Chapter 111 Contraception
Adolescents bear a disproportionate risk of the adverse consequences of sexual activity, sexually transmitted infections (STIs) (Chapter 114), and early, unintended pregnancy (Chapter 112). Adolescents often do not seek reproductive health care for 6 to 12 mo after initiating sex; many will become pregnant and/or acquire an STI during this interval. Youth who plan sexual initiation are 75% more likely to use contraception at sexual debut. Early adolescents are concrete thinkers, which may limit their ability to plan; most contraception requires some planning. Appropriate educational interventions with adolescents including the health care provider bringing up the topic of prevention can decrease sexual risk behavior.
Epidemiology
Sexual Activity
The median age at 1st intercourse varies greatly across the globe. Among participants ranging in age from 16 to above 65 yr representing all educational levels from 26 middle- and high-income nations, age of sexual debut was 18.9 yr for women and 19.5 yr for men, with an overall range of 23.0 yr in Malaysia to 17.3 yr in Austria (18.0 yr in the USA) (Fig. 111-1). Among developing nations, there is greater diversity; 73% of Liberian women ages 15-19 yr have had intercourse, compared to 53% of Nigerian, 49% of Ugandan, and 32% of Botswanan women. Only 7% of Chinese university students report being sexually experienced. Among U.S. high schools students in 2007, 7% report having initiated sex before age 13 yr, including 16% of African-American, 8% of Hispanic, and 4% of white youth; 48% of high school students are sexually experienced, including 67% African-American, 52% Hispanic, and 44% white.
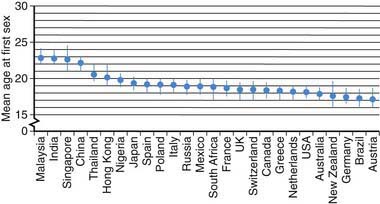
Figure 111-1 Mean age at first sex by country.
(From Durex Network: The face of global sex 2007. First sex: opportunity of a lifetime, Cambridge, UK, 2007, SSL International, p 13. www.durexnetwork.org/en-GB/research/faceofglobalsex/Pages/Home.aspx. Accessed April 22, 2010.)
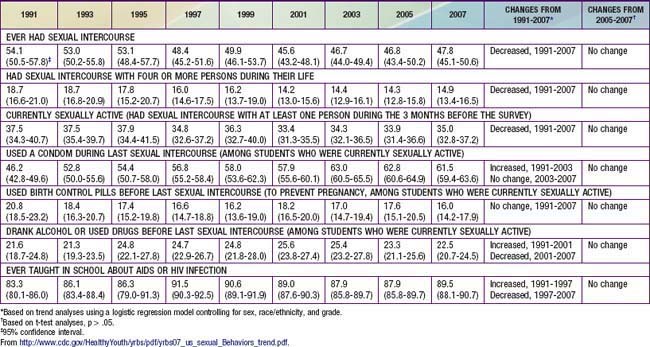
Despite decreases in adverse outcomes of adolescent sexual activity in the USA for the decade at the end of the 20th and beginning of the 21st century, this trend may be reversing. The annual rate of AIDS diagnoses reported among males aged 15-19 yr doubled in the past from 1.3 cases per 100,000 population in 1997 to 2.5 cases in 2006; and rates of gonorrhea and syphilis also increased. Birthrates among adolescents aged 15-19 yr decreased each year from 1991-2005 but increased from 40.5 live births per 1,000 females in 2005 to 42.5 in 2007. The USA has the highest rate of teen pregnancy in the western industrialized world. Of the >750,000 pregnancies among women aged 15-19 yr annually, ~ 80% are unintended (of which 30% are aborted). Consistent with these decreases and subsequent increases in adverse outcomes, the Centers for Disease Control and Prevention “Youth Risk Behavior Survey” reported that among high school students the rate of “ever had intercourse” declined from 54.1% in 1991 to 46.7% in 2005. From 2005 to 2007 there was no further decline; rather, albeit insignificant statistically, all 3 categories of sexual activity (ever had sex, number of partners, currently sexually active) showed increasing trends and both contraception reports (use a condom, use birth control) showed decreasing trends (Table 111-1).
Contraceptive Use
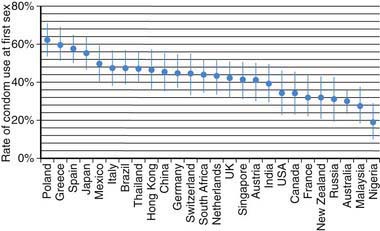
Use of contraception at first sex has increased over the past half-century. Among the residents of 26 middle- and high-income countries listed in Figure 111-2, individuals >65 yr were 8-fold more likely to have used no contraception for their sexual debut, compared to youth currently 16-19 yr of age (among whom 75% used contraception). Females compared to males were 25% more likely to use some form of contraception when they made their sexual debut. Factors increasing the use of contraception at sexual debut include: increasing age among teens up to age 17 yr; spending some time at college; and planning their sexual debut (75% more likely to have used contraception than those who did not plan it). Among U.S. men, data from the National Center for Health Statistics reveals that 48% of those 15-44 yr report using a condom the 1st time they had sex, while 71% of sexually experienced men age 15-19 yr report using a condom the 1st time they have sex. Use of a condom at last episode of intercourse increased from 46% in 1991 to 63% in 2003; in 2007 61.5% reported using a condom; use of birth control pills was 20.8% in 1991 and 16% in 2007 (see Table 111-1). Condoms were the most frequently used method, with dramatic increases from 1995-2002 in non-Hispanic white females (40.8% to 60.8%) and non-Hispanic black males (71% to 86.1%). The type of hormonal method selected also varies by ethnicity, with non-Hispanic white women more likely to select pills (40.7%); black women use pills as the first choice, and use the injectable method twice as much as white women.
Contraceptive Counseling
The health screening interview during the adolescent preventive visit offers the opportunity both to support the adolescent who is abstinent to continue to be so and to identify the sexually active adolescent who has unsafe sexual practices (Chapter 106). Adolescents with chronic diseases are particularly vulnerable to having these issues omitted from the health maintenance visit (Chapter 39). There may be particular cautions related to concurrent medication to be noted for these chronically ill teenagers; sexuality and contraceptive issues do need to be addressed. The goals of a counseling intervention with the adolescent are to understand the adolescent’s perceptions and misperceptions about contraceptives, help him or her put the risk of unprotected intercourse in a personal perspective, and educate the adolescent regarding the real risk and contraindications for the various methods available.
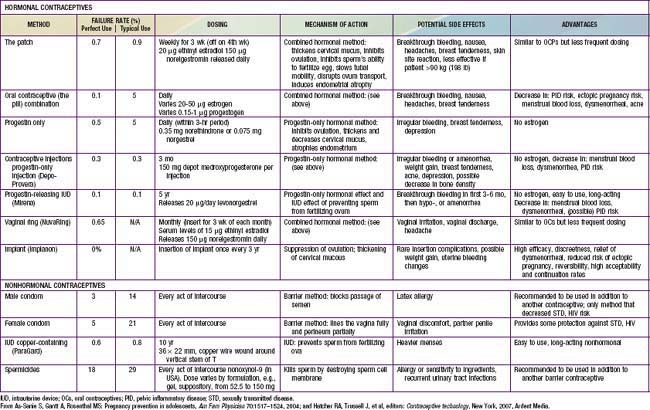
The likelihood that an adolescent will use a contraceptive method depends on such factors as the developmental level of the adolescent, the reproductive history, the involvement in other high-risk behaviors, and the degree of readiness for using contraception. Readiness to use contraception progresses in stages, from (1) precontemplative, not thinking about using contraception; (2) contemplative, giving it some thought, but having no immediate plans; (3) preparative, wanting to try a method in the near future; to (4) active, using contraception. The adolescent should also be made aware of the “perfect” use failure rates versus the “typical” failure rates based on the correct and consistent use of the method (Table 111-2). The pregnancy risk for use of withdrawal as a contraceptive method is probably underestimated in adolescents, and its low efficacy rate should be specifically addressed with young adolescents. Once an adolescent chooses a method, the provider and youth must discuss recognition of the common side effects, with clear plans on management; communication with the provider about the realistic expectation for failure; a contingency plan for that possibility; and strategies for close follow-up (see Table 111-2). A pelvic examination is not required for provision of a contraceptive method. Guidelines from the American College of Obstetrics and Gynecology stipulate that a routine pelvic exam with Pap smear be initiated 3 yr after onset of sexual activity. After this event, annual urine screening for STIs is advised. Confidentiality and consent issues related to contraceptive management are discussed in Chapter 106.
111.1 Barrier Methods
Condoms
This method prevents sperm from being deposited in the vagina. There are no major side effects associated with the use of a condom. The risk of AIDS may have increased the use of condoms among adolescents, with 46.2% of high school students in 1991 reporting using a condom at last sexual intercourse increasing to 61.5% in 2007. Condom use rates vary considerably between countries; condom use at 1st intercourse is higher in many countries compared to the USA (see Fig. 111-2). The main advantages of condoms are their low price, availability without prescription, little need for advance planning, and, most important for this age group, their effectiveness in preventing transmission of STIs, including HIV and human papillomavirus (HPV). Latex condoms are recommended as protection against STIs, to be used along with all nonbarrier medical methods for adolescents. A female condom is available over the counter in single size disposable units. It is a 2nd choice over the male latex condom because of the complexity of properly using the device, its low typical efficacy rate, and the lack of studies in humans demonstrating its effectiveness against STIs. Most adolescents would require intensive education and hands-on practice to use it effectively.
111.4 Hormonal Methods
Combination Oral Contraceptives
The short-term adverse effects of OCs, such as nausea and weight gain, often interfere with compliance in adolescent patients. These effects are usually transient and may be overshadowed by the beneficial effects of a shortened menses and the relief of dysmenorrhea. The inhibition of ovulation or the suppressant effect of estrogens on prostaglandin production by the endometrium makes OCs effective in preventing dysmenorrhea (Chapter 110). An initial thought for younger adolescents regarding the potentially unknown effect of estrogens on epiphyseal growth is no longer a concern. Acne may be worsened by some and improved by other OC preparations. The pills with nonandrogenic progestins are particularly effective in reducing acne and hirsutism. Drospirenone, a progestin with antimineralocorticoid activity, has been shown to reduce premenstrual symptomatology, but the potential for hyperkalemia as a side effect eliminates patients with renal, liver, or adrenal diseases and patients on certain medications. A beneficial cardiovascular effect occurs for adolescents taking estrogen-containing OCs; these young women have higher levels of cardioprotective high-density lipoproteins than controls. Although women <35 yr old who smoke are at less risk of cardiovascular complications, adolescents on OCs should be encouraged to stop smoking.
Contraindications to the use of estrogen-containing OCs include hepatocellular disease, migraine headaches, breast disease, any condition in which hypercoagulability may be a problem (replaced cardiac valve, thrombophlebitis, sickle cell anemia) because of the increased levels of factor VIII and decreased production of antithrombin III, and known or suspected pregnancy (Table 111-3). The risks of pregnancy must be balanced against the benefits of reliable contraception in patients with chronic diseases such as diabetes, epilepsy, and sickle cell disease. The initial history taken before prescribing OCs should specifically address these risks. The World Health Organization ranks multiple medical eligibility criteria for safety with the use of hormonal contraception from 4, precluding use, to 1, conditions raising no concerns, and provides a thorough listing for reference purposes.
Table 111-3 CONTRAINDICATIONS TO COMBINED HORMONAL CONTRACEPTIVES
ABSOLUTE CONTRAINDICATIONS (CLASS 4 IN THE WHO CLASSIFICATION)
RELATIVE CONTRAINDICATIONS (CLASS 2 OR 3 IN THE WHO CLASSIFICATION)
From Amy JJ, Tripathi V: Contraception for women: an evidence based overview, BMJ 339:563–568, 2009.
Missed Contraceptive Pills
The effectiveness of OC is dependent on compliance, and unfortunately adolescent women may forget to take a pill each day. A pill is considered missed if it is 12 hr late from the designated daily time. If 3 pills are missed, back up contraception is required and if intercourse has occurred, emergency contraception (EC) is indicated (Fig. 111-3). Rules for missed pills are noted in Table 111-4.
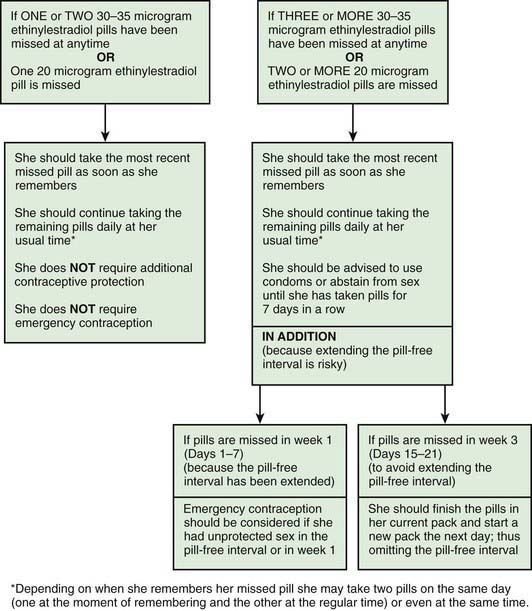
Figure 111-3 Advice for women missing combined oral contraceptives (30-35 µg and 20 µg ethinyl estradiol formulations).
(From Faculty of Family Planning and Reproductive Health Care Effectiveness Unit: FFPRHC Guidance [July 2006]. First prescription of combined oral contraception. The full statement is available at www.ffprhc.org.uk.)
From Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit: Missed pills: new recommendations, April 2005. www.ffprhc.org.uk/admin/uploads/MissedPillRules%20.pdf. Accessed April 23, 2010.
Other Combination Methods
The transdermal patch (Ortho Evra) releases 20 µg ethinyl estradiol and 150 µg norelgestromin daily and is applied to the lower abdomen, buttocks, or upper body. It is worn continuously for 1 wk and changed weekly for a total of 3 wk, then removed to allow menstrual bleeding (see Table 111-2). It should not be applied to the breast. Limited studies in adolescents suggest higher rates of partial or full detachment compared to adults, with high patient satisfaction and 50-83% continuation rates from 3-18 mo of use.
All these methods have contraindications similar to those to oral contraceptives (see Table 111-3).
All-Progestin Contraceptives
An injectable progestin, medroxyprogesterone acetate (Depo-Provera, DMPA), is highly effective as birth control in a dose of 150 mg as a deep intramuscular injection, with failure rates typically at 0.3-0.4% (see Table 111-2). DMPA is particularly attractive for adolescents who have difficulty with compliance, are intellectually impaired, and are chronically ill or have a relative contraindication to estrogen use. Although concern has been directed toward the potential for loss in bone mineral density in adolescents, thereby potentially increasing their risk for osteoporosis later in life, recent studies have found that bone density is recovered after discontinuation of the method. Health care providers may want to consider a contraceptive containing estrogen in teens who are already at high risk for low bone density, such as those who have chronic renal disease, who are wheelchair bound, or who have eating disorders or chronic amenorrhea (Chapter 698).
American Society for Reproductive Medicine Practice Committee. Hormonal contraception: recent advances and controversies. Fertil Steril. 2008;90:S103-S113.
Cromer BA, Scholes D, Berenson A, et al. Depot medroxyprogesterone acetate and bone mineral density in adolescents—the Black Box Warning: a position paper of the Society for Adolescent Medicine. J Adolesc Health. 2006;39:296-301.
Dunn N. Oral contraceptives and venous thromboembolism. BMJ. 2009;339:521-524.
FDA Talk Paper. Black box warning added concerning long-term use of Depo-Provera contraceptive injection. November 17, 2004 www.fda.gov/bbs/topics/ANSWERS/2004/ANS01325.html
Gupta N, Corrado S, Goldstein M. Hormonal contraception in the adolescent. Pediatr Rev. 2008;29:386-396.
Mansour D, Fraser IS. Missed contraceptive pills and the critical pill-free interval. Lancet. 2005;365:1670-1671.
Peterson HB, Curtis KM. Long-acting methods of contraception. N Engl J Med. 2005;353:2169-2175.
Practice Committee of the American Society for Reproductive Medicine. Hormonal contraception: recent advances and controversies. Fertil Steril. 2008;90:S103-S113.
Zhang L, Chen J, Wang Y, et al. Pregnancy outcome after levonorgestrel-only emergency contraception failure: a prospective cohort study. Hum Reprod. 2009;24:1605-1611.
111.5 Emergency Contraception
Unprotected intercourse at mid-cycle carries a pregnancy risk of 20-30%. At other times during the cycle, the risk is 2-4%. The risk may be reduced or eliminated by intervention as soon as possible after unprotected intercourse with a “window” up to 120 hr. Indications for use of emergency contraception are listed in Table 111-5. In 2006, the FDA approved the emergency contraceptive drug Plan B as an over-the-counter option for women aged 18 yr and older. Experience in adolescent women demonstrates more effective use of EC with advance provision and is not associated with more frequent unprotected intercourse or less condom or pill use.
Table 111-5 POTENTIAL INDICATIONS FOR USE OF EMERGENCY CONTRACEPTION
* The usual interval for use of depot medroxyprogesterone acetate as contraception is every 12 wk.
Adapted from Allen RH, Goldberg AB: Emergency contraception: a clinical review, Clin Obstet Gynecol 50:927–936, 2007.
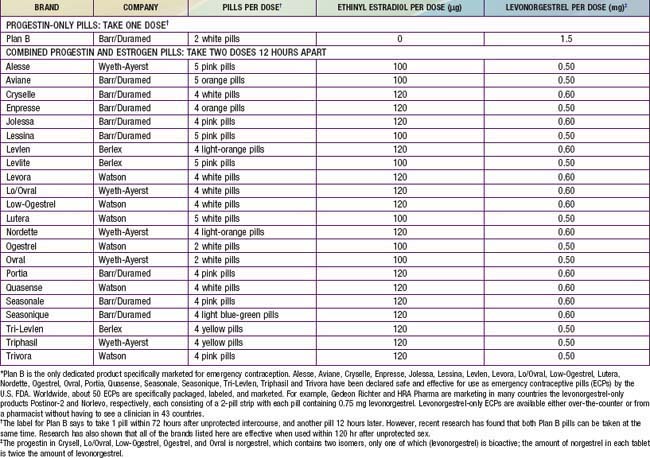
The Yuzpe method is commonly used in the USA, consisting of combination pills totaling 200 µg ethinyl estradiol and 2.0 mg norgestrel or 1.0 mg levonorgestrel. Pills that can be utilized for this method are shown in Table 111-6. The high-dose combination OCs disrupt the luteal phase hormone pattern, creating an unstable and unsuitable uterine lining for implantation. If used mid-cycle, when ovulation is about to occur, the high-dose estrogen and progestin blunt the luteinizing hormone surge and impair ovulation. This method is effective in reducing the risk of pregnancy by 75%. The most common side effects are nausea (50%) and vomiting (20%), prompting some clinicians to prescribe or recommend antiemetics along with the OCs. A urine pregnancy test is usually required prior to dispensing the pills to rule out an existing pregnancy. There is some controversy about the need to do this, since there is no evidence to suggest that OCs used in this manner affect early fetal development and the dose as prescribed would not disrupt a previously undetected pregnancy. The EC kit prepackaged for this method (Preven) was withdrawn from the market in 2004. A progestin-only EC kit was FDA approved in 1999 and contains 2 tablets, each with 0.75 mg levonorgestrel. Nausea and vomiting are uncommon side effects, and in a recent comparison, levonorgestrel proved more effective at preventing pregnancy than the Yuzpe method.
Table 111-6 TWENTY-THREE ORAL CONTRACEPTIVES THAT CAN BE USED FOR EMERGENCY CONTRACEPTION IN THE UNITED STATES*
Allen RH, Goldberg AB. Emergency contraception: a clinical review. Clin Obstet Gynecol. 2007;50:927-936.
American Academy of Pediatrics Committee on Adolescence. Emergency contraception. Pediatrics. 2005;116:1026-1035.
American Academy of Pediatrics Committee on Adolescence. Emergency contraception. Pediatrics. 2005;116:1038-1047.
American College of Obstetricians and Gynecologists. Clinical management guidelines—emergency contraception. Obstet Gynecol. 2005;106:1443-1452.
Prine L. Emergency contraception, myths and facts. Obstet Gynecol Clin North Am. 2007;34:127-136.
American Academy of Pediatrics Committee on Adolescence. Contraception and adolescents. Pediatrics. 2007;120:1135-1148.
Amy JJ, Tripathi V. Contraception for women: an evidence based overview. BMJ. 2009;339:563-568.
Benagiano G, von Hertzen H. Towards more effective emergency contraception? Lancet. 2010;375:527-528.
2011 Centers for Disease Control and Prevention. Contraceptive methods available to patients of office-based physicians and title X clinics—United States, 2009–2010. MMWR. 2011;60(1):104.
Centers for Disease Control and Prevention. U.S medical eligibility criteria for contraceptive use, 2010. MMWR. 59(No. RR-4), 2010.
Centers for Disease Control and Prevention. Sexual and reproductive health of persons aged 10-24 years—United States, 2002-2007. MMWR Morb Mortal Wkly Rep. 2009;58:1-60.
Centers for Disease Control and Prevention. Trends in HIV- and STD-related risk behaviors among high school students—United States, 1991–2007. MMWR Morb Mortal Wkly Rep. 2008;57:817-821.
Darroch JE, Singh SS, Frost JJ, et al. Differences in teenage pregnancy rates among five developed countries: the roles of sexual activity and contraceptive use. Fam Plann Perspect. 2001;33:244-250.
De Irala J, Alonso A. Changes in sexual behaviours to prevent HIV. Lancet. 2006;368:1749-1750.
Duffy K, Wimberly Y, Brooks C. Adolescent contraceptive care for the practicing pediatrician. Adolesc Med State Art Rev. 2009;20:168-187.
Durex Network. The face of global sex 2007. First sex: opportunity of a lifetime. Cambridge, UK Accessed April 23, 2010 www.durexnetwork.org/en-GB/research/faceofglobalsex/Pages/Home.aspx, 2007. SSL International
Grossman D, Holt K, Pena M, et al. Self-induction of abortion among women in the United States. Reprod Health Matters. 2010;18(36):136-146.
Kirby D. Reducing pregnancy and risky behaviour in teenagers. BMJ. 2009;339:116-117.
Manlove J, Ikramullah E, Mincieli L, et al. Trends in sexual experience, contraceptive use, and teenage childbearing: 1992–2002. J Adolesc Health. 2009;44:413-423.
2011 The Medical Letter. Ella: a new emergency contraceptive. Med Lett. 2011;53(1355):3-4.
Monasterio E, Hwang LY, Shafer MA. Adolescent sexual health. Curr Probl Pediatr Adolesc Health Care. 2007;37:302-325.
Paranjothy S, Broughton H, Adappa R, et al. Teenage pregnancy: who suffers? Arch Dis Child. 2009;94:239-245.
Raymond EG, Halpern V, Lopez LM. Pericoital oral contraception with levonorgestrel. Obstet Gynecol. 2011;117(3):673-681.
Santelli JS, Lindberg LD, Finer LB, et al. Explaining recent declines in adolescent pregnancy in the United States: the contribution of abstinence and improved contraceptive use. Am J Public Health. 2007;97:1541-1548.
Shelton JD. Why multiple sexual partners? Lancet. 2009;374:367-368.
Stammers T. Sexual health in adolescents. BMJ. 2007;334:103-104.
Tripp J, Viner R. Sexual health, contraception, and teenage pregnancy. Br Med J. 2005;330:590-593.
World Health Organization. Medical eligibility criteria for contraceptive use. ed 3 www.who.int/reproductive-health/publications/MEC_3/, 2004. Accessed April 23, 2005