Chapter 82 Cervical Spondylosis
Cervical spondylosis is a ubiquitous degenerative process of aging that can lead to both pain and neurologic impairment. Radiographically, it is observed in about 10% of people by age 25 and in nearly 95% by age 65.1,2 Multiple authors near the end of the 19th century initially described it as an inflammatory process, possibly infectious in origin, and, therefore, referred to it as cervical spondylitis3 It was not until 1952 that Brain identified this as a degenerative process of aging and coined the term cervical spondylosis. British neurosurgeon Victor Horsley provided the first description of an operation—a C6 laminectomy—for a patient with progressive spastic quadriparesis with presumed cervical spondylotic myelopathy (CSM).4,5
Pathology of Cervical Spondylosis and Myelopathy
Degeneration associated with spondylosis begins at the intervertebral disc, unlike degenerative arthritis, which is associated with inflammation of the synovial lining of joints.1 The nucleus pulposus consists of proteoglycan aggregates that have hydrophilic hyaluronic chains with side chains containing chondroitin sulfate and keratin sulfate. Repeated stress and aging of the nucleus pulposus lead to several changes.1,6–10 Histologically, there are loss of hydrophilic mucopolysaccharides, increase in keratin sulfate, and loss of water, which lead to disc shrinkage, loss of elasticity, and inequitable distribution of hydrostatic pressure on the anulus with compressive forces. As the disc weakens, surrounding structures are required to bear a greater burden of weight-bearing load and dynamic stresses. As surrounding structures bear greater weight, they undergo reactive changes. End plates, uncovertebral joints, and facet joints form osteophytes as a biomechanical mechanism to increase the weight-bearing surface area.10–14 The ligamentum flavum and PLL undergo hypertrophy.15–17 Dorsally, the ligamentum flavum can buckle into the spinal canal as the discs collapse. Ventrally, the anulus bulges into the spinal canal and dissects the PLL of the bone, and the PLL itself hypertrophies. Degenerative changes in the disc occur ventrally first, leading to kyphosis.
Cervical spondylotic changes can lead to spinal canal and intervertebral foramen narrowing that can impinge on the spinal cord centrally or on the exiting nerve roots laterally. Autopsy studies have described histologic changes that are seen in CSM, including white matter demyelination, particularly in lateral corticospinal tracts, gray matter neuronal loss, necrosis, and cavitation.18,19 Ogino et al. demonstrated that pathologic changes worsened with smaller anteroposterior canal diameter: reduction to 40% to 44% of normal led to mild white matter demyelination; reduction to 22% to 39% correlated with diffuse white matter demyelination and gray matter cavitation; and reduction to 12% to 19% led to white matter gliosis and diffuse gray matter necrosis.19
Pathologic changes found in CSM are due to factors that are often divided into static, dynamic, and vascular processes.1 Static processes are the reactive changes already described stemming from disc desiccation. Dynamic movement in cervical spondylosis may further lead to CSM. During flexion, the spinal cord elongates and may become trapped along ventral osteophytic spurs. With extension, ligamentum buckling may cause dorsal impingement.1,16,20 An MRI flexion-extension study by Muhle et al. demonstrated increasing spinal stenosis on average during extension compared to flexion.21 Finally, animal studies demonstrate that the changes that are observed in CSM mimic changes seen in ischemic cord models.18,22,23 Some authors hypothesize that this occurs because spinal cord compression leads to ischemia at the microcirculation level.22 Demyelination may also be due to increased susceptibility to ischemia seen in oligodendrocytes.20,24 While cervical spondylotic changes are seen throughout the subaxial spine, involvement at C5-6 is the most common, followed by C6-7.25 That this is likely due to the fact that motion is more common at C5-6 and C6-7, where most of flexion and extension in the subaxial spine occur, and motion leads to greater reactive changes.1,26 Spinal cord compression symptoms may be exacerbated by the fact that C5-7 is a watershed area in the cervical cord, with reduced blood flow and greater potential for spinal cord ischemia.27,28
Clinical Syndromes
Axial Pain
Neck pain is a common presenting chief complaint seen by the general practitioner. Contributing anatomic sources of neck pain are multiple and include neck musculature, tendons, ligaments, facet joints, intervertebral discs, craniovertebral junction, and cervical vasculature. Referred pain can be seen with shoulder and temporomandibular joint pathology as well. The intervertebral disc is innervated ventrally by branches from the sympathetic plexus and dorsally by the sinuvertebral nerve, which arises from the ventral nerve root.29–31 The sinuvertebral nerve also innervates the PLL, the dura, and a substantial portion of the vertebral body periosteum.1,28 Cervical facet joints are innervated by branches arising from the dorsal ramus.1
Axial pain can occur alone or in conjunction with radiculopathy and/or myelopathy. When pain occurs alone, the traditional dictum advocates nonoperative management. However, experience shows that when axial pain accompanies radiculopathy or myelopathy, surgery to ameliorate the latter frequently relieves the former.29 The most common cause of nondegenerative isolated neck pain is cervical strain resulting from injury to neck muscles, tendons, and ligaments that is frequently seen with whiplash injury.29 Beliefs about the anatomic source of isolated neck pain in patients with cervical spondylosis vary. The intervertebral disc is commonly cited as the source of axial pain.32 Tears in the anulus may stimulate the sinuvertebral nerve.33,34 Additionally, injection of local anesthetic in the disc space can temporarily relieve pain in some patients.35 The facet joints are another potential source of axial pain.36,37 Stimulation of subaxial facet joints generates reproducible neck pain patterns in normal volunteers.38 However, facet steroid injections39 and percutaneous radiofrequency neurotomy have demonstrated mediocre results.40,41
Isolated axial pain that fails to respond to initial conservative therapy can be further evaluated with cervical radiographs. Cervical spondylotic changes on radiograph are ubiquitous in the aging population and include loss of disc height, osteophyte formation, kyphosis, and subluxation.1,42 Flexion-extension cervical films greatly help in ruling out instability or motion that may be a source of significant pain.
In appropriately selected patients, several studies have demonstrated good results in operative management of axial pain.31,43–45 These studies utilized provocative discography to localize the level(s) of axial pain and treat symptomatic levels with anterior cervical decompression and fusion (ACDF). Neck pain is common in rheumatoid arthritis and can be secondary to instability or from basilar invagination, and surgery is commonly employed in this population. One must always be alert to the possibility of a C3-4 radiculopathy as a source of axial pain. Unilateral pain should alert the practitioner to look for sensory alterations, ask about paresthesias in this distribution, and look for a positive Spurling sign. C3-4 radiculopathy that causes axial pain generally responds very well to surgical decompression.46 Pseudarthrosis from previously attempted fusion can also lead to significant axial pain with or without radiculopathy and is a condition that also responds well to reoperation.
Isolated axial pain can be disabling to patients and presents a significant diagnostic and management challenge to the practitioner. The source of neck pain varies from person to person and in many patients is likely multifactorial. Acute neck pain deserves a trial of NSAIDs and short-term muscle relaxants if needed.47 A temporary soft neck collar can provide comfort as well. Chronic neck pain can be managed with analgesia and physical therapy exercises to strengthen the cervical musculature. Surgery should be reserved for patients with well-accepted indications. Although controversial, surgery may be considered in certain cases of disabling neck pain with positive properly performed discography.
Radiculopathy
Cervical radiculopathy results from compression of an exiting cervical nerve root. This often results from uncovertebral and facet osteophyte formation extending into the neural foramen. Patients often describe a sharp or burning radiating pain in a dermatomal distribution. Nerve compression can also result in paresthesias or impaired sensation in a dermatomal distribution or weakness in the respective myotome. Physical examination is often significant for a positive Spurling sign: Axial compression with lateral bending to the ipsilateral side reproduces the radicular pain. The abduction relief sign—relief of radicular pain by abducting the ipsilateral arm and putting the hand on the head—can help to differentiate radiculopathy from thoracic outlet syndrome or shoulder pathology.4,48 One must carefully evaluate the radiculopathic complaint and consider alternative etiologies such as peripheral entrapment syndromes, thoracic outlet syndrome, brachial neuritis, shoulder pathology, reflex sympathetic dystrophy, and even angina.1
When conservative therapy fails and the diagnosis of cervical root compression is certain, surgical decompression provides good results. When alignment is well maintained, a minimally destabilizing approach includes dorsal laminoforaminotomy. When fusion is needed, either ACDF or dorsal decompression with fusion provides good results in class III evidence. Persson et al. randomized 81 patients with cervical spondylotic radiculopathy to ACDF, physical therapy, or cervical collar immobilization. Evaluation at 3 to 4 months revealed improved pain scores (using a visual analogue scale) and motor and sensory improvements with surgery compared to nonoperative alternatives. This effect dissipated at 12-month follow-up; however, a disability rating index showed improved return to work and dressing ability at 12 months with surgery.49,50
Myelopathy
Patients with myelopathy commonly present with unsteady gait and difficulty with fine motor coordination in the hands.8,11 Physical examination may demonstrate hyperreflexia below the level of compression, increased muscle tone, clonus, the Babinski sign, the Hoffman sign, and the finger escape sign.8,51 Some patients may describe the Lhermitte sign (electric shock sensations traveling down the spine with flexion), which is thought to be due to stimulation of the dorsal columns. Hands may demonstrate intrinsic muscle atrophy, which is a classic sign in myelopathy.51,52 Some patients may complain of urinary retention or spastic detrusor activity leading to frequent urges with or without incontinence. Additional localizing upper motor signs include pectoral muscle reflex, which is suggestive of compression at or above C2-4, and the jaw jerk, which if present suggests a lesion above the foramen magnum.53,54 Patients with severe cervical spondylosis with canal stenosis can experience central cord syndrome with even minor trauma, particularly in hyperextension injury. Greater motor impairment is seen in the upper extremities and is often accompanied by urinary retention.55 Burning hands have been described in football injuries and are thought to be a variant of central cord syndrome in patients with congenital canal stenosis.56 The differential diagnosis for CSM is broad and includes multiple sclerosis, syringomyelia, atrophic lateral sclerosis, subacute combined degeneration, intraspinal tumor, spinal arteriovenous malformation, epidural abscess, Chiari malformation, ossification of the posterior longitudinal ligament, normal pressure hydrocephalus, tabes dorsalis, hereditary spastic paraplegia, and tropical spastic paraparesis.1,11,57,58 Several grading systems have been developed to classify the severity of CSM in an objective, reliable, and valid assessment that can also be used to measure responsiveness to therapeutic interventions. The Japanese Orthopaedic Association (JOA) scale and the modified version by Benzel et al. are the two most widely used systems and have demonstrated good interobserver and intraobserver reliability.59–61 Other accepted systems include gait analysis and the short form-36 (SF-36).62–65
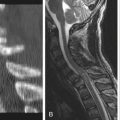
The gold standard for imaging in CSM has become MRI because it provides the best view of the spinal cord, exiting nerve roots, and CSF signal.66 CT myelography may be more useful in cases of previous surgery because it is superior to MRI in viewing residual bony anatomy and produces less artifact with existing hardware. The examiner must be aware that the degree of stenosis on imaging frequently does not correlate with clinical impairment. In one study of asymptomatic elderly patients, 26% had some degree of spinal cord impingement on MRI.11,67 Multiple studies have attempted to correlate spinal cord signal changes on MRI with neurologic recovery after decompression. Several class III studies demonstrate that T2 hyperintensity at a single segment does not predict outcome, but when present at multiple levels or in combination with T1 hypointensity, it does correlate with poor neurologic recovery after surgery.68–72 Other studies have attempted to correlate the degree of canal stenosis with neurologic recovery after surgery. Most studies demonstrate poorer neurologic recovery in patients with greater radiographic canal stenosis, with most studies using a canal area of 30 to 45 mm2 as the cutoff to dichotomize groups.73–76 One study did not corroborate these findings.77
Although electrodiagnostic studies are not necessary for diagnosis of CSM, a class I study by Bednarik et al. followed 66 patients (average age 50 years) with radiographic spinal cord compression from cervical spondylosis without clinical myelopathy. These patients were followed for an average of 4 years, during which 19.7% developed CSM. Bednarik et al. found that electromyography and sensory evoked potential abnormalities and, additionally, clinical radiculopathy, when present initially, predicted the development of CSM.78
Traditional teaching portrays the natural history of CSM as progressive stepwise neurologic deterioration. However, after initial presentation of neurologic impairment, the natural history is mixed. Some patients remain neurologically stable for long periods of time, with some even improving; others will continue to accrue additional deficits.79 Many class III studies have tracked the natural history of CSM.80–83 One of the initial studies by Clarke and Robinson in 1956 retrospectively reviewed 120 patients with CSM: 26 who never underwent surgery plus the preoperative course of 94 patients who eventually underwent surgery. They found that the majority (75%) of patients experienced episodes of neurologic deterioration with intervening periods of stability. Of the smaller cohort that did not undergo surgery, half experienced some degree of neurologic improvement with conservative management.81 Another study by Nurick in 1972 found that most patients remained neurologically stable after initial deficits, and he advocated surgery for those with progressive symptoms and those older than 60 years of age.80 One of the only class I studies, by Kadanka et al., demonstrated that 80% of patients younger than 75 years of age with 1 year of mild CSM (defined as modified JOA > 12) remained neurologically stable with conservative management (NSAIDs, rest, cervical immobilization) over 2 to 3 years as measured by the modified JOA scale, a timed 10-meter walk, and video evaluation of ADL performance.84,85 A 2002 Cochrane review of CSM concluded that there is no clear evidence to support the idea that CSM patients inevitably deteriorate neurologically.86 However, all of these studies of conservative management excluded patients who underwent early surgery likely because of more severe or progressive forms of CSM. Therefore, these studies have a selection bias toward patients with a more benign natural history and cannot be generalized.87
Furthering the decision maker’s dilemma, numerous studies demonstrate that increased symptom duration—most studies using between 12 and 24 months as cutoff—portends worse neurologic recovery.76,88–92 Therefore, it appears that in mild CSM, a conservative management trial is reasonable, but patients with unacceptable neurologic deficits and those with progressive symptoms should be considered for early decompression.
Multiple class III studies demonstrate that the majority of patients either improve or remain neurologically stable, by JOA or Nurick scores, after surgical decompression using both ventral and dorsal approaches.60,93–99
Surgical Strategies
Dorsal Approach
For isolated radiculopathy without myelopathy, dorsal laminoforaminotomy provides an effective alternative to decompress the exiting nerve root.100 The goal of foraminotomy is to provide additional space to the exiting root without necessarily resecting the offending osteophyte.
Laminectomy is frequently used for multilevel pathology, including multilevel cervical spondylosis, congenital canal stenosis, and dorsal compressive pathology such as ligamentum flavum hypertrophy or ossification. Laminectomy has also been successful for treatment of OPLL.101 Laminectomy alone is better suited for the straight or lordotic spine but not the kyphotic spine. Long-term studies show that the rate of postoperative kyphosis after isolated laminectomy ranges from 14% to 47%.102,103 The incidence of postoperative kyphosis increases with loss of lordosis on preoperative radiographs.103 Particularly concerning is that when multilevel ventral pathology exists, increasing kyphosis may result in further draping of the cord over ventral osteophytes. Laminectomy alone also results in a higher rate of kyphosis than laminoplasty.104,105 Numerous studies highlight an increased risk of late neurologic deterioration with laminectomy alone compared to ventral or dorsal decompression with fusion.60,106 However, these same studies are unable to directly correlate kyphosis with development of late neurologic deterioration. One study using dentate ligament sectioning found no additional benefit of such practice.60
Ventral Approach
When the offending compressive elements are ventral, a ventral approach allows better access for direct decompression. When there are three or fewer diseased levels, ACDF or ACCF may be used. For longer segments, either a dorsal or a combined approach is utilized. Ventral plate fixation and instrumentation have become commonplace but should not be a substitute for good graft technique. Kaiser et al. retrospectively compared 251 patients with ACDF with plate fixation showing a 96% fusion rate for single-level ACDF and a 90% fusion rate for two-level ACDF compared to historical fusion rates for single-level ACDF (91%) and two-level ACDF (72%). Additionally, graft complications with plate fixation were reduced from 6% to 1.3%.107 A large retrospective review by Caspar et al. found that the reoperation rate for pseudarthrosis was 4.8% for ACDF and 0.7% for ACDF with plate fixation.108 However, Resnick and Trost performed a systemic review of randomized trials that showed no clear benefit for ventral plate fixation in single-level ACDF.109 From a biomechanical perspective, plate fixation results in greater preservation of lordosis. Troyanovich et al. calculated that lordosis at the fused segment decreased by 2.5 degrees in ACDF but increased by 5.7 degrees in ACDF with plate fixation.110
ACCF is an alternative to ACDF. Traditionally, ACCF demonstrated higher rates of fusion than ACDF without plate fixation.95 However, ACCF appears to yield results equivalent to those of ACDF with plate fixation.111 A pooled analysis of 2682 patients by Fraser and Hartl found that two-level ACDF with plate fixation yielded fusion rates (>90%) similar to those of ACCF. For three-level disease, ACDF with plate fixation yielded significantly lower fusion rates (82.5%) than ACCF with plate fixation (96.2%).112
Ventral plates vary among manufacturers, and some have more recently produced dynamic plates that allow for motion. Class III studies show no difference in fusion rates between dynamic and rigid fixation plates. However, one study found a higher screw failure rate with rigid fixation but increased dysphagia with dynamic plates.113
Cervical disc arthroplasty presents an alternative to fusion with the theoretical benefit of motion sparing at the treated level and the hope of decreasing adjacent segment disease. Mummaneni et al. presented the first randomized controlled trial of 541 patients with single-level cervical disease randomized to arthroplasty versus ACDF without plate fixation. NDI, SF-36, and pain perception scores improved with both groups over a 2-year period. It appears that over the short term, cervical disc arthroplasty is at least as good as traditional fusion without fixation.114 Similar results have been found with alternative manufacturers.115,116 However, long-term neurologic outcome and safety are still to be determined.
Al-Mefty O., Harkey H.L., Marawi I., et al. Experimental chronic compressive cervical myelopathy. J Neurosurg. 1993;79(4):550-561.
Brain W.R., Northfield D., Wilkinson M. The neurological manifestations of cervical spondylosis. Brain. 1952;75(2):187-225.
Kadanka Z., Bednarik J., Vohanka S., et al. Conservative treatment versus surgery in spondylotic cervical myelopathy: a prospective randomised study. Eur Spine J. 2000;9(6):538-544.
Kaptain G.J., Simmons N.E., Replogle R.E., Pobereskin L. Incidence and outcome of kyphotic deformity following laminectomy for cervical spondylotic myelopathy. J Neurosurg. 2000;93(Suppl 2):199-204.
Persson L.C., Moritz U., Brandt L., Carlsson C.A. Cervical radiculopathy: pain, muscle weakness and sensory loss in patients with cervical radiculopathy treated with surgery, physiotherapy or cervical collar: a prospective, controlled study. Eur Spine J. 1997;6(4):256-266.
Shedid D., Benzel E.C. Cervical spondylosis anatomy: pathophysiology and biomechanics. Neurosurgery. 2007;60(1 Supp1 1):S7-S13.
White A.A.3rd, Panjabi M.M. Biomechanical considerations in the surgical management of cervical spondylotic myelopathy. Spine (Phila Pa 1976). 1988;13(7):856-860.
Yonenobu K., Abumi K., Nagata K., et al. Interobserver and intraobserver reliability of the Japanese Orthopaedic Association scoring system for evaluation of cervical compression myelopathy. Spine (Phila Pa 1976). 2001;26(17):1890-1894. discussion 1895
1. Shedid D., Benzel E.C. Cervical spondylosis anatomy: pathophysiology and biomechanics. Neurosurgery. 2007;60(1 Supp1 1):S7-S13.
2. Garfin S.R. Cervical degenerative disorders: etiology, presentation, and imaging studies. Instr Course Lect. 2000;49:335-338.
3. Brain W.R., Northfield D., Wilkinson M. The neurological manifestations of cervical spondylosis. Brain. 1952;75(2):187-225.
4. Harrop J.S., Hanna A., Silva M.T., Sharan A. Neurological manifestations of cervical spondylosis: an overview of signs, symptoms, and pathophysiology. Neurosurgery. 2007;60(1 Supp1 1):S14-S20.
5. Brain W.R.B., Wilkinson M. Cervical spondylosis and other disorders of the cervical spine. London: Heinemann, 1968.
6. McCormack B.M., Weinstein P.R. Cervical spondylosis: an update. West J Med. 1996;165(1–2):43-51.
7. Benzel E.C., American Association of Neurological Surgeons. Biomechanics of spine stabilization. Rolling Meadows, Ill: American Association of Neurological Surgeons; 2001.
8. Emery S.E. Cervical spondylotic myelopathy: diagnosis and treatment. J Am Acad Orthop Surg. 2001;9(6):376-388.
9. Ferguson R.J., Caplan L.R. Cervical spondylitic myelopathy. Neurol Clin. 1985;3(2):373-382.
10. Wilkinson M. The morbid anatomy of cervical spondylosis and myelopathy. Brain. 1960;83:589-617.
11. Baron E.M., Young W.F. Cervical spondylotic myelopathy: a brief review of its pathophysiology, clinical course, and diagnosis. Neurosurgery. 2007;60(1 Supp1 1):S35-S41.
12. Hoff J.T., Wilson C.B. The pathophysiology of cervical spondylotic radiculopathy and myelopathy. Clin Neurosurg. 1977;24:474-487.
13. Kumaresan S., Yoganandan N., Pintar F.A., et al. Contribution of disc degeneration to osteophyte formation in the cervical spine: a biomechanical investigation. J Orthop Res. 2001;19(5):977-984.
14. Parke W.W. Correlative anatomy of cervical spondylotic myelopathy. Spine (Phila Pa 1976). 1988;13(7):831-837.
15. White A.A.3rd, Panjabi M.M. Biomechanical considerations in the surgical management of cervical spondylotic myelopathy. Spine (Phila Pa 1976). 1988;13(7):856-860.
16. Panjabi M., White A.3rd. Biomechanics of nonacute cervical spinal cord trauma. Spine (Phila Pa 1976). 1988;13(7):838-842.
17. Epstein J.A., Epstein B.S., Lavine L.S., et al. Cervical myeloradiculopathy caused by arthrotic hypertrophy of the posterior facets and laminae. J Neurosurg. 1978;49(3):387-392.
18. Ito T., Oyanagi K., Takahashi H., et al. Cervical spondylotic myelopathy: clinicopathologic study on the progression pattern and thin myelinated fibers of the lesions of seven patients examined during complete autopsy. Spine (Phila Pa 1976). 1996;21(7):827-833.
19. Ogino H., Tada K., Okada K., et al. Canal diameter, anteroposterior compression ratio, and spondylotic myelopathy of the cervical spine. Spine (Phila Pa 1976). 1983;8(1):1-15.
20. Fehlings M.G., Skaf G. A review of the pathophysiology of cervical spondylotic myelopathy with insights for potential novel mechanisms drawn from traumatic spinal cord injury. Spine (Phila Pa 1976). 1998;23(24):2730-2737.
21. Muhle C., Weinert D., Falliner A., et al. Dynamic changes of the spinal canal in patients with cervical spondylosis at flexion and extension using magnetic resonance imaging. Invest Radiol. 1998;33(8):444-449.
22. Al-Mefty O., Harkey H.L., Marawi I., et al. Experimental chronic compressive cervical myelopathy. J Neurosurg. 1993;79(4):550-561.
23. Gooding M.R., Wilson C.B., Hoff J.T. Experimental cervical myelopathy: effects of ischemia and compression of the canine cervical spinal cord. J Neurosurg. 1975;43(1):9-17.
24. Gledhill R.F., Harrison B.M., McDonald W.I. Demyelination and remyelination after acute spinal cord compression. Exp Neurol. 1973;38(3):472-487.
25. Crandall P.H., Batzdorf U. Cervical spondylotic myelopathy. J Neurosurg. 1966;25(1):57-66.
26. Arnasson O., Carlsson C.A., Pellettieri L. Surgical and conservative treatment of cervical spondylotic radiculopathy and myelopathy. Acta Neurochir (Wien). 1987;84(1–2):48-53.
27. Bohlman H.H., Emery S.E. The pathophysiology of cervical spondylosis and myelopathy. Spine (Phila Pa 1976). 1988;13(7):843-846.
28. Connell M.D., Wiesel S.W. Natural history and pathogenesis of cervical disk disease. Orthop Clin North Am. 1992;23(3):369-380.
29. Ahn N.U., Ahn U.M., Ipsen B., An H.S. Mechanical neck pain and cervicogenic headache. Neurosurgery. 2007;60(1 Supp1 1):S21-S27.
30. Bogduk N., Windsor M., Inglis A. The innervation of the cervical intervertebral discs. Spine (Phila Pa 1976). 1988;13(1):2-8.
31. Wieser E.S., Wang J.C. Surgery for neck pain. Neurosurgery. 2007;60(1 Supp1 1):S51-S56.
32. Grob D. Surgery in the degenerative cervical spine. Spine (Phila Pa 1976). 1998;23(24):2674-2683.
33. Ahn N.U., Ahn U.M., Andersson G.B., An H.S. Operative treatment of the patient with neck pain. Phys Med Rehabil Clin N Am. 2003;14(3):675-692.
34. Buckwalter J.A. Aging and degeneration of the human intervertebral disc. Spine (Phila Pa 1976). 1995;20(11):1307-1314.
35. Roth D.A. Cervical analgesic discography: a new test for the definitive diagnosis of the painful-disk syndrome. JAMA. 1976;235(16):1713-1714.
36. Aprill C., Dwyer A., Bogduk N. Cervical zygapophyseal joint pain patterns. II: A clinical evaluation. Spine (Phila Pa 1976). 1990;15(6):458-461.
37. Bogduk N., Marsland A. The cervical zygapophysial joints as a source of neck pain. Spine (Phila Pa 1976). 1988;13(6):610-617.
38. Dwyer A., Aprill C., Bogduk N. Cervical zygapophyseal joint pain patterns. I: A study in normal volunteers. Spine (Phila Pa 1976). 1990;15(6):453-457.
39. Barnsley L., Lord S.M., Wallis B.J., Bogduk N. Lack of effect of intraarticular corticosteroids for chronic pain in the cervical zygapophyseal joints. N Engl J Med. 1994;330(15):1047-1050.
40. Lord S.M., Barnsley L., Bogduk N. The utility of comparative local anesthetic blocks versus placebo-controlled blocks for the diagnosis of cervical zygapophysial joint pain. Clin J Pain. 1995;11(3):208-213.
41. Lord S.M., Barnsley L., Wallis B.J., et al. Percutaneous radio-frequency neurotomy for chronic cervical zygapophyseal-joint pain. N Engl J Med. 1996;335(23):1721-1726.
42. Alker G. Neuroradiology of cervical spondylotic myelopathy. Spine (Phila Pa 1976). 1988;13(7):850-853.
43. Garvey T.A., Transfeldt E.E., Malcolm J.R., Kos P. Outcome of anterior cervical discectomy and fusion as perceived by patients treated for dominant axial-mechanical cervical spine pain. Spine (Phila Pa 1976). 2002;27(17):1887-1895. discussion 1895
44. Palit M., Schofferman J., Goldthwaite N., et al. Anterior discectomy and fusion for the management of neck pain. Spine (Phila Pa 1976). 1999;24(21):2224-2228.
45. Whitecloud T.S.3rd, Seago R.A. Cervical discogenic syndrome: results of operative intervention in patients with positive discography. Spine (Phila Pa 1976). 1987;12(4):313-316.
46. Jenis L.G., An H.S. Neck pain secondary to radiculopathy of the fourth cervical root: an analysis of 12 surgically treated patients. J Spinal Disord. 2000;13(4):345-349.
47. Mazanec D., Reddy A. Medical management of cervical spondylosis. Neurosurgery. 2007;60(1 Supp1 1):S43-S50.
48. Davidson R.I., Dunn E.J., Metzmaker J.N. The shoulder abduction test in the diagnosis of radicular pain in cervical extradural compressive monoradiculopathies. Spine (Phila Pa 1976). 1981;6(5):441-446.
49. Persson L.C., Moritz U., Brandt L., Carlsson C.A. Cervical radiculopathy: pain, muscle weakness and sensory loss in patients with cervical radiculopathy treated with surgery, physiotherapy or cervical collar: a prospective, controlled study. Eur Spine J. 1997;6(4):256-266.
50. Persson L.C., Lilja A. Pain, coping, emotional state and physical function in patients with chronic radicular neck pain: a comparison between patients treated with surgery, physiotherapy or neck collar—a blinded, prospective randomized study. Disabil Rehabil. 2001;23(8):325-335.
51. Ono K., Ebara S., Fuji T., et al. Myelopathy hand: new clinical signs of cervical cord damage. J Bone Joint Surg [Br]. 1987;69(2):215-219.
52. Ebara S., Yonenobu K., Fujiwara K., et al. Myelopathy hand characterized by muscle wasting: a different type of myelopathy hand in patients with cervical spondylosis. Spine (Phila Pa 1976). 1988;13(7):785-791.
53. Heller J.G. The syndromes of degenerative cervical disease. Orthop Clin North Am. 1992;23(3):381-394.
54. Watson J.C., Broaddus W.C., Smith M.M., Kubal W.S. Hyperactive pectoralis reflex as an indicator of upper cervical spinal cord compression: report of 15 cases. J Neurosurg. 1997;86(1):159-161.
55. Schneider R.C. The syndrome of acute anterior spinal cord injury. J Neurosurg. 1955;12(2):95-122.
56. Maroon J.C. “Burning hands” in football spinal cord injuries. JAMA. 1977;238(19):2049-2051.
57. Osborn A.G. Diagnostic neuroradiology. St. Louis: Mosby; 1994.
58. Moore A.P., Blumhardt L.D. A prospective survey of the causes of non-traumatic spastic paraparesis and tetraparesis in 585 patients. Spinal Cord. 1997;35(6):361-367.
59. Fujiwara A., Kobayashi N., Saiki K., et al. Association of the Japanese Orthopaedic Association score with the Oswestry Disability Index, Roland-Morris Disability Questionnaire, and Short-Form 36. Spine (Phila Pa 1976). 2003;28(14):1601-1607.
60. Benzel E.C., Lancon J., Kesterson L., Hadden T. Cervical laminectomy and dentate ligament section for cervical spondylotic myelopathy. J Spinal Disord. 1991;4(3):286-295.
61. Yonenobu K., Abumi K., Nagata K., et al. Interobserver and intraobserver reliability of the Japanese Orthopaedic Association scoring system for evaluation of cervical compression myelopathy. Spine (Phila Pa 1976). 2001;26(17):1890-1894. discussion 1895
62. Moorthy R.K., Bhattacharji S., Thayumanasamy G., Rajshekhar V. Quantitative changes in gait parameters after central corpectomy for cervical spondylotic myelopathy. J Neurosurg Spine. 2005;2(4):418-424.
63. Kuhtz-Buschbeck J.P., Jöhnk K., Mäder S., et al. Analysis of gait in cervical myelopathy. Gait Posture. 1999;9(3):184-189.
64. King J.T.Jr., Roberts M.S. Validity and reliability of the Short Form-36 in cervical spondylotic myelopathy. J Neurosurg. 2002;97(Suppl 2):180-185.
65. Singh A., Gnanalingham K., Casey A., Crockard A. Quality of life assessment using the Short Form-12 (SF-12) questionnaire in patients with cervical spondylotic myelopathy: comparison with SF-36. Spine (Phila Pa 1976). 2006;31(6):639-643.
66. Al-Mefty O., Harkey L.H., Middleton T.H., et al. Myelopathic cervical spondylotic lesions demonstrated by magnetic resonance imaging. J Neurosurg. 1988;68(2):217-222.
67. Teresi L.M., Lufkin R.B., Reicher M.A., et al. Asymptomatic degenerative disk disease and spondylosis of the cervical spine: MR imaging. Radiology. 1987;164(1):83-88.
68. Morio Y., Teshima R., Nagashima H., et al. Correlation between operative outcomes of cervical compression myelopathy and MRI of the spinal cord. Spine (Phila Pa 1976). 2001;26(11):1238-1245.
69. Morio Y., Yamamoto K., Kuranobu K., et al. Does increased signal intensity of the spinal cord on MR images due to cervical myelopathy predict prognosis? Arch Orthop Trauma Surg. 1994;113(5):254-259.
70. Suri A., Chabbra R.P., Mehta V.S., et al. Effect of intramedullary signal changes on the surgical outcome of patients with cervical spondylotic myelopathy. Spine J. 2003;3(1):33-45.
71. Fernandez de Rota J.J., Meschian S., Fernandez de Rota A., et al. Cervical spondylotic myelopathy due to chronic compression: the role of signal intensity changes in magnetic resonance images. J Neurosurg Spine. 2007;6(1):17-22.
72. Papadopoulos C.A., Katonis P., Papagelopoulos P.J., et al. Surgical decompression for cervical spondylotic myelopathy: correlation between operative outcomes and MRI of the spinal cord. Orthopedics. 2004;27(10):1087-1091.
73. Kasai Y., Uchida A. New evaluation method using preoperative magnetic resonance imaging for cervical spondylotic myelopathy. Arch Orthop Trauma Surg. 2001;121(9):508-510.
74. Fukushima T., Ikata T., Taoka Y., Takata S. Magnetic resonance imaging study on spinal cord plasticity in patients with cervical compression myelopathy. Spine (Phila Pa 1976). 1991;16(Suppl 10):S534-S538.
75. Matsuyama Y., Kawakami N., Mimatsu K. Spinal cord expansion after decompression in cervical myelopathy: investigation by computed tomography myelography and ultrasonography. Spine (Phila Pa 1976). 1995;20(15):1657-1663.
76. Yamazaki T., Yanaka K., Sato H., et al. Cervical spondylotic myelopathy: surgical results and factors affecting outcome with special reference to age differences. Neurosurgery. 2003;52(1):122-126. discussion 126
77. Mummaneni P.V., Kaiser M.G., Matz P.G., et al. Preoperative patient selection with magnetic resonance imaging, computed tomography, and electroencephalography: does the test predict outcome after cervical surgery? J Neurosurg Spine. 2009;11(2):119-129.
78. Bednarik J., Kadanka Z., Dusek L., et al. Presymptomatic spondylotic cervical cord compression. Spine (Phila Pa 1976). 2004;29(20):2260-2269.
79. Matz P.G., Anderson P.A., Holly L.T., et al. The natural history of cervical spondylotic myelopathy. J Neurosurg Spine. 2009;11(2):104-111.
80. Nurick S. The natural history and the results of surgical treatment of the spinal cord disorder associated with cervical spondylosis. Brain. 1972;95(1):101-108.
81. Clarke E., Robinson P.K. Cervical myelopathy: a complication of cervical spondylosis. Brain. 1956;79(3):483-510.
82. Lees F., Turner J.W. Natural history and prognosis of cervical spondylosis. Br Med J. 1963;2(5373):1607-1610.
83. Barnes M.P., Saunders M. The effect of cervical mobility on the natural history of cervical spondylotic myelopathy. J Neurol Neurosurg Psychiatry. 1984;47(1):17-20.
84. Kadanka Z., Bednarik J., Vohanka S., et al. Conservative treatment versus surgery in spondylotic cervical myelopathy: a prospective randomised study. Eur Spine J. 2000;9(6):538-544.
85. Kadanka Z., Mares M., Bednanik J., et al. Approaches to spondylotic cervical myelopathy: conservative versus surgical results in a 3-year follow-up study. Spine (Phila Pa 1976). 2002;27(20):2205-2210. discussion 2210–2211
86. Fouyas I.P., Statham P.F., Sandercock P.A. Cochrane review on the role of surgery in cervical spondylotic radiculomyelopathy. Spine (Phila Pa 1976). 2002;27(7):736-747.
87. Holly L.T., Matz P.G., Anderson P.A., et al. Clinical prognostic indicators of surgical outcome in cervical spondylotic myelopathy. J Neurosurg Spine. 2009;11(2):112-118.
88. Fujiwara K., Yonenobu K., Ebara S., et al. The prognosis of surgery for cervical compression myelopathy: an analysis of the factors involved. J Bone Joint Surg [Br]. 1989;71(3):393-398.
89. Ebersold M.J., Pare M.C., Quast L.M. Surgical treatment for cervical spondylitic myelopathy. J Neurosurg. 1995;82(5):745-751.
90. Sadasivan K.K., Reddy R.P., Albright J.A. The natural history of cervical spondylotic myelopathy. Yale J Biol Med. 1993;66(3):235-242.
91. Handa Y., Kubota T., Ishii H., et al. Evaluation of prognostic factors and clinical outcome in elderly patients in whom expansive laminoplasty is performed for cervical myelopathy due to multisegmental spondylotic canal stenosis: a retrospective comparison with younger patients. J Neurosurg. 2002;96(Suppl 2):173-179.
92. Pollard M.E., Apple D.F. Factors associated with improved neurologic outcomes in patients with incomplete tetraplegia. Spine (Phila Pa 1976). 2003;28(1):33-39.
93. Chiles B.W.3rd, Leonard M.A., Choudhri H.F., Cooper P.R. Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery. 1999;44(4):762-769. discussion 769–770
94. Heller J.G., Edwards C.C.2nd, Murakami H., Rodts G.E. Laminoplasty versus laminectomy and fusion for multilevel cervical myelopathy: an independent matched cohort analysis. Spine (Phila Pa 1976). 2001;26(12):1330-1336.
95. Emery S.E., Bohlman H.H., Bolesta M.J., Jones P.K. Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy: two to seventeen-year follow-up. J Bone Joint Surg [Am]. 1998;80(7):941-951.
96. Sakaura H., Hosono N., Mukai Y., et al. Long-term outcome of laminoplasty for cervical myelopathy due to disc herniation: a comparative study of laminoplasty and anterior spinal fusion. Spine (Phila Pa 1976). 2005;30(7):756-759.
97. Wada E., Suzuki S., Kanazawa A., et al. Subtotal corpectomy versus laminoplasty for multilevel cervical spondylotic myelopathy: a long-term follow-up study over 10 years. Spine (Phila Pa 1976). 2001;26(13):1443-1447. discussion 1448
98. Yonenobu K., Fuji T., Ono K., et al. Choice of surgical treatment for multisegmental cervical spondylotic myelopathy. Spine (Phila Pa 1976). 1985;10(8):710-716.
99. Yoshida M., Tamaki T., Kawakami M., et al. Indication and clinical results of laminoplasty for cervical myelopathy caused by disc herniation with developmental canal stenosis. Spine (Phila Pa 1976). 1998;23(22):2391-2397.
100. Heary R.F., Ryken T.C., Matz P.G., et al. Cervical laminoforaminotomy for the treatment of cervical degenerative radiculopathy. J Neurosurg Spine. 2009;11(2):198-202.
101. Kato Y., Iwasaki M., Fuji T., et al. Long-term follow-up results of laminectomy for cervical myelopathy caused by ossification of the posterior longitudinal ligament. J Neurosurg. 1998;89(2):217-223.
102. Guigui P., Benoist M., Deburge A. Spinal deformity and instability after multilevel cervical laminectomy for spondylotic myelopathy. Spine (Phila Pa 1976). 1998;23(4):440-447.
103. Kaptain G.J., Simmons N.E., Replogle R.E., Pobereskin L. Incidence and outcome of kyphotic deformity following laminectomy for cervical spondylotic myelopathy. J Neurosurg. 2000;93(Suppl 2):199-204.
104. Ishida Y., Suzuki K., Ohmori K., et al. Critical analysis of extensive cervical laminectomy. Neurosurgery. 1989;24(2):215-222.
105. Matsunaga S., Sakou T., Nakanisi K. Analysis of the cervical spine alignment following laminoplasty and laminectomy. Spinal Cord. 1999;37(1):20-24.
106. Ryken T.C., Heary R.F., Matz P.G., et al. Cervical laminectomy for the treatment of cervical degenerative myelopathy. J Neurosurg Spine. 2009;11(2):142-149.
107. Kaiser M.G., Haid R.W.Jr., Subach B.R., et al. Anterior cervical plating enhances arthrodesis after discectomy and fusion with cortical allograft. Neurosurgery. 2002;50(2):229-236. discussion 236–238
108. Caspar W., Geisler F.H., Pitzen T., Johnson T.A. Anterior cervical plate stabilization in one- and two-level degenerative disease: overtreatment or benefit? J Spinal Disord. 1998;11(1):1-11.
109. Resnick D.K., Trost G.R. Use of ventral plates for cervical arthrodesis. Neurosurgery. 2007;60(1 Supp1 1):S112-S117.
110. Troyanovich S.J., Stroink A.R., Kattner K.A., et al. Does anterior plating maintain cervical lordosis versus conventional fusion techniques? A retrospective analysis of patients receiving single-level fusions. J Spinal Disord Tech. 2002;15(1):69-74.
111. Wang J.C., McDonough P.W., Endow K.K., Delamarter R.B. A comparison of fusion rates between single-level cervical corpectomy and two-level discectomy and fusion. J Spinal Disord. 2001;14(3):222-225.
112. Fraser J.F., Hartl R. Anterior approaches to fusion of the cervical spine: a metaanalysis of fusion rates. J Neurosurg Spine. 2007;6(4):298-303.
113. Saphier P.S., Arginteanu M.S., Moore F.M., et al. Stress-shielding compared with load-sharing anterior cervical plate fixation: a clinical and radiographic prospective analysis of 50 patients. J Neurosurg Spine. 2007;6(5):391-397.
114. Mummaneni P.V., Burkus J.K., Haid R.W., et al. Clinical and radiographic analysis of cervical disc arthroplasty compared with allograft fusion: a randomized controlled clinical trial. J Neurosurg Spine. 2007;6(3):198-209.
115. Heller J.G., Sasso R.C., Papadopoulos S.M., et al. Comparison of BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion: clinical and radiographic results of a randomized, controlled, clinical trial. Spine (Phila Pa 1976). 2009;34(2):101-107.
116. Murrey D., Janssen M., Delamarter R., et al. Results of the prospective, randomized, controlled multicenter Food and Drug Administration investigational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease. Spine J. 2009;9(4):275-286.