[level-membership-for-hematology-oncology-and-palliative-medicine-category]
Chapter 34 Clinical Manifestations, Staging, and Treatment of Follicular Lymphoma
Table 34-1 Initial Evaluation of Follicular Lymphoma
| Stage | Criteria |
|---|---|
| I | Involvement of 1 lymph node (I) or 1 extralymphatic organ or site (IE) |
| II | Involvement of 2 or more lymph nodes on same side of diaphragm (II) or localized extralymphatic organ or site and 1 or more involved lymph node on same side of diaphragm (IIE) |
| III | Involvement of lymph nodes on both sides of diaphragm (III) or same side with localized involvement of extralymphatic site (IIIE), spleen (IIIS), or both (IIIS+E) |
| IV | Diffuse or disseminated involvement of extralymphatic organ or tissues with or without lymph node enlargement |
Table 34-3 Factors Having Prognostic Significance in the FLIPI* and FLIPI2†
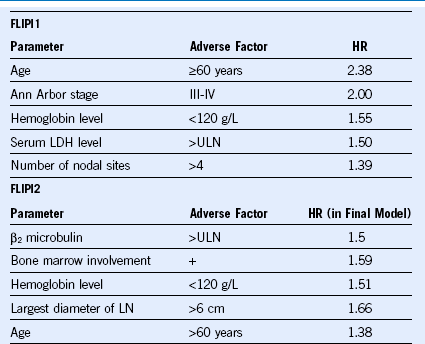
FLIP, Follicular lymphoma international prognostic index; HR, hazard ratio; LDH, lactate dehydrogenase, ULN, upper limit of normal.
Data from Federico M, Bellei M, Marcheselli L, et al: Follicular lymphoma international prognostic index 2: A new prognostic index for follicular lymphoma developed by the international follicular lymphoma prognostic factor project. J Clin Oncol 27:4555, 2009.
Table 34-5 Treatment Strategies for Indolent Lymphomas
| LOCALIZED DISEASE |
| ADVANCED-STAGE DISEASE |
Management of Follicular Lymphoma
Table 34-6 National LymphoCare Study Survey of Current Practice for Follicular Lymphoma in the United States, 2004 to 2007
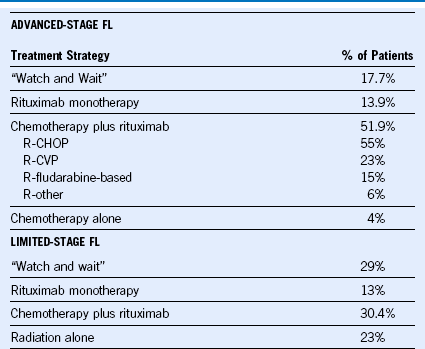
Data from Friedberg JW, Taylor MD, Cerhan JR, et al: Follicular lymphoma in the United States: First report of the national LymphoCare study. J Clin Oncol 27:1202, 2009.
| CVP (EVERY 21 DAYS) |
| CHOP (EVERY 21 DAYS) |
|
• cyclophosphamide 750 mg/m2 IV on day 1 • hydroxydaunomycin 50 mg/m2 IV on day 1 • vincristine (Oncovin) 1.4 mg/m2, up to a maximal dose of 2 mg IV, on day 1 • prednisone 100 mg daily orally on days 1 to 5 Patients being treated with R-CHOP also received 375 mg/m2 of rituximab IV on day 1 of each therapy cycle2 or by alternate schedule.3 |
| CNOP (EVERY 21 DAYS) |
• rituxumab 375 mg/m2 IV on day 1
• methotrexate 200 mg/m2 IV over 2 hours, followed by 800 mg/m2 IV continuous infusion over 22 hours on day 2
• leucovorin 50 mg PO starting 12 hours after completion of methotrexate infusion, followed by 15 mg PO every 6 hours for 8 dosed until the methotrexate level is less than 0.1 µM/L
• cytarabine 3000 mg/m2 IV over 2 hours every 12 hours on days 3 and 4 (4 doses total)
1 Marcus R, Imrie K, Belch A, et al. CVP chemotherapy plus rituximab compared with CVP as first-line treatment for advanced follicular lymphoma. Blood. 2005;105:1417.
2 Hiddemann W, Kneba M, Dreyling M, et al. Frontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) significantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: results of a prospective randomized study of the German Low-Grade Lymphoma Study Group. Blood. 2005;106:3725.
3 Czuczman MS, Grillo-Lopez AJ, White CA, et al. Treatment of patients with low-grade B-cell lymphoma with the combination of chimeric anti-CD20 monoclonal antibody and CHOP chemotherapy. J Clin Oncol. 1999;17:268.
4 Sebban C, Mounier N, Brousse N, et al. Standard chemotherapy with interferon compared with CHOP followed by high-dose therapy with autologous stem cell transplantation in untreated patients with advanced follicular lymphoma: the GELF-94 randomized study from the Groupe d’Etude des Lymphomes de l’Adulte (GELA). Blood. 2006;108:2540.
5 Romaguera JE, Fayad L, Rodriguez MA, et al. High rate of durable remissions after treatment of newly diagnosed aggressive mantle-cell lymphoma with rituximab plus hyper-CVAD alternating with rituximab plus high-dose methotrexate and cytarabine. J Clin Oncol. 2005;23:7013.
[/level-membership-for-hematology-oncology-and-palliative-medicine-category][not-level-membership-for-hematology-oncology-and-palliative-medicine-category]
Chapter 34 Clinical Manifestations, Staging, and Treatment of Follicular Lymphoma
Table 34-1 Initial Evaluation of Follicular Lymphoma
| Stage | Criteria |
|---|---|
| I | Involvement of 1 lymph node (I) or 1 extralymphatic organ or site (IE) |
| II | Involvement of 2 or more lymph nodes on same side of diaphragm (II) or localized extralymphatic organ or site and 1 or more involved lymph node on same side of diaphragm (IIE) |
| III | Involvement of lymph nodes on both sides of diaphragm (III) or same side with localized involvement of extralymphatic site (IIIE), spleen (IIIS), or both (IIIS+E) |
| IV | Diffuse or disseminated involvement of extralymphatic organ or tissues with or without lymph node enlargement |
Table 34-3 Factors Having Prognostic Significance in the FLIPI* and FLIPI2†
FLIP, Follicular lymphoma international prognostic index; HR, hazard ratio; LDH, lactate dehydrogenase, ULN, upper limit of normal.
Data from Federico M, Bellei M, Marcheselli L, et al: Follicular lymphoma international prognostic index 2: A new prognostic index for follicular lymphoma developed by the international follicular lymphoma prognostic factor project. J Clin Oncol 27:4555, 2009.
[/not-level-membership-for-hematology-oncology-and-palliative-medicine-category]
