CHAPTER 24 Carotid Endarterectomy and Carotid Stenting
INDICATIONS FOR SURGERY
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Preoperative Considerations
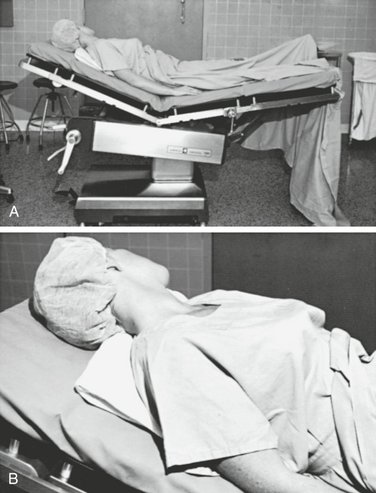
Patient Positioning and Preparation
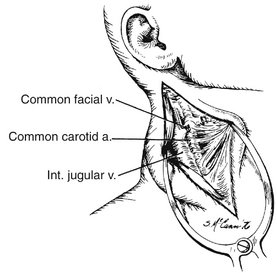
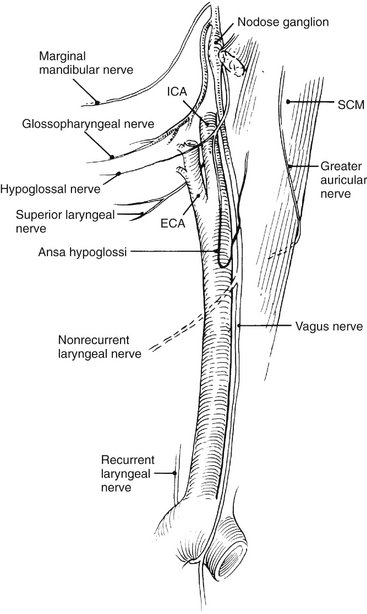
Incision and Exposure
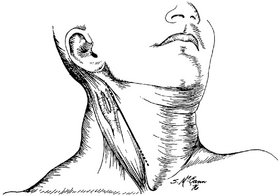
Figure 24-2 Incision for carotid endarterectomy and its relationship to the carotid bifurcation.
(From Rutherford RB: Vascular Surgery, 6th ed. Philadelphia, Saunders, 2005.)
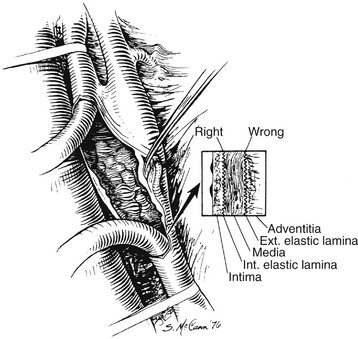
Endarterectomy
Arterial Reconstruction and Wound Closure
COMPLICATIONS
CAROTID ANGIOPLASTY AND STENTING
. Endarterectomy for asymptomatic carotid artery stenosis [Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA. 1995;173:1421-1428.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: Surgical results in 1415 patients. Stroke. 1999;30:1751-1758.
Krupski WC, Moore WS. Indications, surgical technique and results for repair of extracranial occlusive lesions. In Rutherford RB, editor: Vascular Surgery, 6th ed, Philadelphia: Saunders, 2005.
Moore WS. Extracranial cerebrovascular: the carotid artery. In Moore WS, editor: Vascular and Endovascular Surgery: A Comprehensive Review, 7th ed, Philadelphia: Saunders, 2006.