Published on 19/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 2552 times
John J. Zone
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
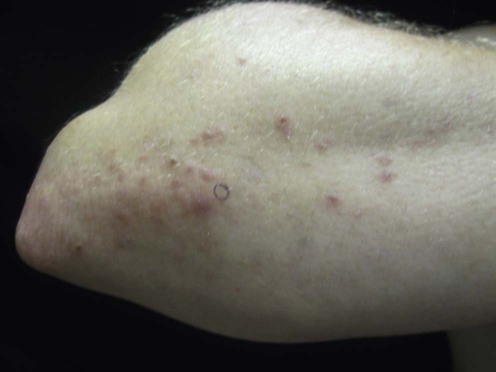
Dermatitis herpetiformis (DH) is a cutaneous manifestation of celiac disease. Rare exceptions have been reported in the Japanese population. More than 85% of patients have an associated gluten-sensitive enteropathy that varies in severity. Both the skin disease and the histological intestinal inflammatory process respond to dietary gluten restriction. DH patients present with a spectrum of severity, ranging from minimal pruritic papules on the elbows and knees to severe, intensely pruritic vesicular lesions over multiple extensor surfaces. The prevalence of DH is approximately 10–39 per 100 000 persons in the Caucasian population. One in six patients diagnosed with celiac disease has DH. DH is distinguished from other bullous diseases by characteristic histologic, immunologic, and associated gastrointestinal findings. Histologically, vesicle formation at the dermal–epidermal junction and infiltration of dermal papillary tips with neutrophils are seen. Direct immunofluorescence shows granular or fibrillar IgA localized in the dermal papillary tips or along the basement membrane of perilesional skin.
The course of DH depends on the therapeutic choices that are made at the time of diagnosis. If patients choose a strict gluten-free diet and adopt a conscientious change in eating habits and lifestyle, they are likely to have a long-term remission and not be bothered by the skin disease. Associated intestinal symptoms are also minimized. In such situations relapses are usually associated with dietary indiscretions. Elevated levels of IgA antibodies to tissue transglutaminase are characteristic of celiac disease, correlate with the degree of intestinal inflammation, and decrease with gluten restriction. Elevated levels of IgA epidermal transglutaminase antibodies are characteristic of DH and are responsible for the diagnostic IgA deposits in skin. If medical therapy with dapsone or sulfapyridine is chosen, the cutaneous lesions can be well controlled. However, attention must be paid to potential side effects of medications. Intestinal symptoms, if present, will continue unabated. Occasionally, some patients (10–20%) will enjoy a spontaneous remission without medication or dietary restriction. The reason for such remission is unclear.
Dapsone is the drug of choice for DH and is currently the only drug approved by the US Food and Drug Administration (FDA) for use in this disease. Initial treatment with dapsone 25 mg daily will usually improve pruritus within 24–48 hours and the papulovesicular lesions within 1 week in adults. Correspondingly smaller doses (0.5–1 mg/kg) should be used in children. Maintenance therapy is then adjusted on a weekly basis to maintain adequate suppression of symptoms. The average maintenance dose is 0.5–1.0 mg/kg daily. Despite adequate dapsone dosages, outbreaks of facial and scalp lesions are common.
Adherence to a gluten-free diet (GFD) improves clinical symptoms in patients with DH. The advantages of gluten restriction include a reduction of dapsone dosage and its attendant complications, improvement of gastrointestinal symptoms (which range from cramping pain to overt diarrhea), and a therapy aimed at the cause rather than the symptoms of the disease. The increased risk of lymphoma incident to DH and celiac disease is also reduced with a GFD, but not with dapsone. Dapsone improves the cutaneous lesions, but has no effect on intestinal disease. Strict adherence to a GFD is, however, challenging, and re-introduction of gluten can exacerbate symptoms of DH. Rare patients will not respond to gluten restriction. It is not possible to predict with certainty which patients will respond to a GFD. In the author’s opinion, a useful therapeutic strategy is the initial control of DH symptoms with dapsone coincident with a GFD with subsequent tapering of dapsone. Oats have been found to be non-toxic in most patients with DH and may broaden the dietary options in an otherwise restrictive GFD.
Sulfapyridine is an alternative choice in patients who are intolerant to dapsone and has been shown to result in significant therapeutic efficacy. Sulfapyridine is started at 500 mg three times a day and is usually increased to a maximum maintenance dose of 1.5 g three times a day.
Other agents that have been reported to have a therapeutic benefit in DH include nicotinamide, tetracycline (or a combination of the two), heparin, cyclosporine, colchicine, and systemic corticosteroids. Topical corticosteroid application is generally inadequate when used alone to control DH symptoms. However, potent corticosteroids in gel form applied frequently may provide relief for occasional lesions that develop on otherwise adequate dapsone or GFD therapy. This allows patients to treat lesions without increasing the dosage of dapsone.
Biopsy for histology and direct immunofluorescence
Complete blood count and liver function tests
Glucose-6-phosphate dehydrogenase levels
IgA tissue transglutaminase antibodies
IgA epidermal transglutaminase antibodies
Zone JJ, Meyer LJ, Petersen MJ. Arch Dermatol 1996; 132: 912–18.
It is accepted that granular IgA deposition in perilesional clinically normal-appearing skin is the most reliable diagnostic criterion for DH. Although the combination of characteristic clinical and pathological features is highly suggestive of DH, the diagnosis of DH should not be made without the identification of granular IgA in dermal papillae. If direct immunofluorescence is negative and histology is suggestive of DH, a repeat biopsy for direct immunofluorescence is recommended.
Bonciani D, Verdelli A, Bonciolini V, et al. Clin Dev Immunol 2012; 2012: 239691.
DH is regarded as a cutaneous manifestation of celiac disease in most cases. The pathogenesis involves an immune response in genetically susceptible individuals (HLA-DQ2 and -DQ8) to dietary gliadin peptides that have been altered by and complexed with tissue transglutaminase (TG2). IgA tissue transglutaminase antibodies are an index of the severity of the intestinal involvement and correlate with response to gluten restriction. IgA epidermal transglutaminase (TG3) antibodies are present in the serum of new DH patients and are complexed with TG3 to form the diagnostic immune complexes in the skin of DH patients.
Wolverton SE, Remlinger K. Dermatol Clin 2007; 25: 195–205.
Dapsone may produce a drug hypersensitivity syndrome with liver toxicity in the first three to 12 weeks. Monitoring of the aspartate transaminase (AST), alanine transaminase (ALT), and eosinophil count is indicated. Hepatocellular toxicity may also occur in a dose-related fashion especially with doses greater than 2 mg/kg. AST and ALT should be monitored when the dosage is increased. There are three main hematologic toxicities of dapsone: hemolysis, methoglobinemia and agranulocytosis. Methoglobinemia is usually mild and not problematic unless the patient has underlying cardiopulmonary problems. Agranulocytosis is rare and usually occurs in the first three to 12 weeks of therapy. Symptoms demanding attention include pharyngitis, fever, and oral ulcerations. Virtually all patients have at least some degree of hemolysis and a fall of the hemoglobin of 1–3 g/dL is to be expected. A compensatory reticulocytosis occurs and may be monitored with a reticulocyte count. Hemolysis may be severe in patients with glucose-6-phosphate dehydrogenase deficiency. Glucose-6-phosphate dehydrogenase levels should be evaluated in blacks and those of Southern Mediterranean origin prior to the initiation of therapy to avoid potentially catastrophic hemolytic anemia.
Complete blood count and liver function tests should be checked every 2 to 3 weeks for the first 3 months and then every 3 to 6 months thereafter.
Niewinski MN. J Am Dietet Assoc 2008; 108: 661–72.
This review focuses in detail on the GFS and the importance of expert dietary counseling for patients with celiac disease. Recent advances in the GFD include food allergen labeling as well as the FDA’s proposed definition of the food-labeling term gluten free. The GFD is complex and patients need comprehensive nutrition education from a skilled dietitian. Support groups are also helpful.
Nino M, Ciacci C, Delfino M. J Dermatolog Treat 2007; 18: 10–12.
This study evaluated the efficacy of treating severe skin manifestations of DH with a GFD alone and compared the results to treatment with GFD and dapsone. Eighty-seven percent of patients on GFD alone had a complete remission in 18 months (67% of severe patients). A total of 89% of patients on diet and dapsone had remission of skin disease (70% of severe patients) and 11% were improved.
Cardones AR, Hall RP. Immunol Allergy Clin North Am 2012; 32: 275–81.
Sulfapyridine is not readily available in the US, but can be prescribed through compounding pharmacies. Sulfasalazine, which is more readily available, is metabolized to 5-amino-salicylic acid and sulfapyridine. Patients have been reported to respond to sulfasalazine, 2–4 g/day administered twice daily.
Kadunce DP, McMurry MP, Avots-Avotins A, Chandler JP, Meyer LJ, Zone JJ. J Invest Dermatol 1991; 97: 175–82.
In severe refractory cases of DH elemental diet therapy is effective and produces dramatic clinical improvement within 2 to 4 weeks. It involves the ingestion of amino acid and carbohydrate alone and is commercially available as Vivonex. It produces rapid healing of the intestine and relief of cutaneous symptoms but was designed for tube feeding and is considered unpalatable by many.
In this author’s experience, elemental diet containing short chain polypeptides is less effective.
Shah SAA, Ormerond AD. Clin Exp Dermatol 2000; 25: 204–5.
This is a case report of a patient with severe DH who was intolerant to dapsone and sulfapyridine. The DH lesions resolved with combination treatment consisting of subcutaneous low-dose heparin, nicotinamide 1.5 g daily in divided doses, and tetracycline 2 g daily. The patient was, however, on a GFD.
Tan CC, Sale JE, Brammer C, Irons RP, Freeman JG. Dermatology 1996; 192: 185–6.
A patient with severe DH who was intolerant of dapsone and sulfapyridine was treated with parenteral heparin with complete resolution of her skin lesions within 1 week of therapy. This treatment is not practical for long-term management.
Stenveld HJ, Starink TM, van Joost T, Stoof TJ. J Am Acad Dermatol 1993; 28: 1014–15.
Two patients with severe DH who were intolerant and/or unresponsive to conventional therapy were treated with cyclosporine (5–7 mg/kg daily) with resolution of skin lesions.
Lang PG. J Am Acad Dermatol 1985; 13: 513–15.
A patient with DH was treated successfully with a short course of prednisone and remained clear 4 months after discontinuation. He was successfully re-treated with systemic corticosteroids for recurrence of the skin lesions.
Silver DN, Juhlin EA, Berczeller PH, McSorley J. Arch Dermatol 1980; 116: 1373–84.
Oral colchicine resulted in a significant improvement of skin lesions in three of four patients with DH. The authors suggest that colchicine may be used when dapsone or sulfapyridine is contraindicated.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us






 Dapsone
Dapsone Gluten-free diet
Gluten-free diet Sulfapyridine and sulfasalazine
Sulfapyridine and sulfasalazine Elemental diet
Elemental diet Tetracycline and nicotinamide
Tetracycline and nicotinamide Heparin
Heparin Cyclosporine
Cyclosporine Colchicine
Colchicine Systemic corticosteroids
Systemic corticosteroids