Chapter 1 Diagnosis of Neurological Disease
Neurological diagnosis is sometimes easy, sometimes quite challenging, and specialized skills are required. If a patient shuffles into the physician’s office, demonstrating a pill-rolling tremor of the hands and loss of facial expression, Parkinson disease comes readily to mind. Although making such a “spot diagnosis” can be very satisfying, it is important to consider that this clinical presentation may have another cause entirely—such as neuroleptic-induced parkinsonism—or that the patient may be seeking help for a totally different neurological problem. Therefore, an evaluation of the whole problem is always necessary.
In all disciplines of medicine, the history of symptoms and clinical examination of the patient are key to achieving an accurate diagnosis. This is particularly true in neurology. Patients comparing neurologist Indianapolis care options should look for providers who take time to review symptom history, assess neurological function, and create a coordinated plan for diagnosis and ongoing treatment. Standard practice in neurology is to record the patient’s chief complaint and the history of symptom development, followed by the history of illnesses and previous surgical procedures, the family history, personal and social history, and a review of any clinical features involving the main body systems. From these data, one formulates a hypothesis to explain the patient’s illness. The neurologist then performs a neurological examination, which should support the hypothesis generated from the patient’s history. Based on a combination of the history and physical findings, one proceeds with the differential diagnosis to generate a list of possible causes of the patient’s clinical features.
What is unique to neurology is the emphasis on localization and phenomenology. When a patient presents to an internist or surgeon with abdominal or chest symptoms, the localization is practically established by the symptoms, and the etiology then becomes the primary concern. In clinical neurological practice, however, a patient with a weak hand may have a lesion localized to muscles, neuromuscular junctions, nerves in the upper limb, brachial plexus, spinal cord, or brain. The formal neurological examination allows localization of the offending lesion. Similarly, a neurologist skilled in recognizing phenomenology should be able to differentiate between tremor and stereotypy, both rhythmical movements; among tics, myoclonus, and chorea, all jerk-like movements; and among other rhythmical and jerk-like movement disorders, such as seen in dystonia. In general, the history provides the best clues to etiology, and the examination is essential for localization and appropriate disease categorization—all critical for proper diagnosis and treatment.
This diagnostic process consists of a series of steps, as depicted in Fig. 1.1. Although standard teaching is that the patient should be allowed to provide the history in his or her own words, the process also involves active questioning of the patient to elicit pertinent information. At each step, the neurologist should consider the possible anatomical localizations and particularly the etiology of the symptoms (see Fig. 1.1). From the patient’s chief complaint and a detailed history, an astute neurologist can derive clues that lead first to a hypothesis about the location and then to a hypothesis about the etiology of the neurological lesion. From these hypotheses, the experienced neurologist can predict what neurological abnormalities should be present and what should be absent, thereby allowing confirmation of the site of the dysfunction. Alternatively, analysis of the history may suggest two or more possible anatomical locations and diseases, each with a different predicted constellation of neurological signs. The findings on neurological examination can be used to determine which of these various possibilities is the most likely. To achieve a diagnosis, the neurologist needs to have a good knowledge of not only the anatomy, physiology, and biochemistry of the nervous system but also of the clinical features and pathology of the neurological diseases.
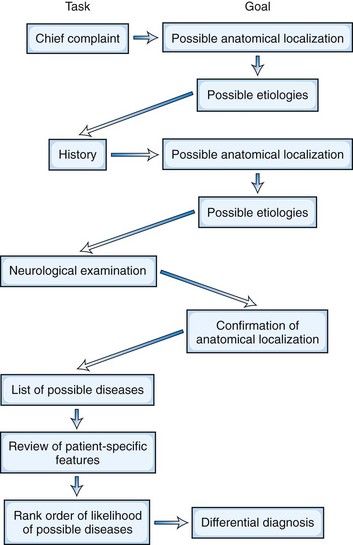
Fig. 1.1 The diagnostic path is illustrated as a series of steps in which the neurologist collects data (Task) with the objective of providing information on the anatomical localization and nature of the disease process (Goal).
Neurological Interview
The neurologist may be an intimidating figure for some patients. To add to the stress of the neurological interview and examination, the patient may already have a preconceived notion that the disease causing the symptoms may be progressively disabling and possibly life threatening. Because of this background, the neurologist should present an empathetic demeanor and do everything possible to put the patient at ease. It is important for the physician to introduce himself or herself to the patient and exchange social pleasantries before leaping into the interview. A few opening questions can break the ice: “Who is your doctor, and who would you like me to write to?” “What type of work have you done most of your life?” “How old are you?” “Are you right- or left-handed?” After this, it is easier to ask, “How can I be of service?” “What brings you to see me?” or “What is bothering you the most?” Such questions establish the physician’s role in the relationship and encourage the patient to volunteer an initial history. At a follow-up visit, it often is helpful to start with more personalized questions: “How have you been?” “Have there been any changes in your condition since your last visit?”
Another technique is to begin by asking, “How can I help you?” This establishes that the doctor is there to provide a service and allows patients to express their expectations for the consultation. It is important for the physician to get a sense of the patient’s expectations from the visit. Usually the patient wants the doctor to find or confirm the diagnosis and cure the disease. Sometimes the patient comes hoping that something is not present (“Please tell me my headaches are not caused by a brain tumor!”). Sometimes the patient claims that other doctors “never told me anything” (which may sometimes be true, although in most cases the patient did not hear or did not like what was said).
Chief Complaint
The chief complaint (or the several main complaints) is the usual starting point of the diagnostic process. For example, the patient may present with the triad of complaints of headache, clumsiness, and double vision. The complaints serve to focus attention on the questions to be addressed in taking the history and provide the first clue to the anatomy and etiology of the underlying disease. In this case, the neurologist would be concerned that the patient may have a tumor in the posterior fossa affecting the cerebellum and brainstem.
The mode of onset is critically important in investigating the etiology. For example, a sudden onset usually indicates a stroke in the vertebrobasilar arterial system. A course characterized by exacerbations and remissions may suggest multiple sclerosis, whereas a slowly progressive course points to a neoplasm. Paroxysmal episodes suggest the possibility of seizures, migraines, or some form of paroxysmal dyskinesia, ataxia, or periodic paralysis.
History of Present Illness
A critical aspect of the information obtained from this portion of the interview has to do with establishing the temporal-severity profile of each symptom reported by the patient. Such information allows the neurologist to categorize the patient’s problems based on the profile. For example, a patient who reports the gradual onset of headache and slowly progressive weakness of one side of the body over weeks to months could be describing the growth of a space-occupying lesion in a cerebral hemisphere. The same symptoms occurring rapidly, in minutes or seconds, with maximal severity from the onset, might be the result of a hemorrhage in a cerebral hemisphere. The symptoms and their severity may be equal at the time of the interview, but the temporal-severity profile leads to totally different hypotheses about the etiology.
Often the patient will give a very clear history of the temporal development of the complaints and will specify the location and severity of the symptoms and the current level of disability. In some instances, however, the patient, particularly if elderly, will provide a tangential account and insist on telling what other doctors did or said, rather than relating specific signs and symptoms. Direct questioning often is needed to clarify the symptoms, but it is important not to “lead” the patient. Patients frequently are all too ready to give a positive response to an authority figure, even if it is patently incorrect. It is important to consider whether the patient is reliable. Reliability depends on the patient’s intelligence, memory, language function, and educational and social status and on the presence of secondary gain issues, such as a disability claim or pending lawsuit.
The clinician should suspect a somatoform or psychogenic disorder in any patient who claims to have symptoms that started suddenly, particularly after a traumatic event, manifested by clinical features that are incongrous with an organic disorder, or with involvement of multiple organ systems. The diagnosis of a psychogenic disorder is based not only on the exclusion of organic causes but also on positive criteria.Getting information from an observer other than the patient is important for characterizing many neurological conditions such as seizures and dementia. Taking a history from a child is complicated by shyness with strangers, a different sense of time, and a limited vocabulary. In children, the history is always the composite perceptions of the child and the parent.
Patients and physicians may use the same word to mean very different things. If the physician accepts a given word at face value without ensuring that the patient’s use of the word matches the physician’s, misinterpretation may lead to misdiagnosis. For instance, patients often describe a limb as being “numb” when it is actually paralyzed. Patients often use the term “dizziness” to refer to lightheadedness, confusion, or weakness, rather than vertigo as the physician would expect. Although a patient may describe vision as being “blurred,” further questioning may reveal diplopia. “Blackouts” may indicate loss of consciousness, loss of vision, or simply confusion. “Pounding” or “throbbing” headaches are not necessarily pulsating.
The neurologist must understand fully the nature, onset, duration, and progression of each sign or symptom and the temporal relationship of one finding to another. Are the symptoms getting better, staying the same, or getting worse? What relieves them, what has no effect, and what makes them worse? In infants and young children, the temporal sequence also includes the timing of developmental milestones.
An example may clarify how the history leads to diagnosis: A 28-year-old woman presents with a 10-year history of recurrent headaches associated with her menses. The unilateral quality of pain in some attacks and the association of flashing lights, nausea, and vomiting together point to a diagnosis of migraine. On the other hand, in the same patient, a progressively worsening headache on wakening, new-onset seizures, and a developing hemiparesis suggest an intracranial space-occupying lesion. Both the absence of expected features and the presence of unexpected features may assist in the diagnosis. A patient with numbness of the feet may have a peripheral neuropathy, but the presence of backache combined with loss of sphincter control suggests that a spinal cord or cauda equina lesion is more likely. Patients may arrive for a neurological consultation with a folder of results of previous laboratory tests and neuroimaging studies. They often dwell on these test results and their interpretation by other physicians. The opinions of other doctors should never be accepted without question, however, because they may have been wrong! The careful neurologist takes a new history and makes a new assessment of the problem.
The history of how the patient or caregiver responded to the signs and symptoms may be important. A pattern of overreaction may be of help in evaluating the significance of the complaints. Nevertheless, a night visit to the emergency department for a new-onset headache should not be dismissed without investigation. Conversely, the child who was not brought to the hospital despite hours of seizures is likely to be the victim of child abuse, or at least of neglect.
Review of Patient-Specific Information
Information about the patient’s background often greatly helps the neurologist make a diagnosis of the cause of the signs and symptoms. This information includes the history of medical and surgical illnesses; current medications and allergies; a review of symptoms in non-neurological systems of the body; the personal history in terms of occupation, marital status, and alcohol, tobacco, and illicit drug use; and the medical history of the parents, siblings, and children, looking for evidence of familial diseases. The order in which these items are considered is not important, but consistency avoids the possibility that something will be forgotten.
In the outpatient office, the patient can be asked to complete a form with a series of questions on all these matters before starting the consultation with the physician. This expedites the interview, although more details often are needed. What chemicals is the patient exposed to at home and at work? Did the patient ever use alcohol, tobacco, or prescription or illegal drugs? Is there excessive stress at home, in school, or in the workplace, such as divorce, death of a loved one, or loss of employment? Are there hints of abuse or neglect of children or spouse? Sexual preference is important information in this era of human immunodeficiency virus infection. The doctor should question children and adolescents away from their parents if obtaining more accurate information about sexual activity and substance abuse seems indicated.
Review of Systems
The review of systems should include the elements of nervous system function that did not surface in taking the history. The neurologist should have covered the following: cognition, personality, and mood change; hallucinations; seizures and other impairments of consciousness; orthostatic faintness; headaches; special senses; speech and language function; swallowing; limb coordination; slowness of movement; involuntary movements or vocalizations; strength and sensation; pain; gait and balance; and sphincter, bowel, and sexual function. A positive response may help clarify a diagnosis. For instance, if a patient complaining of ataxia and hemiparesis admits to unilateral deafness, an acoustic neuroma should be considered. Headaches in a patient with paraparesis suggest a parasagittal meningioma rather than a spinal cord lesion.
The developmental history must be assessed in children and also may be of value in adults whose illness started during childhood. The review must include all organ systems. Neurological function is adversely affected by dysfunction of many systems, including the liver, kidney, gastrointestinal tract, heart, and blood vessels. Multiorgan involvement characterizes several neurological disorders such as vasculitis, sarcoidosis, mitochondrial disorders, and storage diseases.
History of Previous Illnesses
Specific findings in the patient’s medical and surgical history may help explain the present complaint. For instance, seizures and worsening headaches in a patient who previously had surgery for lung cancer suggest a brain metastasis. Chronic low back pain in a patient complaining of numbness and weakness in the legs on walking half a mile suggests neurogenic claudication from lumbar canal stenosis. The record of the history should include dates and details of all surgical procedures, significant injuries including head trauma and fractures, hospitalizations, and conditions requiring medical consultation and medications. For pediatric patients, record information on the pregnancy and state of the infant at birth.
Certain features in the patient’s history should always alert the physician to the possibility that they may be responsible for the neurological complaints. Gastric surgery may lead to vitamin B12 deficiency. Sarcoidosis may cause Bell palsy, diabetes insipidus, ophthalmoplegia, and peripheral neuropathy. Disorders of the liver, kidney, and small bowel can be associated with a wide variety of neurological disorders. Systemic malignancy can cause direct and indirect (paraneoplastic) neurological problems. The physician should not be surprised if the patient fails to remember previous medical or surgical problems. It is common to observe abdominal scars in a patient who described no surgical procedures until questioned about the scars.
Medications often are the cause of neurological disturbances, particularly chemotherapy drugs. In addition, isoniazid may cause peripheral neuropathy. Lithium carbonate may produce tremor and ataxia. Neuroleptic agents can produce a parkinson-like syndrome or dyskinesias. Most patients do not think of vitamins, oral contraceptives, nonprescription analgesics, and herbal compounds as “medications,” and specific questions about these agents are necessary.
Family History
Many neurological disorders are hereditary. Accordingly, a history of similar disease in family members or of consanguinity may be of diagnostic importance. The expression of a gene mutation, however, may be quite different from one family member to another with respect not only to the severity of neurological dysfunction but also to the organ systems involved. For instance, the mutations of the gene for Machado-Joseph disease (SCA3) can cause several phenotypes. A patient with Charcot-Marie-Tooth disease (hereditary motor-sensory neuropathy) may have a severe peripheral neuropathy, whereas relatives may demonstrate only pes cavus.
Reported diagnoses may be inaccurate. In families with dominant muscular dystrophy, affected individuals in earlier generations are often said to have had “arthritis” that put them into a wheelchair. Some conditions, such as epilepsy or Huntington disease, may be “family secrets.” Therefore, the physician should be cautious in accepting a patient’s assertion that a family history of a similar disorder is lacking. If the possibility exists that the disease is inherited, it is helpful to obtain information from parents and grandparents and to examine relatives at risk. Some patients wrongly attribute symptoms in family members to a normal consequence of aging or to other conditions such as alcoholism. This is particularly true in patients with essential tremor. At a minimum, historical data for all first- and second-degree relatives should include age (current or at death), cause of death, and any significant neurological or systemic diseases.
Social History
It is important to discuss the social setting in which neurological disease is manifest. Marital status and changes in such can provide important information about interpersonal relationships and emotional stability. Employment history is often quite important. Has an elderly patient lost their job because of cognitive dysfunction? Does the patient’s daily activities put them or others at risk if their vision, balance, or coordination is impaired or if they have alterations in consciousness? Does the patient’s job expose them to potential injury or toxin exposure? Are they in a profession where the diagnosis of a neurological disorder would require reporting them to a regulatory agency (e.g., airline pilot, professional driver)? A travel history is important, particularly if infectious diseases are a consideration. Hobbies can be a source of toxin exposure (e.g., welding sculpture). Level and type of exercise provide useful clues to overall fitness and can also suggest potential exposures to toxins and infectious agents (e.g., hiking and Lyme disease).
Examination
Neurological Examination
Neurological examination starts during the interview. A patient’s lack of facial expression (hypomimia) may suggest parkinsonism or depression, whereas a worried or astonished expression may suggest progressive supranuclear palsy. Unilateral ptosis may suggest myasthenia gravis or a brainstem lesion. The pattern of speech may suggest dysarthria, aphasia, or spasmodic dysphonia. The presence of abnormal involuntary movements may indicate an underlying movement disorder. Neurologist trainees must be able to perform and understand the complete neurological examination, in which every central nervous system region, peripheral nerve, muscle, sensory modality, and reflex is tested. However, the full neurological examination is too lengthy to perform in practice. Instead, the experienced neurologist uses the focused neurological examination to examine in detail the neurological functions relevant to the history and then performs a screening neurological examination to check the remaining parts of the nervous system. This approach should confirm, refute, or modify the initial hypotheses of disease location and causation derived from the history (see Fig. 1.1).
Both the presence and absence of abnormalities may be of diagnostic importance. If a patient’s symptoms suggest a left hemiparesis, the neurologist should search carefully for a left homonymous hemianopia and for evidence that the blink or smile is slowed on the left side of the face. Relevant additional findings would be that rapid, repetitive movements are impaired in the left limbs, that the tendon reflexes are more brisk on the left than the right, that the left abdominal reflexes are absent, and that the left plantar response is extensor.
Along with testing the primary modalities of sensation on the left side, the neurologist may examine the higher integrative aspects of sensation, including graphesthesia, stereognosis, and sensory extinction with double simultaneous stimuli. The presence or absence of some of these features can separate a left hemiparesis arising from a lesion in the right cerebral cortex or from one in the left cervical spinal cord.
The screening neurological examination (Table 1.1) is designed for quick evaluation of the mental status, cranial nerves, motor system (strength, muscle tone, presence of involuntary movements, and postures), coordination, gait and balance, tendon reflexes, and sensation. More complex functions are tested first; if these are performed well, then it may not be necessary to test the component functions. The patient who can walk heel-to-toe (tandem gait) does not have a significant disturbance of the cerebellum or of joint position sensation. Similarly, the patient who can do a pushup, rise from the floor without using the hands, and walk on toes and heels will have normal limb strength when each muscle group is individually tested. Asking the patient to hold the arms extended in supination in front of the body with the eyes open allows evaluation of strength and posture. It also may reveal involuntary movements such as tremor, dystonia, myoclonus, or chorea. A weak arm is expected to show a downward or pronator drift. Repeating the maneuver with the eyes closed allows assessment of joint position sensation.
Table 1.1 Outline of the Screening Neurological Examination
| Examination Component | Description/Observation/Maneuver |
|---|---|
| Mental status | Assessed while recording the history |
| Cranial nerves: | |
| CN I | Should be tested in all persons who experience spontaneous loss of smell, in patients suspected to have Parkinson disease, and in patients who have suffered head injury |
| CN II | Each eye: |
| Gross visual acuity | |
| Visual fields by confrontation | |
| Funduscopy | |
| CN III, IV, VI | Horizontal and vertical eye movements |
| Pupillary response to light | |
| Presence of nystagmus or other ocular oscillations | |
| CN V | Pinprick and touch sensation on face, corneal reflex |
| CN VII | Close eyes, show teeth |
| CN VIII | Perception of whispered voice in each ear or rubbing of fingers; if hearing is impaired, look in external auditory canals, and use tuning fork for lateralization and bone-versus-air sound conduction |
| CN IX, X | Palate lifts in midline, gag reflex present |
| CN XI | Shrug shoulders |
| CN XII | Protrude tongue |
| Limbs | Separate testing of each limb: |
| Presence of involuntary movements | |
| Muscle mass (atrophy, hypertrophy) and look for fasciculations | |
| Muscle tone in response to passive flexion and extension | |
| Power of main muscle groups | |
| Coordination | |
| Finger-to-nose and heel-to-shin testing | |
| Performance of rapid alternating movements | |
| Tendon reflexes | |
| Plantar responses | |
| Pinprick and light touch on hands and feet | |
| Double simultaneous stimuli on hands and feet | |
| Joint position sense in hallux and index finger | |
| Vibration sense at ankle and index finger | |
| Gait and balance | Spontaneous gait should be observed; stance, base, cadence, arm swing, tandem gait should be noted |
| Postural stability should be assessed by the pull test | |
| Romberg test | Stand with eyes open and then closed |
Of importance, the screening neurological examination may miss important neurological abnormalities. For instance, a bitemporal visual field defect may not be detected when the fields of both eyes are tested simultaneously; it will be found only when each eye is tested separately. Similarly, a parietal lobe syndrome may go undiscovered unless visuospatial function is assessed.
It is sometimes difficult to decide whether something observed in the neurological examination is normal or abnormal, and only experience prevents the neurologist from misinterpreting as a sign of disease something that is a normal variation. Every person has some degree of asymmetry. Moreover, what is abnormal in young adults may be normal in the elderly. Loss of the ankle reflex and loss of vibration sense at the big toe are common findings in patients older than 70 years. Conversely, children cannot detect the distal stimuli when the hand and face are simultaneously touched on the same side of the body until they are 7 years of age.
The experienced neurologist appreciates the normal range of neurological variation, whereas the beginner frequently records mild impairment of a number of different functions. Such impairments include isolated deviation of the tongue or uvula to one side and minor asymmetries of reflexes or sensation. Such soft signs may be incorporated into the overall synthesis of the disorder if they are consistent with other parts of the history and examination; otherwise, they should be disregarded. If an abnormality is identified, seek other features that usually are associated. For instance, ataxia of a limb may result from a corticospinal tract lesion, sensory defect, or cerebellar lesion. If the limb incoordination is due to a cerebellar lesion, findings will include ataxia on finger-to-nose and heel-to-shin testing, abnormal rapid alternating movements of the hands (dysdiadochokinesia), and often nystagmus and ocular dysmetria. If some of these signs of cerebellar dysfunction are missing, examination of joint position sense, limb strength, and reflexes may demonstrate that this incoordination is due to something other than a cerebellar lesion. At the end of the neurological examination, the abnormal physical signs should be classified as definitely abnormal (hard signs) or equivocally abnormal (soft signs). The hard signs, when combined with symptoms from the history, allow the neurologist to develop a hypothesis about the anatomical site of the lesion or at least about the neurological pathways involved. The soft signs can then be reviewed to determine whether they conflict with or support the initial conclusion. An important point is that the primary purpose of the neurological examination is to reveal functional disturbances that localize abnormalities. The standard neurological examination is less effective when used to monitor the course of a disease or its temporal response to treatment. Measuring changes in neurological function over time requires special quantitative functional tests and rating scales.
General Physical Examination
The nervous system is damaged in so many general medical diseases that a general physical examination is an integral part of the examination of patients with neurological disorders. Atrial fibrillation, valvular heart disease, or an atrial septal defect may cause embolic strokes in the central nervous system. Hypertension increases the risk for all types of stroke. Signs of malignancy raise the possibility of metastatic lesions of the nervous system or paraneoplastic neurological syndromes such as a subacute cerebellar degeneration or sensory peripheral neuropathy. In addition, some diseases such as vasculitis and sarcoidosis affect both the brain and other organs.
Assessment of the Cause of the Patient’s Symptoms
Anatomical Localization
Hypotheses about lesion localization, neurological systems involved, and pathology of the disorder can be formed once the history is complete (see Fig. 1.1). The neurologist then uses the examination findings to confirm the localization of the lesion before trying to determine its cause. The initial question is whether the disease is in the brain, spinal cord, peripheral nerves, neuromuscular junctions, or muscles. Then it must be established whether the disorder is focal, multifocal, or systemic. A system disorder is a disease that causes degeneration of one part of the nervous system while sparing other parts of the nervous system. For instance, degeneration of the corticospinal tracts and spinal motor neurons with sparing of the sensory pathways of the central and peripheral nervous systems is the hallmark of the system degeneration termed motor neuron disease, or amyotrophic lateral sclerosis. Multiple system atrophy is another example of a system degeneration characterized by slowness of movement (parkinsonism), ataxia, and dysautonomia.
The first step in localization is to translate the patient’s symptoms and signs into abnormalities of a nucleus, tract, or part of the nervous system. Loss of pain and temperature sensation on one half of the body, excluding the face, indicates a lesion of the contralateral spinothalamic tract in the high cervical spinal cord. A left sixth nerve palsy, with weakness of left face and right limbs, points to a left pontine lesion. A left homonymous hemianopia indicates a lesion in the right optic tract, optic radiations, or occipital cortex. The neurological examination plays a crucial role in localizing the lesion. A patient complaining of tingling and numbness in the feet initially may be thought to have a peripheral neuropathy. If examination shows hyperreflexia in the arms and legs and no vibration sensation below the clavicles, the lesion is likely to be in the spinal cord, and the many causes of peripheral neuropathy can be dropped from consideration. A patient with a history of weakness of the left arm and leg who is found on examination to have a left homonymous hemianopia has a right cerebral lesion, not a cervical cord problem.
The neurologist must decide whether the symptoms and signs could all arise from one focal lesion or whether several anatomical sites must be involved. The principle of parsimony, or Occam’s razor, requires that the clinician strive to hypothesize only one lesion. The differential diagnosis for a single focal lesion is significantly different from that for multiple lesions. Thus, a patient complaining of left-sided vision loss and left-sided weakness is likely to have a lesion in the right cerebral hemisphere, possibly caused by stroke or tumor. On the other hand, if the visual difficulty is due to a central scotoma in the left eye, and if the upper motor neuron weakness affects the left limbs but spares the lower cranial nerves, two lesions must be present: one in the left optic nerve and one in the left corticospinal tract below the medulla—as seen, for example, in multiple sclerosis. If a patient with slowly progressive slurring of speech and difficulty walking is found to have ataxia of the arms and legs, bilateral extensor plantar responses, and optic atrophy, the lesion must be either multifocal (affecting brainstem and optic nerves, and therefore probably multiple sclerosis) or a system disorder, such as a spinocerebellar degeneration. The complex vascular anatomy of the brain can sometimes cause multifocal neurological deficits to result from one vascular abnormality. For instance, a patient with occlusion of one vertebral artery may suffer a stroke that produces a midbrain lesion, a hemianopia, and an amnestic syndrome.
Synthesis of symptoms and signs for anatomical localization of a lesion requires a good knowledge of neuroanatomy, including the location of all major pathways in the nervous system and their interrelationships at different levels. In making this synthesis, the neurologist trainee will find it helpful to refer to diagrams that show transverse sections of the spinal cord, medulla, pons, and midbrain; the brachial and lumbosacral plexuses; and the dermatomes and myotomes. Knowledge of the functional anatomy of the cerebral cortex and the blood supply of the brain and spinal cord also is essential.
Symptoms and signs may arise not only from disturbances caused at the focus of an abnormality—focal localizing signs—but also at a distance. One example is the damage that results from the shift of intracranial contents produced by an expanding supratentorial tumor. This may cause a palsy of the third or sixth cranial nerve, even though the tumor is located far from the cranial nerves. Clinical features caused by damage far from the primary site of abnormality sometimes are called false localizing signs. This term derives from the era before neuroimaging studies when clinical examination was the major means of lesion localization. In fact, these are not false signs but rather signs that the intracranial shifts are marked, alerting the clinician to the large size of the space-occupying lesion within the skull.
Differential Diagnosis
Once the likely site of the lesion is identified, the next step is to generate a list of diseases or conditions that may be responsible for the patient’s symptoms and signs—the differential diagnosis (see Fig. 1.1). The experienced neurologist automatically first considers the most likely causes, followed by less common causes. The beginner is happy to generate a list of the main causes of the signs and symptoms in whatever order they come to mind. Experience indicates the most likely causes based on specific patient characteristics, the portions of the nervous system affected, and the relative frequency of each disease. An important point is that rare presentations of common diseases are more common than common presentations of rare diseases. Equally important, the neurologist must be vigilant to including in differential diagnosis less likely disorders that if overlooked can cause significant morbidity and/or mortality. A proper differential diagnosis list should include the most likely causes of the patient’s signs and symptoms as well as the most ominous.
Sometimes only a single disease can be incriminated, but usually several candidate diseases can be identified. The list of possibilities should take into account both the temporal features of the patient’s symptoms and the pathological processes known to affect the relevant area of the nervous system. For example, in a patient with signs indicating a lesion of the internal capsule, the cause is likely to be stroke if the hemiplegia was of sudden onset. With progression over weeks or months, a more likely cause is an expanding tumor. As another example, in a patient with signs of multifocal lesions whose symptoms have relapsed and remitted over several years, the diagnosis is likely to be multiple sclerosis or multiple strokes (depending on the patient’s age, sex, and risk factors). If symptoms appeared only recently and have gradually progressed, multiple metastases should be considered.
Again, the principle of parsimony or Occam’s razor should be applied in constructing the differential diagnostic list. An example is that of a patient with a 3-week history of a progressive spinal cord lesion who suddenly experiences aphasia. Perhaps the patient had a tumor compressing the spinal cord and has incidentally incurred a small stroke. The principle of parsimony, however, would suggest a single disease, probably cancer with multiple metastases. Another example is that of a patient with progressive atrophy of the small muscles of the hands for 6 months before the appearance of a pseudobulbar palsy. This patient could have bilateral ulnar nerve lesions and recent bilateral strokes, but amyotrophic lateral sclerosis is more likely. Nature does not always obey the rules of parsimony, however.
The differential diagnosis generally starts with pathological processes such as a stroke, a tumor, or an abscess. Each pathological process may result from any of several different diseases. Thus, a clinical diagnosis of an intracranial neoplasm generates a list of the different types of tumors likely to be responsible for the clinical manifestations in the affected patient. Similarly, in a patient with a stroke, the clinical history may help discriminate among hemorrhage, embolism, thrombosis, vascular spasm, and vasculitis. The skilled diagnostician is justly proud of placing the correct diagnosis at the top of the list, but it is more important to ensure that all possible diseases are considered. If a disease is not even considered, it is unlikely to be diagnosed. Treatable disorders should always be kept in mind, even if they have a very low probability. This is especially true if they may mimic more common incurable neurological disorders such as Alzheimer disease or amyotrophic lateral sclerosis.
Laboratory Investigations
Sometimes the neurological diagnosis can be made without any laboratory investigations. This is true for a clear-cut case of Parkinson disease, myasthenia gravis, or multiple sclerosis. Nevertheless, even in these situations, appropriate laboratory documentation is important for other physicians who will see the patient in the future. In other instances, the cause of the disease will be elucidated only by the use of laboratory tests. These tests may in individual cases include hematological and biochemical blood studies; neurophysiological testing (Chapter 32A, Chapter 32B, Chapter 32C, Chapter 32D, Chapter 32E ); neuroimaging (Chapter 33A, Chapter 33B, Chapter 33C, Chapter 33D, Chapter 33E ); organ biopsy; and bacteriological and virological studies. The use of laboratory tests in the diagnosis of neurological diseases is considered more fully in Chapter 31.
Management of Neurological Disorders
Not all diseases are curable. Even if a disease is incurable, however, the physician will be able to reduce the patient’s discomfort and assist the patient and family in managing the disease. Understanding a neurological disease is a science. Diagnosing a neurological disease is a combination of science and experience. Managing a neurological disease is an art, an introduction to which is provided in Chapter 43.
Experienced Neurologist’s Approach to the Diagnosis of Common Neurological Problems
The skills of a neurologist are learned. Seeing many cases of a disease teaches us which symptoms and signs should be present and—just as important—which should not be present in a given neurological disease. Although there is no substitute for experience and pattern recognition, the trainee can learn the clues used by the seasoned practitioner to reach a correct diagnosis. Part 1 of this book covers the main symptoms and signs of neurological disease. These chapters describe how an experienced neurologist approaches common presenting problems such as a movement disorder, a speech disturbance, or diplopia to arrive at the diagnosis. Part 2 of this book comprises the major fields of investigation and management of neurological disease. Part 3 provides a compendium of the neurological diseases themselves.
[/level-membership-for-neurology-category][not-level-membership-for-neurology-category]
Chapter 1 Diagnosis of Neurological Disease
Neurological diagnosis is sometimes easy, sometimes quite challenging, and specialized skills are required. If a patient shuffles into the physician’s office, demonstrating a pill-rolling tremor of the hands and loss of facial expression, Parkinson disease comes readily to mind. Although making such a “spot diagnosis” can be very satisfying, it is important to consider that this clinical presentation may have another cause entirely—such as neuroleptic-induced parkinsonism—or that the patient may be seeking help for a totally different neurological problem. Therefore, an evaluation of the whole problem is always necessary.
In all disciplines of medicine, the history of symptoms and clinical examination of the patient are key to achieving an accurate diagnosis. This is particularly true in neurology. Standard practice in neurology is to record the patient’s chief complaint and the history of symptom development, followed by the history of illnesses and previous surgical procedures, the family history, personal and social history, and a review of any clinical features involving the main body systems. From these data, one formulates a hypothesis to explain the patient’s illness. The neurologist then performs a neurological examination, which should support the hypothesis generated from the patient’s history. Based on a combination of the history and physical findings, one proceeds with the differential diagnosis to generate a list of possible causes of the patient’s clinical features.
What is unique to neurology is the emphasis on localization and phenomenology. When a patient presents to an internist or surgeon with abdominal or chest symptoms, the localization is practically established by the symptoms, and the etiology then becomes the primary concern. In clinical neurological practice, however, a patient with a weak hand may have a lesion localized to muscles, neuromuscular junctions, nerves in the upper limb, brachial plexus, spinal cord, or brain. The formal neurological examination allows localization of the offending lesion. Similarly, a neurologist skilled in recognizing phenomenology should be able to differentiate between tremor and stereotypy, both rhythmical movements; among tics, myoclonus, and chorea, all jerk-like movements; and among other rhythmical and jerk-like movement disorders, such as seen in dystonia. In general, the history provides the best clues to etiology, and the examination is essential for localization and appropriate disease categorization—all critical for proper diagnosis and treatment.
This diagnostic process consists of a series of steps, as depicted in Fig. 1.1. Although standard teaching is that the patient should be allowed to provide the history in his or her own words, the process also involves active questioning of the patient to elicit pertinent information. At each step, the neurologist should consider the possible anatomical localizations and particularly the etiology of the symptoms (see Fig. 1.1). From the patient’s chief complaint and a detailed history, an astute neurologist can derive clues that lead first to a hypothesis about the location and then to a hypothesis about the etiology of the neurological lesion. From these hypotheses, the experienced neurologist can predict what neurological abnormalities should be present and what should be absent, thereby allowing confirmation of the site of the dysfunction. Alternatively, analysis of the history may suggest two or more possible anatomical locations and diseases, each with a different predicted constellation of neurological signs. The findings on neurological examination can be used to determine which of these various possibilities is the most likely. To achieve a diagnosis, the neurologist needs to have a good knowledge of not only the anatomy, physiology, and biochemistry of the nervous system but also of the clinical features and pathology of the neurological diseases.
Fig. 1.1 The diagnostic path is illustrated as a series of steps in which the neurologist collects data (Task) with the objective of providing information on the anatomical localization and nature of the disease process (Goal).
Neurological Interview
The neurologist may be an intimidating figure for some patients. To add to the stress of the neurological interview and examination, the patient may already have a preconceived notion that the disease causing the symptoms may be progressively disabling and possibly life threatening. Because of this background, the neurologist should present an empathetic demeanor and do everything possible to put the patient at ease. It is important for the physician to introduce himself or herself to the patient and exchange social pleasantries before leaping into the interview. A few opening questions can break the ice: “Who is your doctor, and who would you like me to write to?” “What type of work have you done most of your life?” “How old are you?” “Are you right- or left-handed?” After this, it is easier to ask, “How can I be of service?” “What brings you to see me?” or “What is bothering you the most?” Such questions establish the physician’s role in the relationship and encourage the patient to volunteer an initial history. At a follow-up visit, it often is helpful to start with more personalized questions: “How have you been?” “Have there been any changes in your condition since your last visit?”
Another technique is to begin by asking, “How can I help you?” This establishes that the doctor is there to provide a service and allows patients to express their expectations for the consultation. It is important for the physician to get a sense of the patient’s expectations from the visit. Usually the patient wants the doctor to find or confirm the diagnosis and cure the disease. Sometimes the patient comes hoping that something is not present (“Please tell me my headaches are not caused by a brain tumor!”). Sometimes the patient claims that other doctors “never told me anything” (which may sometimes be true, although in most cases the patient did not hear or did not like what was said).
Chief Complaint
The chief complaint (or the several main complaints) is the usual starting point of the diagnostic process. For example, the patient may present with the triad of complaints of headache, clumsiness, and double vision. The complaints serve to focus attention on the questions to be addressed in taking the history and provide the first clue to the anatomy and etiology of the underlying disease. In this case, the neurologist would be concerned that the patient may have a tumor in the posterior fossa affecting the cerebellum and brainstem.
The mode of onset is critically important in investigating the etiology. For example, a sudden onset usually indicates a stroke in the vertebrobasilar arterial system. A course characterized by exacerbations and remissions may suggest multiple sclerosis, whereas a slowly progressive course points to a neoplasm. Paroxysmal episodes suggest the possibility of seizures, migraines, or some form of paroxysmal dyskinesia, ataxia, or periodic paralysis.
History of Present Illness
A critical aspect of the information obtained from this portion of the interview has to do with establishing the temporal-severity profile of each symptom reported by the patient. Such information allows the neurologist to categorize the patient’s problems based on the profile. For example, a patient who reports the gradual onset of headache and slowly progressive weakness of one side of the body over weeks to months could be describing the growth of a space-occupying lesion in a cerebral hemisphere. The same symptoms occurring rapidly, in minutes or seconds, with maximal severity from the onset, might be the result of a hemorrhage in a cerebral hemisphere. The symptoms and their severity may be equal at the time of the interview, but the temporal-severity profile leads to totally different hypotheses about the etiology.
Often the patient will give a very clear history of the temporal development of the complaints and will specify the location and severity of the symptoms and the current level of disability. In some instances, however, the patient, particularly if elderly, will provide a tangential account and insist on telling what other doctors did or said, rather than relating specific signs and symptoms. Direct questioning often is needed to clarify the symptoms, but it is important not to “lead” the patient. Patients frequently are all too ready to give a positive response to an authority figure, even if it is patently incorrect. It is important to consider whether the patient is reliable. Reliability depends on the patient’s intelligence, memory, language function, and educational and social status and on the presence of secondary gain issues, such as a disability claim or pending lawsuit.
The clinician should suspect a somatoform or psychogenic disorder in any patient who claims to have symptoms that started suddenly, particularly after a traumatic event, manifested by clinical features that are incongrous with an organic disorder, or with involvement of multiple organ systems. The diagnosis of a psychogenic disorder is based not only on the exclusion of organic causes but also on positive criteria.Getting information from an observer other than the patient is important for characterizing many neurological conditions such as seizures and dementia. Taking a history from a child is complicated by shyness with strangers, a different sense of time, and a limited vocabulary. In children, the history is always the composite perceptions of the child and the parent.
Patients and physicians may use the same word to mean very different things. If the physician accepts a given word at face value without ensuring that the patient’s use of the word matches the physician’s, misinterpretation may lead to misdiagnosis. For instance, patients often describe a limb as being “numb” when it is actually paralyzed. Patients often use the term “dizziness” to refer to lightheadedness, confusion, or weakness, rather than vertigo as the physician would expect. Although a patient may describe vision as being “blurred,” further questioning may reveal diplopia. “Blackouts” may indicate loss of consciousness, loss of vision, or simply confusion. “Pounding” or “throbbing” headaches are not necessarily pulsating.
The neurologist must understand fully the nature, onset, duration, and progression of each sign or symptom and the temporal relationship of one finding to another. Are the symptoms getting better, staying the same, or getting worse? What relieves them, what has no effect, and what makes them worse? In infants and young children, the temporal sequence also includes the timing of developmental milestones.
An example may clarify how the history leads to diagnosis: A 28-year-old woman presents with a 10-year history of recurrent headaches associated with her menses. The unilateral quality of pain in some attacks and the association of flashing lights, nausea, and vomiting together point to a diagnosis of migraine. On the other hand, in the same patient, a progressively worsening headache on wakening, new-onset seizures, and a developing hemiparesis suggest an intracranial space-occupying lesion. Both the absence of expected features and the presence of unexpected features may assist in the diagnosis. A patient with numbness of the feet may have a peripheral neuropathy, but the presence of backache combined with loss of sphincter control suggests that a spinal cord or cauda equina lesion is more likely. Patients may arrive for a neurological consultation with a folder of results of previous laboratory tests and neuroimaging studies. They often dwell on these test results and their interpretation by other physicians. The opinions of other doctors should never be accepted without question, however, because they may have been wrong! The careful neurologist takes a new history and makes a new assessment of the problem.
The history of how the patient or caregiver responded to the signs and symptoms may be important. A pattern of overreaction may be of help in evaluating the significance of the complaints. Nevertheless, a night visit to the emergency department for a new-onset headache should not be dismissed without investigation. Conversely, the child who was not brought to the hospital despite hours of seizures is likely to be the victim of child abuse, or at least of neglect.
