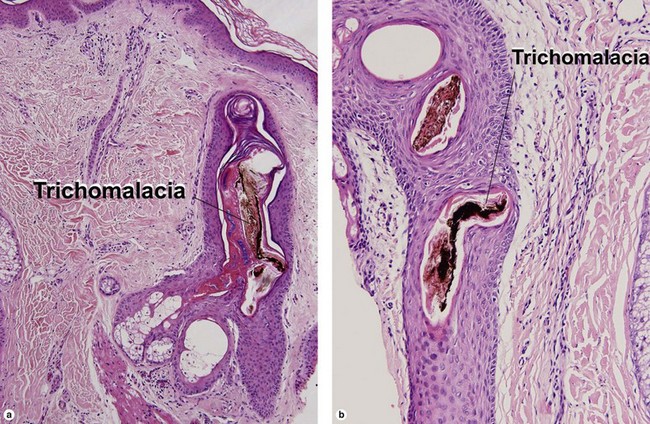
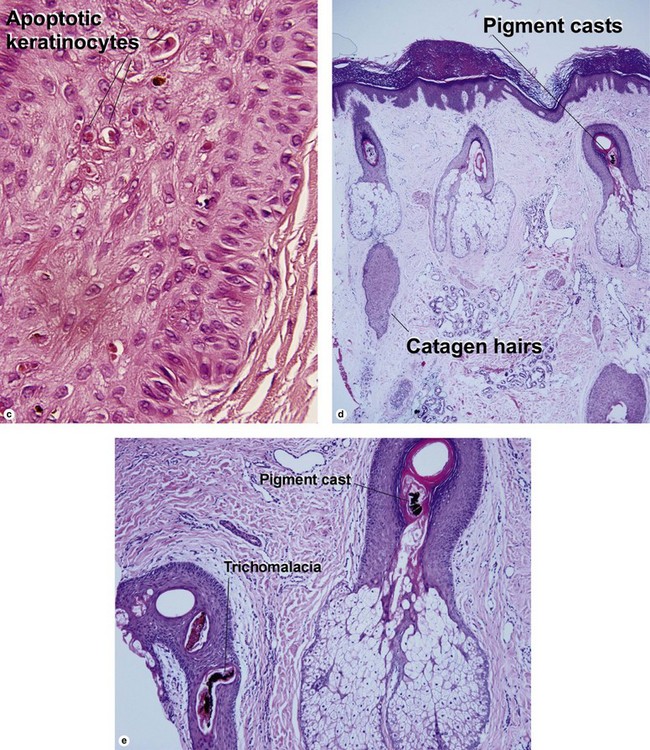
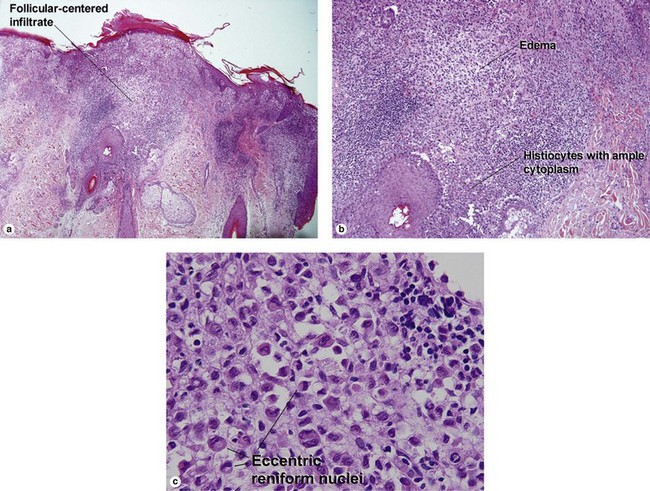
The lymphocytes appear to target melanocytes within the hair bulb. White hairs are spared. The inflammation results in damage to the hair matrix, tapered hair shafts with fracture, and miniaturization of the follicular unit.
Cicatricial alopecia
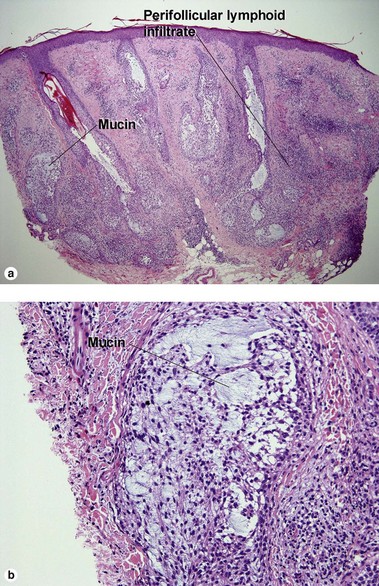
Lupus erythematosus
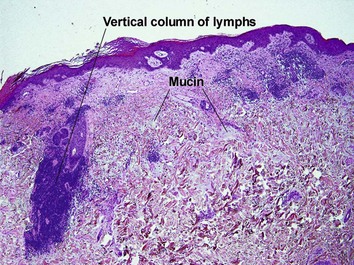
The features of discoid lupus erythematosus appear in a time-dependent fashion. Biopsies of early patches will show only perifollicular mucinous fibrosis and focal interface change. DIF will usually be negative at this stage. The biopsy should always be taken from an active lesion, of at least 3 months’ duration. Burnt-out patches demonstrate scarring throughout the dermis in elastic tissue-stained sections.
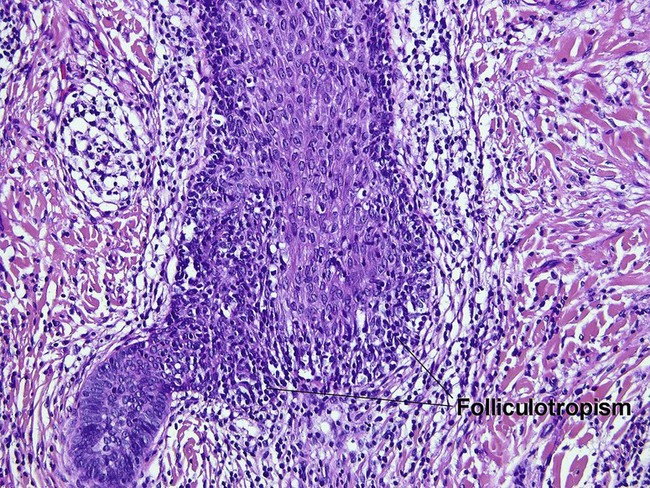
Lichen planopilaris (LPP)
Table 15-2
Characteristics of discoid lupus erythematosus versus lichen planopilaris
| Characteristic | Discoid lupus erythematosus | Lichen planopilaris |
| Hyperkeratosis | Yes | Yes |
| Interface dermatitis | Vacuolar or lichenoid | Lichenoid |
| Pigment incontinence | Yes | Yes |
| Lymphoid infiltrate | Centered at isthmus | Centered at the infundibulum |
| Basement membrane zone thickening | Common | No |
| Dermal mucin | Common | No |
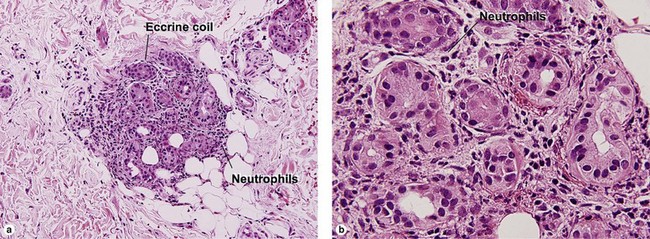
| Lymphocytes in eccrine coil | Common | No |
| Lobular panniculitis with fibrin | Sometimes | No |
| Direct immunofluorescence | “Full house” common in established lesions, may have cytoid bodies | Negative or shaggy fibrin and cytoid bodies |
| Scar in late lesions | Throughout dermis | Superficial wedges |
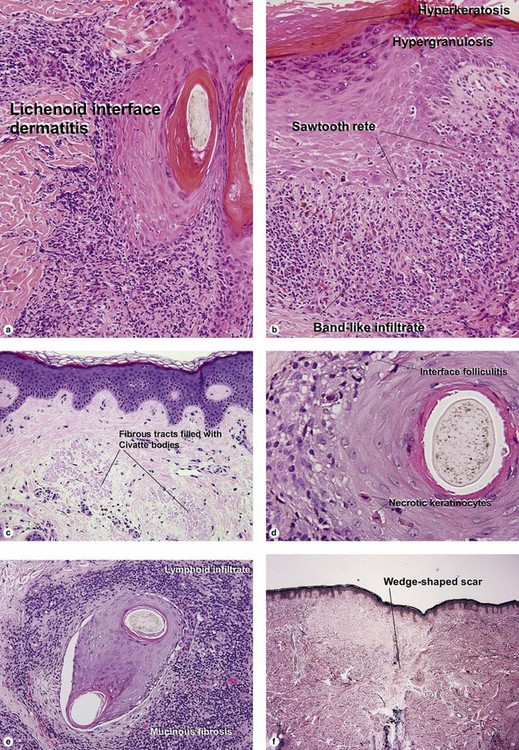
Fig 15-11 (a–e) Lichen planopilaris. (f) Wedge-shaped scar characteristic of lichen planopilaris (Verhoeff–van Gieson stain)
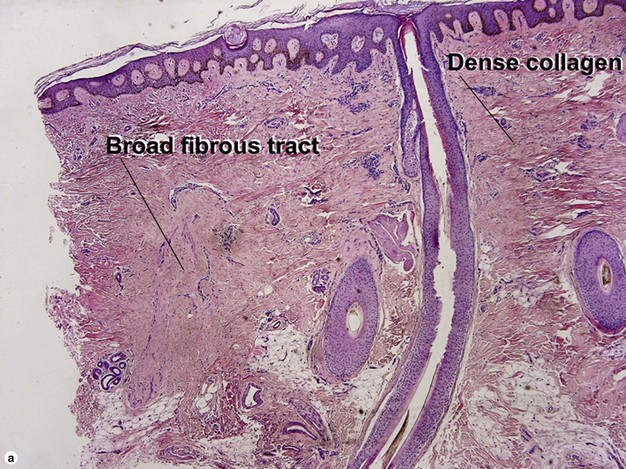

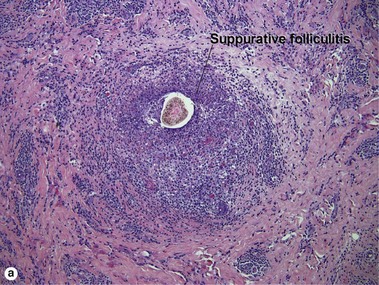

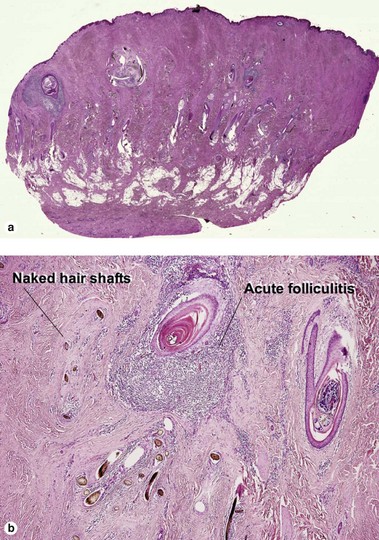
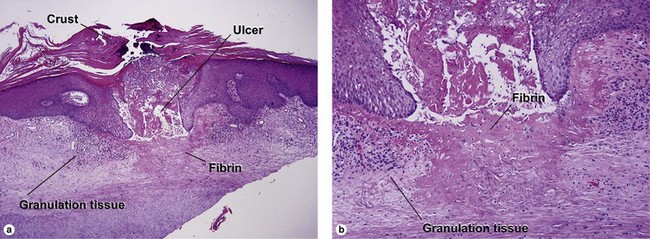
Fig 15-13 (a) Folliculitis decalvans. (b) Wedge-shaped scar of folliculitis decalvans (Verhoeff–van Gieson stain)
As with lupus erythematosus, the features of lichen planopilaris appear in a time-dependent fashion. Biopsies of early patches will show only perifollicular mucinous fibrosis and focal lymphoid inflammation. These changes are most notable about the infundibulum, whereas lupus erythematosus affects the isthmus preferentially. DIF will usually be negative in the early stages, but will often show shaggy linear fibrin and cytoid bodies in more advanced lesions. Burnt-out patches demonstrate wedge-shaped scars at the level of the infundibulum.

Böer, A, Hoene, K. Transverse sections for diagnosis of alopecia? Am J Dermatopathol. 2005; 27(4):348–352.
Childs, JM, Sperling, LC. Histopathology of scarring and nonscarring hair loss. Dermatol Clin. 2013; 31(1):43–56.
Elston, DM. What’s new in the histologic evaluation of alopecia and hair-related disorders? Dermatol Clin. 2012; 30(4):685–694.
Elston, DM. Vertical vs. transverse sections: both are valuable in the evaluation of alopecia. Am J Dermatopathol. 2005; 27(4):353–356.
Elston, DM, Ferringer, T, Dalton, S, et al. A comparison of vertical versus transverse sections in the evaluation of alopecia biopsy specimens. J Am Acad Dermatol. 2005; 53(2):267–272.
Elston, DM, McCollough, ML, Warschaw, KE, et al. Elastic tissue in scars and alopecia. J Cutan Pathol. 2000; 27(3):147–152.
Elston, DM, McCollough, ML, Bergfeld, WF, et al. Eosinophils in fibrous tracts and near hair bulbs: a helpful diagnostic feature of alopecia areata. J Am Acad Dermatol. 1997; 37(1):101–106.
Jackson, AJ, Price, VH. How to diagnose hair loss. Dermatol Clin. 2013; 31(1):21–28.
Olsen, EA, Bergfeld, WF, Cotsarelis, G, et al. Summary of North American Hair Research Society (NAHRS)-sponsored Workshop on Cicatricial Alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003; 48(1):103–110.
Peckham, SJ, Sloan, SB, Elston, DM. Histologic features of alopecia areata other than peribulbar lymphocytic infiltrates. J Am Acad Dermatol. 2011; 65(3):615–620.
Templeton, SF, Santa Cruz, DJ, Solomon, AR. Alopecia: histologic diagnosis by transverse sections. Semin Diagn Pathol. 1996; 13(1):2–18.
Trachsler, S, Trueb, RM. Value of direct immunofluorescence for differential diagnosis of cicatricial alopecia. Dermatology. 2005; 211(2):98–102.
Whiting, DA. Histopathologic features of alopecia areata: a new look. Arch Dermatol. 2003; 139(12):1555–1559.