Chapter 624 Childhood Glaucoma
Primary glaucoma indicates that the cause is an isolated anomaly of the drainage apparatus of the eye (trabecular meshwork). More than 50% of infantile glaucoma is primary. In secondary glaucoma, other ocular or systemic abnormalities are associated, even if a similar developmental defect of the trabecular meshwork is also present. Primary infantile glaucoma occurs with an incidence of 0.03% (see Table 624-1 on the Nelson Textbook of pediatrics website at www.expertconsult.com).
Table 624-1 PRIMARY AND SECONDARY CHILDHOOD GLAUCOMAS
I.PRIMARY GLAUCOMAS
II.SECONDARY GLAUCOMAS
Adapted from Nelson LB: Harley’s pediatric ophthalmology, ed 4, Philadelphia, 1998, WB Saunders, p 294.
Clinical Manifestations
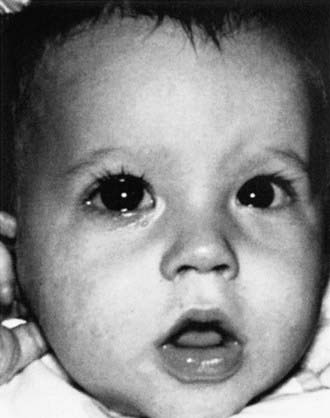
The symptoms of infantile glaucoma include the classic triad of epiphora (tearing), photophobia (sensitivity to light), and blepharospasm (eyelid squeezing) (Fig. 624-1). Each can be attributed to corneal irritation. Only about 30% of affected infants demonstrate the classic symptom complex. Signs of glaucoma include corneal edema, corneal and ocular enlargement, and conjunctival injection (Fig. 624-2).

Beck AD, Freedman S, Kammer J, et al. Aqueous shunt devices compared with trabeculectomy with mitomycin-C for children in the first two years of life. Am J Ophthalmol. 2003;136:994-1000.
Carter BC, Plager DA, Neely DE, et al. Endoscopic diode laser cyclophotocoagulation in the management of aphakic and pseudophakic glaucoma in children. J AAPOS. 2007;11:34-40.
Chen TC, Walton DS, Bhatia LS. Aphakic glaucoma after congenital cataract surgery. Arch Ophthalmol. 2004;122:1819-1825.
Coppens G, Stalmans I, Zeyen T, Casteels I. The safety and efficacy of glaucoma medication in the pediatric population. J Pediatr Ophthalmol Strabismus. 2009;46:12-18.
Morad Y, Donaldson CE, Kim YM, et al. The Ahmed drainage implant in the treatment of pediatric glaucoma. Am J Ophthalmol. 2003;135:821-829.
Sidoti PA, Belmonte SJ, Liebmann JM, et al. Trabeculectomy with mitomycin-C in the treatment of pediatric glaucomas. Ophthalmology. 2000;107:422-429.
Simon JW, Mehta N, Simmons ST, et al. Glaucoma after pediatric lensectomy/vitrectomy. Ophthalmology. 1991;98:670-674.





