[level-membership-for-basic-science-category]
Chapter 8 Bones of the Skull and Orbit
Bones of the Cranium
The paired parietal bones form the roof and sides of the cranium (Figure 8-1). The parietal bones articulate with each other at the midline in the sagittal suture, with the occipital bone posteriorly in the lambdoid suture, and with the frontal bone anteriorly at the coronal suture. The parietal bone articulates inferiorly with the temporal bone and the greater wing of the sphenoid bone.
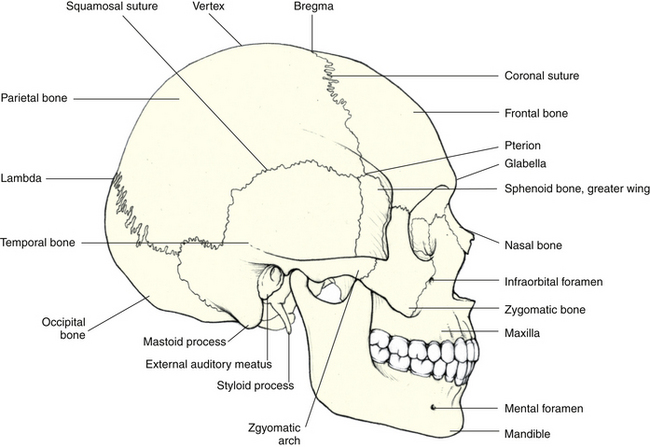
FIGURE 8-1 Lateral view of skull.
(From Mathers LH, Chase RA, Dolph J et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
The occipital bone forms the posterior aspect of the skull and posterior floor of the cranial cavity. A prominence, the external occipital protuberance, or inion, is found on the external surface at the posterior midline (Figure 8-2). The large foramen magnum is found in the inferior aspect of the occipital bone. The inner surface of the bone forms the posterior cranial fossa, in which there are depressions where the lobes of the cerebellum lie. Figure 8-3 shows the inner aspect of the cranial floor. The occipital bone articulates with the temporal bones, parietal bones, and sphenoid bone.
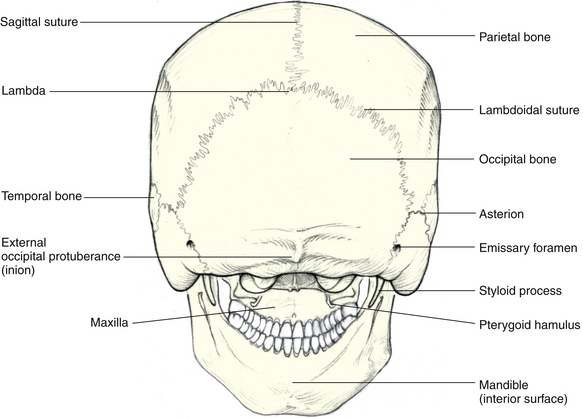
FIGURE 8-2 Posterior view of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
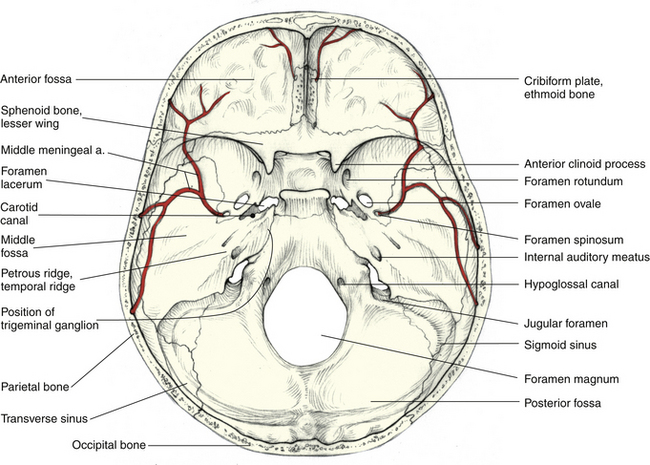
FIGURE 8-3 Floor of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
Bones of the Face
The single frontal bone forms the forehead and articulates with the nasal bones, maxillae, and zygomatic bones in formation of the face (see Figure 8-4). The sutures joining adjacent bones of the face generally are named according to the names of the two bones that are connected (e.g., the suture between the frontal bone and the zygomatic bone is the frontozygomatic suture).
The two maxillae, or maxillary bones, form the upper jaw, the hard palate, the lateral walls of the nasal cavity, and the floor of both orbits (see Figure 8-4). Each maxillary bone articulates with the frontal, nasal, lacrimal, ethmoid, sphenoid, palatine, and zygomatic bones. That portion of the maxillary bone forming the cheek contains the maxillary sinus.
Each of the temporal bones is composed of two portions: a large, flat plate, the squamous portion; and a thickened, wedge-shaped area, the petrous portion. The squamous portion forms the side of the cranium and articulates with the parietal bone and the sphenoid bone. An anterior projection, the zygomatic process, articulates with the zygomatic bone (see Figure 8-1). The petrous portion extends within the cranium and houses the middle and inner ear structures. The mastoid process and styloid process project from the inferior aspect, and between these two processes is the stylomastoid foramen, through which the facial nerve exits the skull. The petrous portion articulates with the occipital bone in the floor of the skull. The carotid canal runs superiorly and anteriorly through the petrous portion and provides an entrance for the internal carotid artery into the cranial cavity (Figure 8-3).
The single frontal bone forms the anterior portion of the cranium, anterior floor of the cranial cavity, and superior part of the face (Figure 8-4). At the top of the skull, the frontal bone articulates with the parietal bones; inferiorly it articulates with the sphenoid bone, ethmoid bone, and lacrimal bones. Inferoanteriorly, it articulates with the nasal bones, maxillary bones, and zygomatic bones. The inner surface of the cranial cavity portion of the frontal bone forms the anterior cranial fossa (see Figure 8-3), in which the frontal lobes of the cerebral hemispheres lie. The frontal sinuses are located within the anterior portion of the frontal bone.
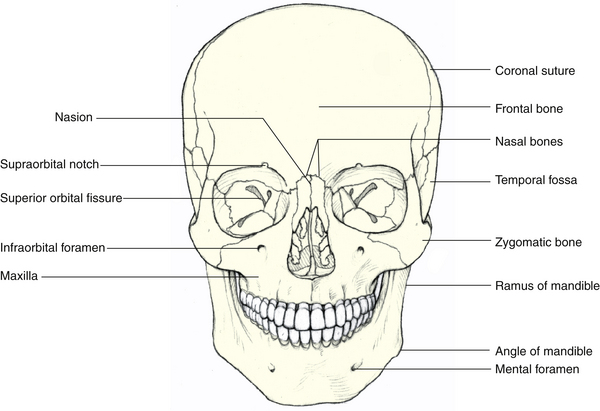
FIGURE 8-4 Anterior view of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
The sphenoid bone is a single bone, the body of which lies in the midline and articulates with the occipital bone and the temporal bones to form the base of the cranium (see Figure 8-3). The sphenoid bone joins the zygomatic bones to form the lateral walls of the orbits. Anteriorly and inferiorly the sphenoid bone articulates with the maxillary and palatine bones, superiorly with the parietal bones, and anteriorly and superiorly with the ethmoid and frontal bones. The depression on the superior cranial surface of the body of the sphenoid bone, the hypophyseal fossa (or the sella turcica), houses the pituitary gland; a portion of the body is hollow, forming the sphenoid sinus cavity.
Two pairs of wings project from the body of the sphenoid bone. The lesser wings project from the anterior aspect of the body and are more superior and smaller than the greater wings (see Figure 8-3). The lesser wings are attached to the body by small roots or struts. The gap between the lesser wing and the sphenoid body forms the optic foramen (canal) through which the optic nerve exits the orbit. The lesser wings articulate with the frontal and ethmoid bones.
The greater wings project from the lateral aspects of the body and articulate with the frontal bone, the parietal bones, squamous portions of the temporal bones, and the zygomatic bones. The pterygoid process projects from the base of the greater wing and articulates with the vertical stem of the palatine bone; each contributes to a shallow depression, the pterygopalatine fossa. Three important foramina are located in the greater wing (Figure 8-5): the foramen rotundum, through which the maxillary nerve passes; the foramen ovale, through which the mandibular nerve passes; and the foramen spinosum, through which the middle meningeal artery passes.
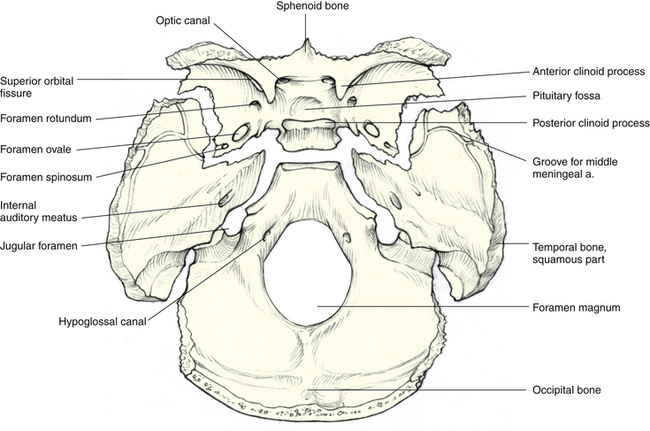
FIGURE 8-5 Disarticulated view of base of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
The two nasal bones form the bridge of the nose and articulate with each other, with the frontal bone, and with the frontal processes of the maxillary bones (see Figure 8-4). The vomer is a single bone that forms the posterior part of the nasal septum. It articulates with the palatine and maxillary bones inferiorly and with the ethmoid bone superiorly. The inferior conchae are separate bones located along the lateral walls of the nasal cavity.
The paired zygomatic bones form the lateral part of the cheekbones and articulate with the zygomatic process of the temporal bones to form the zygomatic arches (see Figure 8-1). The zygomatic bones also articulate with the maxillary bones and with the greater wings of the sphenoid bone.
The Orbit
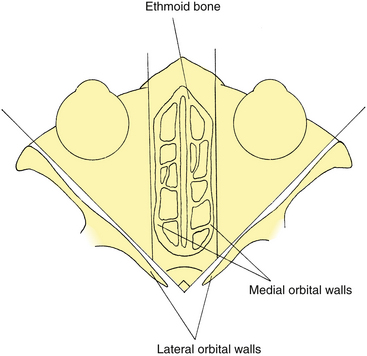
The orbit is shaped like a four-sided pyramid, the base of which is at the anterior orbital margin and the apex at the posterior margin within the skull. The orbital walls are referred to as the roof, floor, and medial and lateral walls. The medial walls run approximately parallel to each other, whereas the two lateral walls, if extended posteriorly, would form approximately a 90-degree angle with each other1,2 (Figure 8-6). The orbit has also been described as pear shaped, having its widest portion 1.5 cm inside the orbital margin.1 The orbital floor extends to approximately two-thirds the depth of the orbit; the other three sides extend to the apex.
Each orbit is composed of seven bones—the frontal, maxillary, zygomatic, sphenoid, ethmoid, palatine, and lacrimal bones (Figure 8-7). The frontal, sphenoid, and ethmoid are each a single bone and take part in the formation of both orbits.
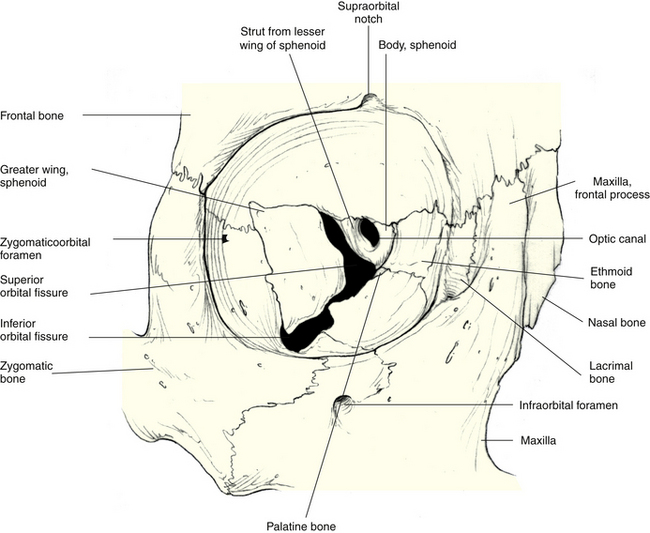
FIGURE 8-7 Anterior view of bones of orbit.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
Orbital Walls
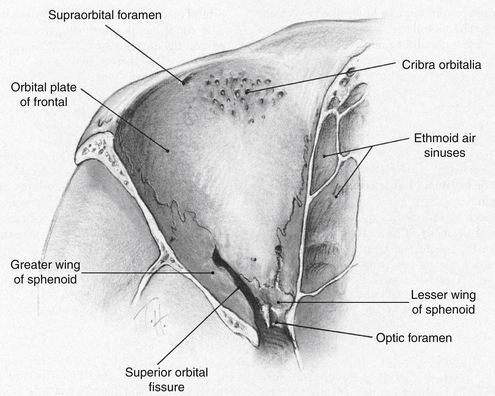
Roof
The roof is triangular and is composed primarily of the orbital plate of the frontal bone in front (Figure 8-8). The lesser wing of the sphenoid contributes a small posterior portion. The orbital plate of the frontal bone is thin in the area that separates the orbit from the anterior cranial fossa. In an elderly adult, bone in this area may resorb, leaving only the periosteal connective tissue in contact with the dural covering of the frontal lobe of the brain. The small area of the lesser wing of the sphenoid that is involved in this wall runs slightly downward, and an oval foramen, the optic canal, lies between it and the body of the sphenoid (see Figure 8-7). This optic foramen is located roughly at the apex of the orbit.
Floor
The floor is also triangular and is composed of the orbital plate of the maxillary bone and the orbital plate of the zygomatic bone in front and the small orbital process of the palatine bone behind (Figure 8-9). The maxillary bone makes up the largest part of the floor, and most of the remainder is provided by the zygomatic bone. The orbital process of the palatine bone is a small, flattened area at the top of the vertical arm and is located at the most posterior edge of the orbital plate of the maxilla. Often in the adult skull, the suture between the orbital process of the palatine bone and the maxilla is indistinguishable.
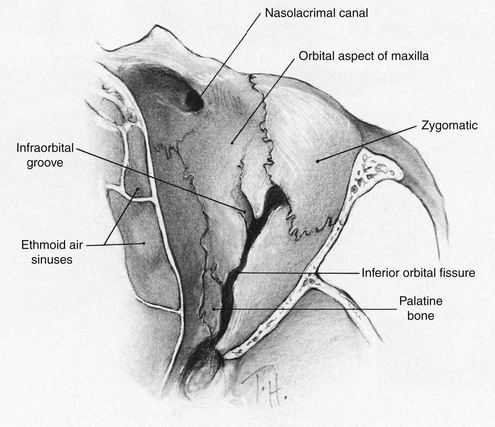
FIGURE 8-9 Bones of orbital floor.
(From Doxanas MT, Anderson RL: Clinical orbital anatomy, Baltimore, 1984, Williams & Wilkins.)
The floor does not reach all the way to the apex and is separated from the lateral wall posteriorly by the inferior orbital fissure. The infraorbital groove runs across the floor from the inferior orbital fissure and anteriorly is bridged by a thin plate of bone, thus becoming a canal running within the maxillary bone. This canal opens on the facial surface of the maxilla below the inferior orbital margin as the infraorbital foramen (see Figure 8-7). The inferior orbital margin is composed of the maxilla and the maxillary process of the zygomatic bone.
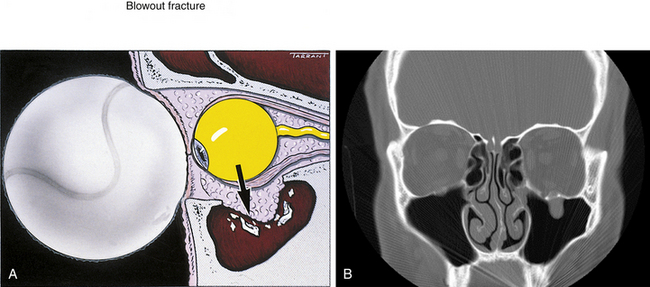
Clinical Comment: Blow-Out Fracture of the Orbit
The orbital rim is strong and can withstand considerable impact. However, a blow to the orbital rim can cause compression of the orbital contents, and such a sudden increase in intraorbital pressure might cause a fracture in one of the orbital walls. In the classic blow-out fracture, the orbital rim remains intact. The floor of the orbit is particularly susceptible to such a fracture, which usually occurs in the thin region along the infraorbital canal2–4 (Figure 8-10). Clinical signs and symptoms accompanying this damage include orbital swelling, ecchymosis, anesthesia of the area innervated by the infraorbital nerve, and diplopia caused by restriction of ocular motility (particularly noted in upward gaze).4 Limitations in ocular motility are caused by damage to the inferior extraocular muscles, either from bruising or hematoma or from entrapment of the muscle or adjoining connective tissue within the fracture.3,5,6
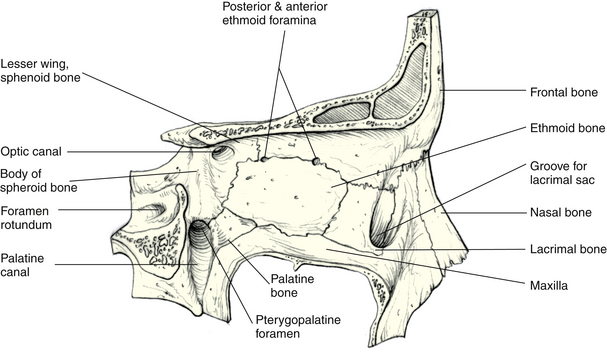
Medial Wall
The medial wall is rectangular. From front to back, it is formed by the frontal process of the maxilla, the lacrimal bone, the orbital plate of the ethmoid, and a part of the body of the sphenoid (Figure 8-11). A ridge on the frontal process of the maxilla that forms the anterior part of the medial orbital margin also forms the anterior lacrimal crest, which demarcates one border of the fossa for the lacrimal sac. The lacrimal bone, a small bone approximately the size of a thumbnail, together with the frontal process of the maxillary bone, forms the wall of this fossa. The lower portion of the fossa is a groove that is continuous inferiorly with the nasolacrimal canal, which continues into the nasal cavity. A ridge in the lacrimal bone forms the posterior lacrimal crest and is continuous superiorly with the prominence of the frontal bone, forming the posterior part of the medial margin of the orbit.
Lateral Wall
The lateral wall is roughly triangular and is composed of the zygomatic bone in front and of the greater wing of the sphenoid bone behind (Figure 8-12). The zygomatic bone separates the orbit from the temporal fossa. One or more foramina may be present in the zygomatic bone as a conduit for nerves and vessels between the orbit and facial areas. The lateral or marginal orbital tubercle (Whitnall’s tubercle) is a small, bony prominence located on the orbital surface of the zygomatic bone and is the attachment site for the aponeurosis of the superior palpebral levator muscle, the lateral palpebral ligament, and the lateral check ligament.7
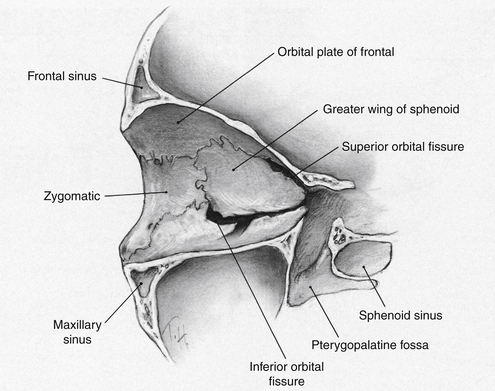
FIGURE 8-12 Bones of lateral orbital wall.
(From Doxanas MT, Anderson RL: Clinical orbital anatomy, Baltimore, 1984, Williams & Wilkins.)
The greater wing of the sphenoid separates the orbit from the middle cranial fossa. The roof is separated from the lateral wall in back by the superior orbital fissure and in front by the frontozygomatic and frontosphenoidal sutures. The inferior orbital fissure separates the posterior part of the floor from the lateral wall (see Figure 8-7).
Orbital Margins
Although dimensions of the orbit vary widely, the average horizontal diameter of the orbital margin is 4 cm, the average vertical diameter is 3.5 cm, and the average depth is 4.5 cm.1,2,8 The frontal bone forms the superior orbital margin. The highest point of this arch is located one-third the way along the margin from the superior medial corner of the orbit. The supraorbital notch (see Figure 8-7) is located just medial to the center of the superior orbital margin and is the conduit for the supraorbital vessels and nerves. This notch can be palpated easily. In 25% of orbits, the supraorbital notch is enclosed to form a foramen.2,9
At the superior medial corner is a less well-defined groove, the supratrochlear notch, through which pass the nerve and vessels of the same name. The supratrochlear notch remains a notch or groove in the majority of orbits, becoming a foramen in just 3%.9
The inferior orbital margin usually is formed equally by the maxillary bone and the zygomatic bone. The zygomaticomaxillary suture can often be easily palpated through the skin along the inferior orbital edge. The infraorbital foramen (the opening from the infraorbital canal) is found in the anterior surface of the maxillary bone below the inferior orbital margin.
The frontal process of the maxillary bone articulates with the frontal bone and forms part of the medial rim of the orbital margin. This process articulates posteriorly with the lacrimal bone and anteriorly with the nasal bone. The medial margin is not continuous. Starting from the inferior nasal aspect, which is the anterior lacrimal crest, the orbital margin forms a spiral (Figure 8-13). The posterior lacrimal crest completes the superior curve of the medial orbital margin.

Orbital Foramina and Fissures
A number of foramina and fissures exist between the orbit and the middle cranial fossa, sinuses, and face to allow the entrance and exit of vessels and nerves that supply the globe and orbital structures. The optic foramen or the optic canal (see Figure 8-7) is formed by a bridge of bone called the “optic strut,” which extends from the lesser wing to the sphenoid body.10 The canal lies just lateral to the body of the sphenoid. The canal often causes an indentation into the bone of the sphenoid sinus.11 It provides communication between the orbital cavity and the middle cranial fossa and is separated from the medial posterior edge of the superior orbital fissure by the optic strut. The optic nerve exits and the ophthalmic artery enters the orbit through this canal (Figure 8-14).
The superior orbital fissure is the gap between the lesser wing and the greater wing of the sphenoid bone and is located between the roof and the lateral wall (see Figure 8-7). As with the optic canal, this fissure is a communication between the orbital cavity and the middle cranial fossa. The fissure usually is widest medially, becoming narrower toward the lateral portion. Approximately midway on the lower aspect is a small sharp spur (the lateral rectus spine) that serves as the attachment for the lateral rectus muscle. A circular band of connective tissue, the common tendinous ring (or annulus of Zinn), is located anterior to the fissure and the optic canal. This ring is the origin for the four rectus muscles. Figure 8-15 shows the relationships among the superior orbital fissure, the tendinous ring, and the various nerves passing through them. The lacrimal nerve, frontal nerve, trochlear nerve, and superior ophthalmic vein pass through the superior orbital fissure above the circular tendon. The superior and inferior divisions of the oculomotor nerve, the nasociliary nerve, and the abducens nerve pass through the fissure and the ring tendon. The optic nerve and the ophthalmic artery pass through the optic canal and the tendinous ring.
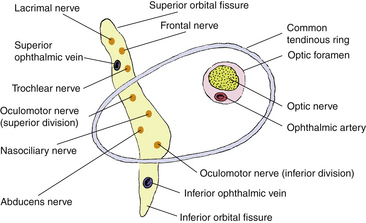
The inferior orbital fissure lies between the floor of the orbit and the lateral wall (see Figure 8-7). It allows passage of vessels and nerves between the orbit and the pterygopalatine and temporal fossae. This fissure often is narrowest in its center. The foramen rotundum opens into the pterygopalatine fossa and transmits the maxillary division of the trigeminal nerve to the inferior orbital fissure. Branches of the maxillary nerve, including the infraorbital nerve, join vessels passing through the inferior orbital fissure. Most of these structures continue into the infraorbital groove in the maxillary bone. The inferior ophthalmic vein exits the orbit through the inferior orbital fissure below the ring tendon.
Clinical Comment: Optic Nerve Damage
The dura mater lining the optic canal is adherent to both the dura of the optic nerve and the periosteum of the canal. This close confinement of the nerve within the bony passage predisposes the nerve to compression and damage by even very small lesions or tumors of the bony canal.12
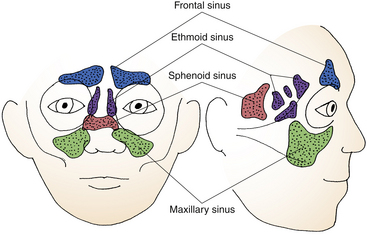
Paranasal Sinuses
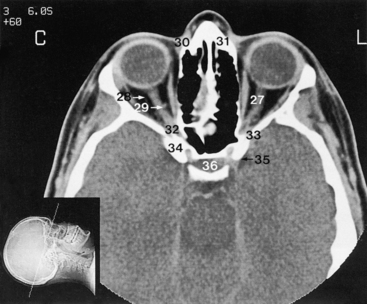
The orbit is surrounded on three sides by sinuses (Figure 8-16): the frontal sinus above, the ethmoid and sphenoid sinus cavities medial to, and the maxillary sinus below the orbit. Of these, the maxillary sinus is largest. The roof of the maxillary sinus is the orbital plate of the maxilla; this plate, only 0.5 to 1 mm thick, separates the sinus from the orbital contents.1 The sphenoid sinus is within the body of the sphenoid and, in some individuals, continues into the lesser wing and may surround the optic canal.1 The ethmoid sinus sometimes continues into the lacrimal bone or into the frontal process of the maxilla.13 In a high percentage of orbits, the thin bone of both the sphenoid and the ethmoid sinuses makes contact with the dural sheath of the optic nerve.14,15 Table 8-1 shows the location of each of the sinus cavities.
| Sinus | Location |
|---|---|
| Frontal | In frontal bone, on each side of midline, superior to orbits |
| Ethmoid | Several air cells on both sides of perpendicular plate of ethmoid bone, medial to orbits |
| Sphenoid | In body of sphenoid bone, posterior and medial to orbits |
| Maxillary | In each maxillary bone, inferior to orbits |
Clinical Comment: Orbital Cellulitis
The thin walls of the sinus cavities are poor barriers to the passage of infection from the air cavities into the orbit. If pathogens from a sinusitis penetrate the thin, bony barrier, a serious infection involving the orbital contents might ensue. A major infection that involves the orbital connective-tissue contents is called orbital cellulitis, and one of its major causes is sinusitis.2,3,16,17 Signs and symptoms include sudden onset of pain, edema, proptosis, and a decrease in ocular motility. Orbital cellulitis is a serious medical situation because of the relatively easy access to the brain through orbital foramina and fissures and must be treated aggressively; hospitalization may be required.3,16 Orbital cellulitis also is a possible sequela of a blow-out fracture, which can (but rarely does) provide a pathologic avenue between the sinus cavities and the orbit that results in orbital infection.18
Orbital Connective Tissue
The connective tissue of the orbit is arranged in a complex network that serves to line, cover, and separate orbital structures; to anchor soft tissue structures to bone; and to compartmentalize areas. Although this network is continuous, the segments are described here individually according to their position and function.
Periorbita
The periorbita, also called the orbital periosteum or orbital fascia, covers the bones of the orbit (Figure 8-17). This dense connective tissue membrane serves as an attachment site for muscles, tendons, and ligaments and is a support structure for the blood supply to the orbital bones. The periorbita is attached only loosely to the underlying bone except at the orbital margins, the sutures, and the edges of fissures and foramina. At the orbital margins it is continuous with the periosteal covering of the bones of the face; at the edges of the superior orbital fissure, the optic canal, and the ethmoid canals, the periorbita is continuous with the periosteal layer of the dura mater. At the anterior portion of the optic canal, the periorbita splits such that a portion becomes continuous with the dura of the optic nerve and another portion reflects forward to take part in the formation of the common tendinous ring. At the inferior orbital fissure the periorbita is continuous with the periosteum of the skull. At the lacrimal crests a sheet of periorbita covers the lacrimal sac, and the periorbita is continuous with the tissue lining the nasolacrimal canal. Another portion of the periorbita covers the lacrimal gland.
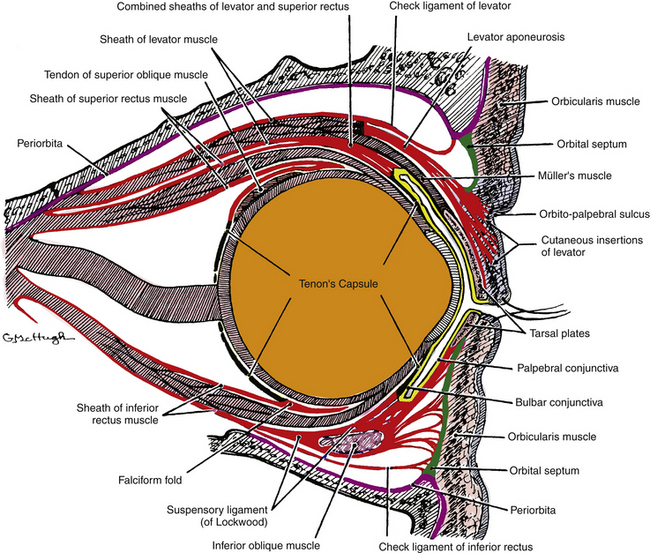
Orbital Septum
At the orbital margins the periorbita is continuous with a connective tissue sheet known as the orbital septum, also termed the palpebral fascia or septum orbitale. This dense connective tissue sheet is circular and runs from the entire rim of the orbit to the tarsal plates, which are embedded in the eyelids. This strong barrier helps prevent facial infections from entering the orbit; it also maintains orbital fat in its place. Figures 8-17 and 8-18 show the relationships between orbital structures and these connective tissue structures. At the lateral margin the orbital septum lies in front of the lateral palpebral ligament and the check ligament for the lateral rectus muscle.7 At the superior orbital margin the orbital septum passes in front of the trochlea and bridges the supraorbital and supratrochlear notches. At the medial margin the orbital septum, which attaches behind the posterior lacrimal crest, lies in front of the check ligament for the medial rectus muscle; it lies behind the medial palpebral ligament, Horner’s muscle, and the lacrimal sac (see Figure 8-18), isolating the lacrimal sac (which communicates with the nasal cavity) from the orbit proper.
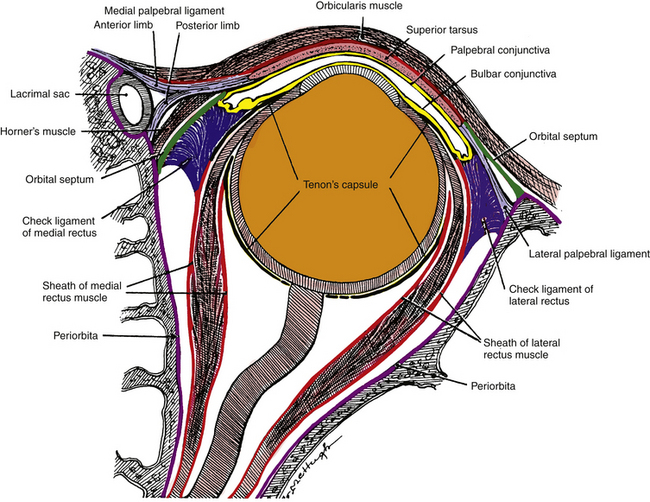
Tenon’s Capsule
Tenon’s capsule (bulbar fascia) is a sheet of dense connective tissue that encases the globe.19 It lies between the conjunctiva and the episclera and merges with them anteriorly in the limbal area. Tenon’s capsule is pierced by the optic nerve, the vortex veins, the ciliary vessels and nerves, and the extraocular muscles. At the muscle insertions, Tenon’s capsule forms sleevelike sheaths that cover the tendons.2,20 Posteriorly, Tenon’s capsule merges with the dural sheath of the optic nerve. This dense connective tissue capsule acts as a barrier to prevent the spread of orbital infections into the globe.
Suspensory Ligament (of Lockwood)
The suspensory ligament (of Lockwood) (see Figure 8-17) is a hammocklike sheet of dense connective tissue that runs from its attachment on the lacrimal bone at the medial orbital wall to the zygomatic bone at the lateral wall. Tissue from several structures—Tenon’s capsule, the sheaths of the two inferior extraocular muscles, and the inferior eyelid aponeurosis—contributes to the formation of this ligament. The suspensory ligament helps to support the globe, particularly in the absence of the bones of the orbital floor.
Orbital Muscle of Müller
The orbital muscle of Müller is a small, smooth muscle embedded in the periorbita and covering part of the inferior orbital fissure.6,21 Its function in humans is unknown.
Orbital Septal System
A complex web of interconnecting connective tissue septa organize the orbital space surrounding the globe into radial compartments. Collagenous strands connect the periorbita to Tenon’s capsule and intermuscular membranes. This connective tissue system of “slings” anchors and supports the extraocular muscles and blood vessels, attaching them to adjacent orbital walls.22 The slings associated with each of the muscles maintain correct positioning of the muscles during eye movements. Varying degrees of connectivity occur throughout the orbit (see Figures 10-11 and 10-12).
Orbital Fat
The spaces not occupied by ocular structures, connective tissue, nerves, or vessels become filled with adipose tissue. Usually, four adipose tissue compartments are located within the muscle cone surrounding the optic nerve and separating it from the extraocular muscles.6,23 A ring of adipose tissue separates the muscles from the walls of the orbit, and adipose is the predominant tissue near the orbital apex.6 Because of the close association of the orbital contents, a space-occupying lesion will cause outward displacement of the globe.
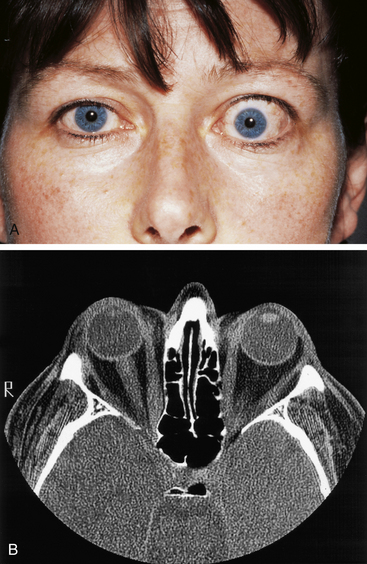
Clinical Comment: Exophthalmos
Protrusion of the globe is termed exophthalmos, or proptosis (Figure 8-19). It can be caused by a number of pathologic conditions, including inflammation, edema, tumors, and injuries.16 The most common type is thyroid ophthalmopathy (dysthyroid orbitopathy, Graves’ disease), which can cause hypertrophy of the extraocular muscles; in some patients the muscles become enlarged to eight times their normal size.3 Thyroid ophthalmopathy also causes proliferation of orbital fat and connective tissue, and lymphoid infiltration.3 Because the orbital tissue is encased in immovable bony walls, this increase in volume of the orbital contents produces protrusion of the globe and simulates eyelid retraction. At the first sign of proptosis, investigation is necessary to determine the causative factor.
1. Warwick R. Eugene Wolff’s anatomy of the eye and orbit, ed 7. Philadelphia: Saunders; 1976. pp 1, 8, 15, 19
2. Doxanas M.T., Anderson R.L. Clinical orbital anatomy. Baltimore: Williams & Wilkins; 1984. pp 20, 25, 117
3. Kanski J.J. Clinical ophthalmology, ed 3. London: Butterworth-Heinemann; 1994. pp 33, 52
4. Forrest L.A., Schuller D.E., Strauss R.H. Management of orbital blow-out fractures. Am J Sports Med. 1989;17(2):217-220.
5. Taher A.A. Diplopia caused by orbital floor blowout fracture. Oral Surg Oral Med Oral Pathol. 1993;75(4):433-435.
6. Koornneef L. Orbital connective tissue. In: Jakobiec F.A., editor. Ocular anatomy, embryology, and teratology. Philadelphia: Harper & Row; 1982:835.
7. Rosenstein T., Talebzadeh N., Pogrel M.A. Anatomy of the lateral canthal tendon. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89(1):24-28.
8. Reeh M.J., Wobig J.L., Wirtschafter J.D. Ophthalmic anatomy. San Francisco: American Academy of Ophthalmology; 1981. p 11
9. Webster R.C., Gaunt J.M., Hamdan U.S., et al. Supraorbital and supratrochlear notches and foramina: anatomical variations and surgical relevance. Laryngoscope. 1986;96(3):311-315.
10. Sires B.S., Gausas R., Cook B.E.Jr., et al. Orbit. In: Kaufman P.L., Alm A., editors. Adler’s physiology of the eye. St Louis: Mosby, 2003. p 11
11. Goldberg R.A., Hannai K., Toga A.W. Microanatomy of the orbital apex. Computed tomography and microcryoplaning of soft and hard tissue. Ophthalmology. 1992;99(9):1447-1452.
12. Lang J., Kageyama I. The ophthalmic artery and its branches, measurements, and clinical importance. Surg Radiol Anat. 1990;12(2):83-90.
13. Blaylock W.K., Moore C.A., Linberg J.V. Anterior ethmoid anatomy facilitates dacryocystorhinostomy. Arch Ophthalmol. 1990;108(12):1774-1777.
14. Bansberg S.F., Harner S.G., Forbes G. Relationship of the optic nerve to the paranasal sinuses as shown by computed tomography. Otolaryngol Head Neck Surg. 1987;96(4):331-335.
15. Cheung D.K., Attia E.L., Kirkpatrick D.A., et al. An anatomic and CT scan study of the lateral wall of the sphenoid sinus as related to the transnasal transethmoid endoscopic approach. J Otolaryngol. 1993;22(2):63-68.
16. Berkow R., editor. The Merck manual, ed 14, Rahway, NJ: Merck, 1982. p 1984
17. Mills R.P., Kartush J.M. Orbital wall thickness and the spread of infection from the paranasal sinuses. Clin Otolaryngol. 1985;10(4):209-216.
18. Silver H.S., Fucci M.J., Flanagan J.C., et al. Severe orbital infection as a complication of orbital fracture. Arch Otolaryngol Head Neck Surg. 1992;118(8):845-848.
19. Tenon J.R., Naus J., Blanken R. Anatomical observations on some parts of the eye and eyelids. Strabismus. 2003;11(1):63-68.
20. Eggers H.M. Functional anatomy of the extraocular muscles. Tasman W., Jaeger E.A., editors. Duane’s foundations of clinical ophthalmology, vol 1. Philadelphia: Lippincott, 1994.
21. Rodríguez-Vázquez J.F., Mérida-Velasco J.R., Jiménez-Collado J. Orbital muscle of Müller: observations on human fetuses measuring 35-150 mm. Acta Anat (Basel). 1990;139:300-303.
22. Dutton J.J. Clinical and surgical orbital anatomy. Ophthalmol Clin North Mm. 1996;9(4):527.
23. Wolfram-Gabel R., Kahn J.L. Adipose body of the orbit. Clin Anat. 2002;15(3):186-192.
[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
Chapter 8 Bones of the Skull and Orbit
Bones of the Cranium
The paired parietal bones form the roof and sides of the cranium (Figure 8-1). The parietal bones articulate with each other at the midline in the sagittal suture, with the occipital bone posteriorly in the lambdoid suture, and with the frontal bone anteriorly at the coronal suture. The parietal bone articulates inferiorly with the temporal bone and the greater wing of the sphenoid bone.
FIGURE 8-1 Lateral view of skull.
(From Mathers LH, Chase RA, Dolph J et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
The occipital bone forms the posterior aspect of the skull and posterior floor of the cranial cavity. A prominence, the external occipital protuberance, or inion, is found on the external surface at the posterior midline (Figure 8-2). The large foramen magnum is found in the inferior aspect of the occipital bone. The inner surface of the bone forms the posterior cranial fossa, in which there are depressions where the lobes of the cerebellum lie. Figure 8-3 shows the inner aspect of the cranial floor. The occipital bone articulates with the temporal bones, parietal bones, and sphenoid bone.
FIGURE 8-2 Posterior view of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
FIGURE 8-3 Floor of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
Bones of the Face
The single frontal bone forms the forehead and articulates with the nasal bones, maxillae, and zygomatic bones in formation of the face (see Figure 8-4). The sutures joining adjacent bones of the face generally are named according to the names of the two bones that are connected (e.g., the suture between the frontal bone and the zygomatic bone is the frontozygomatic suture).
The two maxillae, or maxillary bones, form the upper jaw, the hard palate, the lateral walls of the nasal cavity, and the floor of both orbits (see Figure 8-4). Each maxillary bone articulates with the frontal, nasal, lacrimal, ethmoid, sphenoid, palatine, and zygomatic bones. That portion of the maxillary bone forming the cheek contains the maxillary sinus.
Each of the temporal bones is composed of two portions: a large, flat plate, the squamous portion; and a thickened, wedge-shaped area, the petrous portion. The squamous portion forms the side of the cranium and articulates with the parietal bone and the sphenoid bone. An anterior projection, the zygomatic process, articulates with the zygomatic bone (see Figure 8-1). The petrous portion extends within the cranium and houses the middle and inner ear structures. The mastoid process and styloid process project from the inferior aspect, and between these two processes is the stylomastoid foramen, through which the facial nerve exits the skull. The petrous portion articulates with the occipital bone in the floor of the skull. The carotid canal runs superiorly and anteriorly through the petrous portion and provides an entrance for the internal carotid artery into the cranial cavity (Figure 8-3).
The single frontal bone forms the anterior portion of the cranium, anterior floor of the cranial cavity, and superior part of the face (Figure 8-4). At the top of the skull, the frontal bone articulates with the parietal bones; inferiorly it articulates with the sphenoid bone, ethmoid bone, and lacrimal bones. Inferoanteriorly, it articulates with the nasal bones, maxillary bones, and zygomatic bones. The inner surface of the cranial cavity portion of the frontal bone forms the anterior cranial fossa (see Figure 8-3), in which the frontal lobes of the cerebral hemispheres lie. The frontal sinuses are located within the anterior portion of the frontal bone.
FIGURE 8-4 Anterior view of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
The sphenoid bone is a single bone, the body of which lies in the midline and articulates with the occipital bone and the temporal bones to form the base of the cranium (see Figure 8-3). The sphenoid bone joins the zygomatic bones to form the lateral walls of the orbits. Anteriorly and inferiorly the sphenoid bone articulates with the maxillary and palatine bones, superiorly with the parietal bones, and anteriorly and superiorly with the ethmoid and frontal bones. The depression on the superior cranial surface of the body of the sphenoid bone, the hypophyseal fossa (or the sella turcica), houses the pituitary gland; a portion of the body is hollow, forming the sphenoid sinus cavity.
Two pairs of wings project from the body of the sphenoid bone. The lesser wings project from the anterior aspect of the body and are more superior and smaller than the greater wings (see Figure 8-3). The lesser wings are attached to the body by small roots or struts. The gap between the lesser wing and the sphenoid body forms the optic foramen (canal) through which the optic nerve exits the orbit. The lesser wings articulate with the frontal and ethmoid bones.
The greater wings project from the lateral aspects of the body and articulate with the frontal bone, the parietal bones, squamous portions of the temporal bones, and the zygomatic bones. The pterygoid process projects from the base of the greater wing and articulates with the vertical stem of the palatine bone; each contributes to a shallow depression, the pterygopalatine fossa. Three important foramina are located in the greater wing (Figure 8-5): the foramen rotundum, through which the maxillary nerve passes; the foramen ovale, through which the mandibular nerve passes; and the foramen spinosum, through which the middle meningeal artery passes.
FIGURE 8-5 Disarticulated view of base of skull.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
The two nasal bones form the bridge of the nose and articulate with each other, with the frontal bone, and with the frontal processes of the maxillary bones (see Figure 8-4). The vomer is a single bone that forms the posterior part of the nasal septum. It articulates with the palatine and maxillary bones inferiorly and with the ethmoid bone superiorly. The inferior conchae are separate bones located along the lateral walls of the nasal cavity.
The paired zygomatic bones form the lateral part of the cheekbones and articulate with the zygomatic process of the temporal bones to form the zygomatic arches (see Figure 8-1). The zygomatic bones also articulate with the maxillary bones and with the greater wings of the sphenoid bone.
The Orbit
The orbit is shaped like a four-sided pyramid, the base of which is at the anterior orbital margin and the apex at the posterior margin within the skull. The orbital walls are referred to as the roof, floor, and medial and lateral walls. The medial walls run approximately parallel to each other, whereas the two lateral walls, if extended posteriorly, would form approximately a 90-degree angle with each other1,2 (Figure 8-6). The orbit has also been described as pear shaped, having its widest portion 1.5 cm inside the orbital margin.1 The orbital floor extends to approximately two-thirds the depth of the orbit; the other three sides extend to the apex.
Each orbit is composed of seven bones—the frontal, maxillary, zygomatic, sphenoid, ethmoid, palatine, and lacrimal bones (Figure 8-7). The frontal, sphenoid, and ethmoid are each a single bone and take part in the formation of both orbits.
FIGURE 8-7 Anterior view of bones of orbit.
(From Mathers LH, Chase RA, Dolph J, et al: Clinical anatomy principles, St Louis, 1996, Mosby.)
Orbital Walls
Roof
The roof is triangular and is composed primarily of the orbital plate of the frontal bone in front (Figure 8-8). The lesser wing of the sphenoid contributes a small posterior portion. The orbital plate of the frontal bone is thin in the area that separates the orbit from the anterior cranial fossa. In an elderly adult, bone in this area may resorb, leaving only the periosteal connective tissue in contact with the dural covering of the frontal lobe of the brain. The small area of the lesser wing of the sphenoid that is involved in this wall runs slightly downward, and an oval foramen, the optic canal, lies between it and the body of the sphenoid (see Figure 8-7). This optic foramen is located roughly at the apex of the orbit.
Floor
The floor is also triangular and is composed of the orbital plate of the maxillary bone and the orbital plate of the zygomatic bone in front and the small orbital process of the palatine bone behind (Figure 8-9
[/not-level-membership-for-basic-science-category]
