CHAPTER 10 AUTISM AND ATTENTION DEFICIT/HYPERACTIVITY DISORDER
Autism and attention deficit hyperactivity disorder (ADHD) are the two main classes of neurodevelopmental disorders that begin in early childhood. The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR)1 specifies that the diagnosis of ADHD cannot be made if the symptoms occur in a child with autism. However, symptoms of attention deficit and hyperactivity are common problems in children with autism, which points toward some neuropathophysiological characteristics shared between these two groups of neurodevelopmental disorders. Autism is a generic term referring to a group of related conditions defined in the DSM-IV-TR1 and the International Classification of Diseases, Tenth Revision (ICD-10),2 as pervasive developmental disorders. The term autistic spectrum disorders is frequently used but lacks any international agreement regarding its definition.3 The term is sometimes used to refer to a group of related conditions similar to pervasive developmental disorders. It is also used to describe the range of intellectual abilities, from severe disability to normal ability, found in children with autism. The concept of a spectrum has also been applied to describe developmental changes, such as improvement in language ability, which might occur over time in an individual with autism. In this chapter, autism refers to the pervasive developmental disorders, which share the core features of severe and pervasive impairment in social and communication skills, together with the presence of restricted and repetitive patterns of behavior and interests. The onset of these disorders occurs within the first 3 years of life, but the clinical picture may change with development. In DSM-IV-TR1 the pervasive developmental disorders comprise the categories of Autistic Disorder, Asperger Disorder, Rett’s Disorder, Childhood Disintegrative Disorder, and Pervasive Developmental Disorder–Not Otherwise Specified (PDD-NOS). Autism was first described by Leo Kanner in 1943 for a group of 11 children who had the distinctive core features of social, language, and communication disturbance and an obsessive desire for sameness.4 In the following year, Hans Asperger described a group of 16 children and adolescents who had deficits in communication and social skills together with obsessional interest, intolerance of change, and motor clumsiness.5 Unlike the children described by Kanner, these young people were of normal intellectual ability and did not have any delay or abnormality in their language development. This has become the differentiating feature of Asperger’s disorder from autistic disorder. This review focuses on the assessment, pathophysiologic aspects, and treatment of the two main pervasive developmental disorders, autistic disorder and Asperger’s disorder.
The problem of excessive hyperactive, inattentive, and impulsive behavior in children has been described in the medical literature from the 19th century.6 Current theories regarding the etiology of developmentally excessive inattentiveness and hyperactivity encompass an interaction of genetic predisposition, central nervous system dysfunction resulting from prenatal and early postnatal traumatic or toxic events, and environmental and social influences. The concept of minimal brain damage with associated soft neurological signs led to theories of dysfunction of the thalamus and prefrontal circuits to account for the hyperactivity and inattention, respectively. Current interest is focused on deficiencies of executive function and inhibition of attention resulting from such dysfunction, particularly affecting the right prefrontal cortex and associated basal ganglia structures.7 These primary deficits affect the development of working memory, emotional regulation, motivation, and the development of language and morality.7 Historically, the approach to the diagnosis of ADHD has differed between North America and Europe. Clinicians in Europe have sought for evidence of neurological dysfunction and pervasive symptoms of inattention and hyperactivity in all contexts. Clinicians in North America have taken a more qualitative approach to diagnosis, acknowledging that symptoms may vary in different settings and subdividing the diagnosis into the number of symptoms in each of the dimensions of inattention or hyperactivity/impulsiveness. Thus, a child may receive a diagnosis of ADHD predominantly hyperactive type or predominantly inattentive type. There has been an attempt to bring the diagnostic criteria for ADHD in the DSM-IV-TR into line with the criteria for hyperkinetic disorder in the ICD-10.2 Although the criteria used in both classification systems are now virtually identical, there are still differences regarding the number of criteria required and the pervasiveness of symptoms. As a consequence, application of ICD-10 criteria is more restrictive and conservative, which has implications for studies of epidemiology and etiology. The discovery in 1937 of the therapeutic effect of dextroamphetamine on concentration and hyperactivity in children with disruptive behavior has also influenced approaches to diagnosis and the interest taken by society in these behavioral problems.8
Regardless of an element of social determinism inherent in the diagnosis of ADHD, there is no doubt that young people with pervasive difficulties with attention, impulsiveness, and motor hyperactivity are at great risk of suffering educational, social, emotional, and behavioral problems during childhood and subsequent mental health, relationship, occupational, forensic, and substance abuse problems in adult life. This chapter focuses on advances in the understanding of the neuropathophysiology and treatment of ADHD.
EPIDEMIOLOGY
Autism
There is evidence that the prevalence of autism is increasing. More than 23 prevalence studies of autism have been reported in the literature from 1966 to 1997. In most studies before 1990, investigators reported prevalence rates of 4 to 5 per 10,000. In more recent studies in which rigorous diagnostic criteria and standardized diagnostic assessment were used, investigators have found rates of approximately 10 to 12 per 10,000.9 Since the mid-1990s in a number of countries, specialist children’s services have reported an increasing demand for services for children with autism. For example, in Iceland, the prevalence of autism and the demand for services are reported to have doubled.10 Reviews indicate that the apparent increase in prevalence is probably a result of differences in ascertainment and diagnosis and an increasing awareness of autism by the general public.9 At least 14 different approaches to diagnosis have been used in prevalence studies. For example, when DSM-IV-TR or ICD-10 diagnostic criteria are used, the prevalence of autism is two to three times higher than that found with the application of the earlier criteria of Kanner.9 The inclusion of subcategory diagnoses of pervasive developmental disorders such as PDD-NOS or atypical autism leads to further increases of prevalence to approximately 27 to 30 per 10,000.9 In several longitudinal studies, researchers using equivalent methods of diagnosis over time, but with relatively small sample sizes, have not found significant changes in prevalence rates in subsequent birth cohorts.9,11
There is no evidence that prevalence varies between countries or racial groups, and social class and level of parental education are not associated with autism.9 Autistic disorder is more common in boys than in girls (ratio, 4:1), and the gender distribution is even more marked for Asperger’s disorder (ratio, 10:1 to 13:1). This gender distribution might point to the possibility of an X-linked element to the disorder, but research has failed to confirm this explanation.
Attention Deficit/Hyperactivity Disorder
Estimates of the prevalence of ADHD vary widely according to the diagnostic criteria, measures used, ascertainment methods, and demographics of the population. For example, in a populationwide study in the United States in which parent- and self-report screening questionnaires were used, a prevalence of ADHD of up to 20% was identified.12 Population rates of 1% to 2% are found if prevalence is based on the application of the restrictive ICD-10 criteria2 without the presence of comorbid conditions.13 Prevalence rates of 5% to 10% are found in studies in which the more inclusive DSM-IV-TR criteria, which allow some variability of symptoms and the presence of comorbidity, are used.14
Studies with DSM-IV-TR criteria reveal that the combined inattentive-hyperactive subtype of ADHD is the most common manifestation. For example, a clinic study demonstrated that 60% of young people with a diagnosis of ADHD had the combined subtype, 30% had the inattentive subtype, and 10% had the hyperactive-impulsive subtype.15 Note that the subtypes are designated on the basis of symptom predominance; meeting criteria for one subtype, such as inattentive subtype, does not preclude the presence of some symptoms from another subtype, such as hyperactive symptoms. Community studies reveal that the childhood prevalence of ADHD is approximately three times higher in boys than in girls but is more likely to decrease over time in male patients while remaining stable into adulthood in female patients.16
Symptoms usually reduce with maturation, but at least 30% of children with ADHD continue to suffer from the disorder in adulthood.17 Because of differences in diagnostic criteria and methods of ascertainment, the prevalence of ADHD in adults varies between 0.3% and 5%.17 Approximately a third of these adults are likely to suffer from a comorbid affective disorder as well, and the majority have associated social, marital, employment, and legal problems.18
CLINICAL FEATURES
Autism
Autism manifests with delays and abnormalities in the development of language and social skills, and the presence of rigid, repetitive, stereotyped play and behavior, often in association with intellectual disability and a variety of neurological conditions such as epilepsy. Therefore, the assessment and diagnosis is multifaceted, involving medical, cognitive, language, developmental, and mental state assessments.19 A reliable diagnosis can be made in patients aged 2 years and older. In view of the value of early intervention, early diagnosis is important and can be facilitated with the use of screening tools completed by parents (e.g., the Developmental Behavior Checklist),20 and clinician-completed checklists (e.g., the Checklist for Autism in Toddlers).21 Diagnosis is enhanced by the use of a structured, reliable, and valid parental interview and child observation schedule,22 such as the Autism Diagnostic Interview/Revised23 and the Autism Diagnostic Observation Schedule.24
All children with autism have impaired social interactions, which may change as they develop. Infants with autism do not anticipate social interactions, such as being picked up, or seek physical comfort or parental attention. Preschool children with autism usually avoid eye contact and do not engage in social imitation such as waving goodbye. They are unresponsive to the feelings and emotions of others. They are aloof and unable to engage effectively with other children or understand reciprocal social interactions. As such children grow older, there may be an increased interest in other people, but social skills are often stilted and learned in an inflexible manner, leading the children to appear odd and socially clumsy. Parents usually first seek help because their children have language delay and a lack of nonverbal communication and easily becomes frustrated. About 50% of children with autism fail to develop functional speech and learn only slowly to compensate with gesture. Language development is often abnormal in the remainder, with echolalia, self-directed jargon, and the repetition of irrelevant phrases (for example, from a television show). The correct use of pronouns and the related development of a sense of self and others are delayed. Poor comprehension, problems expressing needs by words and gesture, and difficulty in social understanding are frequently the causes of frustration and disturbed behavior. Children who do develop functional language usually have difficulty in using language socially and in initiating or sustaining a reciprocal conversation. For example, the child may talk at others in a socially inappropriate manner. In contrast to children with autistic disorder, young people with Asperger’s disorder have no delay in the development of normal expressive and receptive language, including the use of communicative phrases by the age of 3 years. However, children with Asperger’s disorder have problems in their social use of language, such as being verbose and preoccupied with a favorite topic. Their speech may appear odd because of the use of an unusual accent or because of the presence of abnormalities in pitch and volume; for example, delivery may be flat and monotonous.
Children with autism often have a range of disruptive behaviors such as stubbornness, self-injury, and aggression, which place a high burden of care on parents and teachers. These disruptive behaviors are the main cause of failure in school and community activities and lead to more restrictive care. High levels of anxiety are common and prevent these children from learning, coping with change, and participating in family and community activities. The anxiety associated with autism is likely to persist into adult life.25 Children with autism are also likely to suffer from depression, particularly during adolescence. This may manifest as mood disturbance and irritability, sleep and appetite disturbance, and thoughts of suicide, which may be enacted.26 The increased vulnerability to depression during adolescence may be associated with self-awareness of the disability, but pubertal brain development and a family history of depression may also contribute.
At least 13% of children with autism also meet diagnostic criteria for ADHD,27 but the DSM-IV-TR specifically precludes the diagnosis of ADHD “during the course of a Pervasive Developmental Disorder” (p. 93).1 Nevertheless, symptoms of attention deficit and hyperactivity in children with autism impede and disrupt their learning, school adjustment, and family life. These symptoms of ADHD are responsive to educational, behavioral, and pharmacological managements used for children with ADHD, although not always as successfully.26 Children with autism also have an increased risk of suffering tic disorder or Gilles de la Tourette syndrome, with the tics becoming more prevalent during times of stress and anxiety, such as a change in school placement.26 Epilepsy occurs in approximately 20% of young people with autism, emerging most commonly in early childhood or during adolescence. It is seen more frequently in children with more severe levels of intellectual disability.26 Young people with Asperger’s disorder also suffer from a similar range of mental health problems but are even more likely to have higher levels of disruptive and antisocial behavior and to suffer from anxiety and depression.28 They may also have an increased risk of developing psychosis during adolescence or early adult life.
Attention Deficit/Hyperactivity Disorder
The diagnosis of ADHD is based on a clinical judgment that there are sufficient symptoms of inattention and hyperactivity/impulsivity, together with the decision that these symptoms cause significant impairment in daily functioning in at least two settings and are not consistent with the developmental level of the child.1 Therefore, the diagnosis requires a careful and comprehensive history of the child’s development and behavior from the parents and other informants such as the teacher, together with observation of the child during both structured and unstructured activities. A structured cognitive assessment, apart from providing information on specific learning difficulties and related problems such as deficits in short-term auditory memory, also reveals problems with concentration and distractibility—that is, with sustained, directed attention. The use of structured behavior rating scales, such as the Conner’s Parent and Teacher Rating Scales,29 may be useful for screening and as a measure of response to treatment.
Apart from high levels of distractibility and inattention, children with ADHD are disorganized and are usually unable to follow routine or complete tasks.1 They have difficulty monitoring their behavior and therefore often interrupt others, have difficulty following rules, and display inappropriate and impulsive behavior.1 Those who also suffer from hyperactivity are constantly restless and fidgety, have difficulty remaining seated, and behave as if they are driven by a motor. These behaviors are influenced by aspects of the environment, such as the degree of external stimulation and sensory complexity. Therefore, observers may report differences in behavior, depending on the context. For example, a teacher in a busy, noisy classroom setting is more likely to observe inattention than is a teacher’s aide who has the child for individual teaching in a quiet library environment. However, the symptoms and impairments are usually observed, at least to some extent, in all aspects of the child’s daily life.
Young people with ADHD have a range of associated problems. Their primary symptoms often lead to hostile interactions with other children, who may reject them. ADHD is frequently complicated by the presence of other psychopathological conditions: in particular, conduct disorder (25%), oppositional defiant disorder (35%), depression (15%), and anxiety disorder (25%).30 The majority of children with ADHD have various learning difficulties and poor school performance in relation to their intellectual abilities.31 Approximately 25% of individuals with ADHD have intellectual disability, including delayed language development.31
Children with ADHD have difficulty falling asleep and wake early, and their sleep is often unsettled and complicated by breathing and snoring difficulties.32 Adolescents with ADHD are at risk for delinquent behavior and abuse of nicotine, alcohol, and other substances, perhaps as a means of self-medication.33 Young people who are treated with stimulant medication for ADHD are less likely to use substances than are adolescents with ADHD who are not receiving treatment.33 There is also an association between the use of alcohol, tobacco, and other substances during pregnancy and the birth of a child with ADHD, but the mechanisms for these associations are likely to reflect the complex interaction of genes and environment.33
The assessment and diagnosis of ADHD for the first time in adults is difficult.34 Such an adult may not be living in a situation in which others can report on behaviors and symptoms to help the clinician reach a judgment on the severity of symptoms and the degree of disability. The presence of other comorbid psychiatric illnesses complicates the presentation. Adults are not able to reliably remember their childhood; therefore, if possible, a history of the manifestation of the disorder throughout childhood should be obtained from other persons or from school reports.34 Adults with ADHD are usually less disruptive and hyperactive than are children with ADHD, but they usually remain impulsive, disorganized, inattentive, and restless.34
ETIOLOGY AND PATHOPHYSIOLOGY
Autism
Neurocognitive Theories
There are three main cognitive theories of autism: the “theory-of-mind,”35 the “executive dysfunction” theory,36 and the theory of “weak central coherence.”37 Deficiencies in theory-of-mind—that is, the ability to understand that other people have unique perspectives and thoughts that are sometimes contextually independent—are thought to be linked to the social-communicative deficits associated with autism.35 Weak central coherence, a deficit in the ability to integrate details into a coherent global perception, is thought to be linked to the tendency of individuals with autism to be preoccupied with parts of objects and to miss the “bigger picture.”37 Executive functioning refers to the role of the frontostriatal circuits in coordinating cognitive-motor output so that behavior is well timed, planned, adaptable, appropriate, and relevant38 (and see Chapter 7). The repetitive, stereotyped, and restricted behaviors seen in autism are thought to result, in part, from deficient executive functioning.39 Poor performance on tests of executive functioning “… is found more consistently in autism than in any other form of childhood psychopathology” (p. 103).40
It is not clear which, if any, of these cognitive deficits is central to the psychiatric and neurological symptoms that characterize autism.41 Volkmar and colleagues42 argued that the main criticism leveled at theory-of-mind is that it cannot account for the clinical phenomenology of autism, because the social deficits characteristic of autism appear at a point in development before normally developing children demonstrate the acquisition of a theory-of-mind. Furthermore, children with autism and normal intelligence are reported to perform at an age-appropriate level on theory-of-mind tasks,43 although some authors disagree with this conclusion.44,45 Other, more primary deficits reflect problems with “weak central coherence.” Studies suggest that problems in moving attentional focus away from the detail of an object may better account for why individuals with autism appear to get “stuck” on detail and have a poor ability to appreciate the object’s gestalt.46,47
The broader executive dysfunction theory of autism (including attentional dysfunction) is perhaps the most appealing theory from a cognitive neuroscience perspective, inasmuch as it enables the linking of more specific cognitive deficits to possible impairments in specific neurological circuitries. Contemporary cognitive research has focused on uncovering distinct executive functioning profiles48 that might distinguish children with autism from those with other neurodevelopmental disorders: for example, ADHD, obsessive compulsive disorder, Gilles de la Tourette disorder, schizophrenia, and depression.49 Standardized neuropsychological tests—for example, the Wisconsin Card Sort Test, the Tower of Hanoi, and the Stroop Color-Word Test—have demonstrated that the profile of autism is characterized primarily by deficient cognitive flexibility and planning,48 with intact sustained and directed attention50 and intact cognitive inhibition.48 However, results of attempts to measure impairment of cognitive inhibition in autism with novel approaches that align more closely to a child’s everyday experiences—for example, generating novel verbal utterances, ideas, and drawings—challenge the view that this area of cognition is intact in autism.51,52
Some studies suggest that measures of “motor” functioning in autism may provide a more useful neurobiological probe than do more complex cognitive-social measures, which do not define discrete neural pathways.53,54 Motor studies of young people with autism (3 to 21 years of age) demonstrate movement anomalies commensurate with basal ganglia dysfunction.55–57 For example, atypical upper-body motor preparation with intact execution,58 reduced motor evoked potentials,59 and postural abnormalities60 have been reported. Studies of gait in autism also suggest a cerebellar contribution to motor dysfunction: for example,61 gait variability60,61 and difficulty with straight-line walking, which are consistent with a cerebellar ataxic gait disturbance.62
An important issue in the cognitive description of autism is the question of so-called “knock-on” effects: that is, how one potentially primary cognitive deficit may have downstream effects on other emerging skills.41 A neurocognitive comparison of normally intelligent individuals with autism and those with Asperger’s disorder can be used to illustrate the potential “knock on” effects of disordered and delayed language, because this is the clearest point of neurological departure between these disorders in the first 3 years of life. Neurocognitive comparisons of individuals with autism and those with Asperger’s disorder have revealed quantitative and qualitative differences in executive functioning,63,64 which potentially represent downstream neural and environmental consequences of language deficits in autism. For example, executive functioning anomalies show a lateralization pattern consistent with left-hemisphere dysfunction for autism, but not in Asperger’s disorder.65 A better understanding of the primacy of cognitive deficits and how they unfold and link to the psychiatric and neurological symptoms of autism is likely to come from detailed prospective studies of the newborn siblings of autistic children, who are themselves at higher genetic risk of developing autism than are unrelated newborns.
Neuroanatomical and Neuroimaging Studies
There is no consistent neuroimaging marker that has been identified for autism. Structural changes in the brains of individuals with autism include slightly increased average brain volume, decreased gray matter volumes in the limbic system (an area important for social cognition), reduced neuron numbers in the vermis of the cerebellum, and gross structural changes in cerebellum66,67 and the parietal lobes68 (areas important for efficient attention). A reduction in neuronal integrity in prefrontal areas and concurrent abnormalities in the frontal cortex and cerebellum67 possibly underlie the repetitive behavioral symptoms that characterize autism.69 Several imaging studies have uncovered left hemisphere impairment in autism.70 One review71 concluded that although many structural abnormalities have been identified in individuals with autism, the findings are inconsistent and not specific.
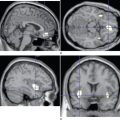
Functional magnetic resonance imaging (fMRI) has the potential to more clearly elucidate the neurobiological substrates that underpin faulty cognitive-motor processes in autism. There have been several attempts to link the social-communicative deficits with particular neural regions using neuroimaging techniques,72–74 but there have been relatively few attempts to study frontal regions associated with executive functioning. A study of the application of fMRI during a mental rotation task75 revealed that individuals with autism and Asperger’s disorder showed decreased activation in the highly interconnected cortical and subcortical frontal structures, including lateral and medial premotor cortex, frontal eye fields, caudate, dorsolateral prefrontal cortex, and anterior cingulate cortex, suggestive of disruption to multiple frontostriatal circuits.
Although advances in the cognitive neuroscience of executive function and attention enable investigators to more clearly study the component processes and anatomical substrates of autism,76 a more comprehensive understanding of the brain-behavior disruption that characterizes autism is likely to come from a larger systematic examination of cognitive processing, in which the cognitive and anatomical specificity afforded by fMRI and event-related methods are used.
Genetic Theories
In fewer than 10% of cases, autism is associated with defined environmental causes, such as rubella and cytomegalovirus, fetal infections, perinatal brain injury, toxins, and specific genetic abnormalities such as tuberous sclerosis and fragile X syndrome.77
A suggested link between measles, mumps, and rubella vaccination and the use of thimerosal in vaccines as a cause of the increased prevalence of autism has been discounted by several comprehensive studies.78 Thimerosal has not been in vaccines in North America and Japan since the mid-1990s, during the time of reported increases in prevalence.
The cause of the majority of cases remains unknown, but they are almost certain to have a multifactorial and complex genetic basis. The 3:1 predominance of autism in boys is probably not X-linked but might be accounted for by a male-specific excess of linkage peaks at the chromosomal locus 17q11.79
If an older sibling has autism, the risk that a subsequent full sibling will have autism is 2% to 8%. The concordance for autism in monozygotic twins is 60% for autistic disorder and 92% for the spectrum of pervasive developmental disorder. For dizygotic twins, the concordance for either diagnosis is up to 10%.7 Studies of individuals with autism suggest that chromosome 15q11-q13 is a candidate region for genetic risk factors.80 There is also an increased frequency of the chromosome 4B null allele and of variant serotonin transporter gene alleles at chromosomal locus 17q11-q12.77 Studies of multiplex families (those with more than one case of autism) also suggest linkage at chromosomal loci 7q31-q33, 2q31-q33, and 3p25-p26 sites.77,81 These family studies point to the possible involvement of multiple genetic risk factors.
Attention Deficit/Hyperactivity Disorder
Neurocognitive Theories
DSM-IV-TR criteria preclude a comorbid diagnosis of ADHD and autism.1 However, this is at odds with the frontostriatal model of developmental dysfunction proposed by Bradshaw,38 which links these disorders by virtue of shared neural circuitry. The frontostriatal model of developmental dysfunction also predicts that the two disorders are likely to share “common heritability factors” (p. 262).38 In addition, both disorders share a number of neurotransmitter abnormalities, including of dopamine, noradrenaline, acetylcholine, γ-amino butyric acid, and serotonin.38 The likelihood of comorbidity between these two conditions is confirmed by study findings that indicate that at least 13% of children with autism also meet criteria for ADHD.27
In contrast to autism, the executive frontostriatal profile of ADHD is characterized by inhibitory deficits82 and problems with sustained attention.83,84 The classic neuropsychological paradigms used to measure these inhibitory deficits include the Stop Signal Task and the Stroop Color-Word Task. Children with ADHD are generally slower to inhibit their responses on the Stop Signal Task and exhibit more false alarms; these abnormalities have been associated with decreased orbitofrontal and anterior cingulate cortex activation.85 On the Stroop task, children with ADHD are typically slower at calling out the color in which the incongruent words are printed, because of problems with inhibiting the more automatic word-reading response. Deficiencies of sustained attention in children with ADHD have been demonstrated on the Continuous Performance Task, a measure of sustained attention that requires participants to identify a target stimuli interspersed within a series of irrelevant distractor stimuli,83 and on the Test of Everyday Attention, a standardized test that analyzes component attentional deficits.86 Whereas planning and cognitive flexibility deficits are prominent in the cognitive profiles of children with autism, these areas of cognition are relatively intact in children with ADHD.48
Brain lateralization is potentially another point of neurocognitive difference between children with ADHD and those with autism. Whereas children with autism have been shown to display deficiencies in right hemispace performance on executive function tasks, implicating left hemisphere dysfunction,65 there is evidence that the performance of nonmedicated children with ADHD on a line-bisection task is consistent with right hemisphere dysfunction.87
Neuroanatomical and Neuroimaging Studies
As is the case with autism, no consistent structural abnormalities have been recorded for individuals affected by ADHD. Whereas autism has been associated with larger whole-brain volumes and left hemisphere anomalies, ADHD has been associated in some but not all studies with smaller whole-brain volumes,88 and right, rather than left, prefrontal anomalies.87 As with autism, structural anomalies have been reported in the basal ganglia, cerebellum, and corpus callosum.88,89
Neural regions that subserve key attentional and inhibitory functions—for example, the dorsolateral prefrontal, lateral temporal, and posterior parietal regions—have been shown to be dysfunctional in fMRI studies of individuals with ADHD.90 Children with ADHD also show decreased left caudate activation when engaged in a response inhibition task, which is potentially linked to the core symptoms of hyperactivity, disinhibition, and inattention.91
A separate fMRI study in which the same mental rotation task was used for a group of normally intelligent adolescents with ADHD (mean age 14.6 years)92 and a group with autism (mean age 14.7 years)75 revealed similar patterns of reduced prefrontal activation for both disorders, which is consistent with the frontostriatal model of neurodevelopmental disorders.38 Therefore, inherited or environmentally determined developmental dysfunction of frontostriatal circuits may manifest predominantly as autism or as ADHD, depending on the particular regions that are defective.
Genetic Theories
Evidence from twin studies and molecular genetic studies points to an inherited basis for ADHD in approximately 80% of cases, with perinatal brain injury responsible for the remainder.93 The cause in the inherited cases is likely to be a complex interaction of multiple genes; in some individuals, there is also an interaction with perinatal brain injury or other environmental traumas such as fetal alcohol exposure or postnatal malnutrition.
The most consistent findings implicate dopamine D4 and D5 receptors and the dopamine transporter and the serotonin transporter genes as candidate risk factor genes in ADHD.94,95 Genetic screening for ADHD is not yet possible, and recognition of the complex gene-environment interaction associated with each individual with ADHD is central to clinical management.95
TREATMENT
Autism
There is a wide range of approaches to the treatment and management of autism but relatively little empirical evidence to support claims of effectiveness. In view of the devastating and persistent nature of the disorder, parents understandably try interventions that promise cure, regardless of a lack of scientific evidence.96 The U.S. National Academy of Sciences concluded that there is no single intervention or treatment that is effective for all individuals with autism.97 The best outcomes are produced by a combination of educational, behavioral, communication, and social skills training approaches, together with medication if indicated, designed to target the specific needs of each child and also to provide education, support, and skills training for the parents.
Behavioral Management
Difficult behaviors such as self-injury can be eliminated, and competent behaviors such as remaining seated with other children can be taught, after an identification of the antecedents and consequences of the target behaviors. New skills can be taught with the use of positive reinforcement, physical and verbal prompts, and incrementally shaping behavior, by breaking a desired outcome into small steps (chaining). An analysis of the communicative function of a negative behavior may facilitate the development of more positive behaviors that achieve the same communicative outcome. Time out, the withdrawal of attention, and the use of a loss of favorite activities or privileges may help immediately to decrease undesirable behaviors but should be used in conjunction with approaches that then teach appropriate behaviors. Aversive, cruel, and abusive responses to negative behaviors create further adverse consequences and are unethical. There is some evidence that the application of an intensive 40-hour-per-week behavioral program (applied behavior analysis) might be associated with significant and sustained improvement, particularly in cognitive skills.98 Some parents may report satisfaction with applied behavior analysis programs, but the costs of therapy can be prohibitive, and replication of the initial study in a randomized controlled trial with comprehensive outcome measures is required.
Communication Skills
Improving the capacity of a child with autism to more effectively communicate reduces inappropriate behavior and distress. The augmentation of spoken communication with visual and nonverbal communication, such as the use of pictures and line drawings, helps improve communication skills. Social skills may also be improved through the use of cartoons or social stories that teach appropriate social behavior, such as catching a bus to school.99
Parent Training
Effective management involves collaboration between parents, teachers, and clinicians. The involvement of parents of preschool children with autism in a structured education and skills training program is associated with reduced parental stress and a sustained improvement in parental mental health, and it also facilitates developmental progress and behavioral improvement in the child.100
Pharmacotherapy
Evidence for the effectiveness of medication in the treatment of disturbed emotions and behaviors in individuals with autism is derived mostly from studies of adults with intellectual disability. Drugs should be prescribed only after an assessment has defined the specific symptoms or disorder, such as depression, that is the focus of treatment. Before the implementation of medication, it is necessary to record a baseline measure of target symptoms—for example, with a behavior checklist—in order to follow response to treatment and monitor side effects.20 Compliance is improved when the parents and individual with autism are involved in regular review.
There is some evidence that neuroleptic medication (e.g., haloperidol, risperidone) reduces aggressive, disruptive, and stereotypical behaviors and anxiety.101 However, it may produce side effects, including sedation, dystonic reactions, and increased weight gain. Tricyclic antidepressants (e.g., imipramine, clomipramine) are effective anxiolytics and may also reduce repetitive behaviors.102 Caution should be exercised, because of the potential cardiotoxic effects of tricyclic antidepressants. Case reports indicate that the selective serotonin-reuptake inhibitors such as fluoxetine may reduce anxiety and associated obsessive-compulsive behaviors, although the side effects (excitation, nausea, and headache) can be troublesome. Lithium and other mood stabilizers may reduce episodes of disruptive, aggressive, and self-injurious behavior, particularly if there is a family history of bipolar disorder. Other drugs such as stimulant medication, clonidine, and naltrexone are used to treat disruptive behaviors and symptoms of attention deficit and hyperactivity, but evidence of their efficacy is lacking.
Attention Deficit/Hyperactivity Disorder
A multimodal approach to management, including medication, special education, behavior modification, and parent education and skills training, is likely to lead to the greatest treatment response.103 Medication is the most important aspect of treatment, but multimodal treatments that account for the complex learning, behavioral, and social problems of the child improve outcomes.104 An elimination diet is effective for children in whom the specific provocative food, such as those containing tartrazine, can be identified, but it is of benefit to fewer children than is medication.105
Stimulants (methylphenidate and dexamphetamine) are the most frequently used medications. They are indirect catecholamine agonists, which facilitate the action of dopamine and noradrenaline agonists by inhibiting reuptake and facilitating release, as well as antagonizing α2-adrenergic receptors.106 There have been many randomized placebo-controlled trials of the efficacy of stimulant medication. These have clearly demonstrated immediate improvement in inattention, impulsivity, and hyperactivity and a reduction in aggression.104,105 The longer term effects on learning and academic achievement are less clear, and there is a lack of good long-term evidence for the effectiveness of stimulant medication.105
Anorexia, insomnia, irritability, and emotional distress are significant side effects that may necessitate cessation of treatment. The use of long-acting preparations may reduce some side effects and improve compliance. There is some evidence that prolonged treatment does not increase the risk of subsequent drug abuse.103,107 Stimulant medication is less effective in preschool children and young people with intellectual disability, including those with autism, and these groups are more likely to suffer adverse side effects.108 The presence of comorbid anxiety disorder also militates against the effectiveness of stimulant medication.
Children who have side effects, or who are unresponsive to stimulant medication, may benefit from treatment with tricyclic antidepressants (imipramine) or perhaps clonidine. These agents reduce hyperactivity and improve behavior but are less effective for inattention and learning. In view of the potential cardiotoxic effects of tricyclic antidepressants, review of the cardiovascular system is indicated.105 The combination of stimulant medication and nighttime clonidine is used to overcome insomnia, and neuroleptic medication may be added to control aggressive behavior, but there are no long-term studies regarding the safety or efficacy of combination treatments.
Atomoxetine, an inhibitor of the presynaptic norepinephrine transporter, has been shown in several randomized controlled trials to be at least as effective as methylphenidate in the treatment of inattention, impulsiveness, and hyperactivity.109,110 Reported side effects include decreased appetite, somnolence, fatigue, irritability, and some increase in pulse rate and blood pressure. A single morning dose produces a therapeutic effect throughout the day, and insomnia is not a side effect.
CONCLUSIONS AND RECOMMENDATIONS
Both pervasive developmental disorders and ADHD are serious neurodevelopmental conditions that cause profound distress, impairment, and disability for the individual child, stress and burden for the parents and family, and long-term cumulative costs for the community. Diagnosis depends on the careful and systematic gathering of a developmental history and on observation of behavior in a variety of settings, supplemented by a comprehensive cognitive assessment. The management of autism relies on a multimodal program of structured and targeted behavioral and educational interventions supplemented, when indicated, by pharmacotherapy. Effective medications are available for the treatment of ADHD but should be prescribed in the setting of a comprehensive educational and behavioral management program. The active involvement of parents as partners in management, together with the provision of education and skills training, further helps to consolidate treatment response, relieve family stress, and improve parental mental health. Current research into the neuropsychological features of these conditions, together with advances in understanding of central nervous system abnormalities and contributory genetic factors, is likely to lead to the elucidation of more specific neurobiological markers that will aid in the specificity of the diagnosis and the elucidation of subtypes of these disorders, with implications for treatment.
Barkley RA. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, 2nd ed. New York: Guilford Press, 1998.
Bock G, Goode J. Autism: Neural Basis and Treatment Possibilities. Novartis Foundation Symposium, No. 251. London: Wiley, 2003.
Bradshaw JL. Developmental Disorders of the Frontostriatal System: Neuropsychological, Neuropsychiatric and Evolutionary Perspectives. Hove, UK: Psychological Press, 2001.
Brereton AV, Tonge BJ. Preschoolers with Autism: An Education and Skills Training Program for Parents. London: Jessica Kingsley, 2005.
Cohen DJ, Volkmar FR, editors. Handbook of Autism and Pervasive Developmental Disorders, 2nd ed., New York: John Wiley, 1997.
1 American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association, 2000.
2 World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision. Geneva: World Health Organization, 1992.
3 Tonge BJ. Autism: time for a national approach to early assessment and management [Editorial]. Med J Aust. 1996;165:244-245.
4 Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2:217-250.
5 Asperger H. Die “autistichen psychopathen” in kindersalter. Arch Psychiatrie Nervenkrankheiten. 1944;117:76-136.
6 Sandberg S, Barton J. Historical development. In: Sandberg S, editor. Hyperactivity Disorders of Childhood. Cambridge, UK: Cambridge University Press; 1996:1-25.
7 Barkley RA. Behavioural inhibition, sustained attention, and executive functions: constructing a unified theory of ADHD. Psychol Bull. 1997;121:65-94.
8 Bradley C. The behavior of children receiving Benzedrine. Am J Psychiatry. 1937;94:577-585.
9 Fombonne P. Epidemiological surveys of autism and other pervasive developmental disorders. J Autism Dev Disord. 2003;33:365-382.
10 Magnusson P, Saemundsen E. Prevalence of autism in Iceland. J Autism Dev Disord. 2001;31:153-163.
11 Fombonne P, Du Mazaubrunc C, Cans C, et al. Autism and associated medical disorders in a French epidemiological survey. J Am Acad Child Adolesc Psychiatry. 1997;36:1561-1569.
12 Wolraich ML, Hannah JN, Baumgaertel A, et al. Examination of DSM-IV criteria for attention deficit/hyperactivity disorder in a country wide sample. J Dev Behav Pediatr. 1998;19:162-168.
13 Swanson JM, Sargeant JA, Taylor E, et al. Attention-deficit hyperactivity disorder and hyperkinetic disorder. Lancet. 1998;351:429-433.
14 Bird HR, Gould MS, Staghezza BM. Patterns of diagnostic comorbidity in a community sample of children aged 9 through 16 years. J Am Acad Child Adolesc Psychiatry. 1993;32:361-368.
15 Faraone SV, Biederman J, Weber W, et al. Psychiatric, neuropsychological and psychosocial features of DSM IV subtypes of attention-deficit/hyperactivity disorder: results from a clinically referred sample. J Am Acad Child Adolesc Psychiatry. 1998;37:185-193.
16 Szatmari P, Offord DR, Boyle MH. Correlates, associated impairments and patterns of service utilization of children with attention deficit disorder: findings from the Ontario Child Health Study. J Child Psychol Psychiatry Allied Disciplines. 1989;30:205-217.
17 Mannuzza S, Klein RG, Bessler A, et al. Adult psychiatric status of hyperactive boys grown up. Am J Psychiatry. 1998;155:493-498.
18 McCann S, Roy-Byrne P. Screening and diagnostic utility of self report attention deficit hyperactivity disorder scales in adults. Compr Psychiatry. 2004;45:175-183.
19 Filipek PA, Accardo PJ, Ashwal S, et al. Practice parameter: screening and diagnosis of autism. Neurology. 2000;55:468-479.
20 Einfeld SL, Tonge BJ. Manual for the Developmental Behaviour Checklist, Edition 2. Melbourne, Australia: Monash University Centre for Developmental Psychiatry and Psychology and School of Psychiatry, University of New South Wales, 2002.
21 Baron-Cohen S, Allen J, Gillberg C. Can autism be detected at 18 months? The needle, and the CHAT. Br J Psychiatry. 1992;161:839-934.
22 Pipek PA, Accardo PJ, Baranek GT, et al. The screening and diagnosis of autistic spectrum disorders. J Autism Dev Disord. 1999;29:437-482.
23 LeCouteur A, Rutter M, Lord C, et al. Autism Diagnostic Interview: a standardized investigator based instrument. J Autism Dev Disord. 1989;19:363-387.
24 Lord C, Rutter M, Goode S, et al. Autism Diagnostic Observation Schedule: a standardized observation of communicative and social behavior. J Autism Dev Disord. 1989;19:185-212.
25 Tonge BJ, Einfeld SL. Psychopathology and intellectual disability: the Australian Child to Adult Longitudinal Study. Int Rev Res Ment Retard. 2003;26:61-91.
26 Tonge BJ. Autism: time for a national approach to early assessment and management [Editorial]. Med J Aust. 1996;165:244-245.
27 Keen D, Ward S. Autistic spectrum disorder: a child population profile. Autism. 2004;8:39-48.
28 Tonge BJ, Brereton AV, Gray KM, et al. Behavioural and emotional disturbance in high functioning autism and Asperger disorder. Autism Int J Res Pract. 1999;2:117-130.
29 Conners CK. Rating scales in attention-deficit/hyperactivity disorder: use in assessment and treatment monitoring. J Clin Psychiatry. 1998;59:24-30.
30 Jensen PS, Martin D, Cantwell DP. Comorbidity in ADHD: implications for research, practice and DSM-V. J Am Acad Child Adolesc Psychiatry. 1997;36:1065-1079.
31 Mannuzza S, Klein RG, Bessler A, et al. Educational and occupational outcome of hyperactive boys grown up. J Am Acad Child Adolesc Psychiatry. 1997;36:1222-1227.
32 Corkum P, Tannock R, Moldofsky H. Sleep disturbances in children with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 1998;37:637-646.
33 Whalen CK, Jamner LD, Henker B, et al. The ADHD spectrum and everyday life: experience sampling of adolescent moods, activities, smoking and drinking. Child Dev. 2002;73:209-227.
34 Toone B. Attention deficit hyperactivity disorder in adulthood. J Neurol Neurosurg Psychiatry. 2004;75:523-525.
35 Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”? Cognition. 1985;21:37-46.
36 Russell J. Autism as an Executive Disorder. New York: Oxford University Press, 1997.
37 Frith U, Happe F. Autism: beyond “theory of mind.”. Cognition. 1994;50:115-132.
38 Bradshaw JL. Developmental Disorders of the Frontostriatal System: Neuropsychological, Neuropsychiatric and Evolutionary Perspectives. Hove, UK: Psychology Press, 2001.
39 Turner M. Annotation: repetitive behavior in autism: a review of psychological research. J Child Psychol Psychiatry. 1999;40:839-849.
40 Russell J, Jarrold C, Hood B. Two intact executive capacities in children with autism: implications for the core executive dysfunctions in the disorder. J Autism Dev Disord. 1999;29:103-112.
41 Happe F. Cognition in autism: one deficit or many? In Novartis Foundation Symposium: Autism: Neural Basis and Treatment Possibilities. London: Wiley, 2003;198-212.
42 Volkmar FR, Klin A, Pauls D. Nosological and genetic aspects of Asperger syndrome. J Autism Dev Disord. 1998;28:457-461.
43 Dahlgren SO, Trillingsgaard A. Theory of mind in nonretarded children with autism and Asperger’s syndrome: a research note. J Child Psychol Psychiatry Allied Disciplines. 1996;37:759-763.
44 Baron-Cohen S, O’Riordan M, Stone V, et al. Recognition of faux pas by normally developing children and children with Asperger syndrome or high-functioning autism. J Autism Dev Disord. 1999;29:407-415.
45 Baron-Cohen S, Jolliffe T, Mortimore C, et al. Another advanced test of theory of mind: evidence from very high functioning adults with autism or Asperger syndrome. J Child Psychol Psychiatry. 1997;38:813-822.
46 Rinehart NJ, Bradshaw JL, Moss SA, et al. A deficit in shifting attention present in high functioning autism but not Asperger’s disorder. Autism Int J Res Pract. 2001;5:67-80.
47 Rinehart NJ, Bradshaw JL, Moss SA, et al. Atypical interference of local detail on global processing in high functioning autism and Asperger’s disorder. J Child Psychol Psychiatry. 2000;41:778-796.
48 Ozonoff S, Jensen J. Brief report: specific executive function profiles in three neurodevelopmental disorders. J Autism Dev Disord. 1999;29:171-177.
49 Sheppard DM, Bradshaw JL, Purcell R, et al. Tourette’s and comorbid syndromes: Obsessive compulsive and attention deficit hyperactivity disorder. A common etiology? Clin Psychol Rev. 1999;19:531-552.
50 Noterdaeme M, Amorosa H, Mildenberger K, et al. Evaluation of attention problems in children with autism and children with a specific language disorder. Eur Child Adolesc Psychiatry. 2001;10:58-66.
51 Turner MA. Generating novel ideas: fluency performance in high-functioning and learning disabled individuals with autism. J Child Psychol Psychiatry. 1999;40:189-201.
52 Rinehart NJ, Bradshaw JA, Moss SA, et al. Pseudo-random number generation in children with high-functioning autism and Asperger’s disorder: further evidence for a dissociation in executive functioning? Autism J Res Pract. 2006;10:70-85.
53 Mari M, Castiello U, Marks D, et al. The reach-to-grasp movement in children with autism spectrum disorder. Philos Trans R Soc Lond B Biol Sci. 2003;358:393-403.
54 Minshew NJ, Sung K, Jones BL, et al. Underdevelopment of the postural control system in autism. Neurology. 2004;63:2056-2061.
55 Maurer RG, Damasio AG. Childhood autism from the point of view of behavioral neurology. J Autism Dev Disord. 1982;12:195-205.
56 Damasio AR, Maurer RG. A neurological model for childhood autism. Arch Neurol. 1978;35:777-786.
57 Vilensky JA, Damasio AR, Maurer RG. Gait disturbances in patients with autistic behavior. Arch Neurol. 1981;38:646-649.
58 Rinehart NJ, Tonge BJ, Bradshaw JL, et al: An examination of movement kinematics in young people with high-functioning autism and Asperger’s disorder: further evidence for a motor planning deficit. J Autism Dev Disord. In press.
59 Rinehart NJ, Tonge BJ, Bradshaw JL, et al. Movement-related-potentials in autism and Asperger’s disorder. Dev Med Child Neurol. 2006;48:272-277.
60 Rinehart NJ, Tonge BJ, Bradshaw JL, et al: Kinematic gait function in children with high functioning autism and Asperger’s disorder. Eur Child Adolescent Psychiatry (In Press).
61 Hallet M, Lebiedowska MK, Thomas SL, et al. Locomotion of autistic adults. Arch Neurol. 1993;50:1304-1308.
62 Rinehart NJ, Tonge BJ, Bradshaw JL, et al: Kinematic gait function in newly diagnosed children with autism (3–5 years). Dev Med Child Neurol (In Press)
63 Rinehart NJ, Bradshaw JL, Brereton AV, et al. A clinical and neurobehavioural review of high-functioning autism and Asperger’s disorder. Aust N Z J Psychiatry. 2002;36:762-770.
64 Rinehart NJ, Bradshaw JL, Tonge BJ, et al. A neurobehavioural examination of individuals with high-functioning autism and Asperger’s disorder using a frontostriatal model of dysfunction. Behav Cogn Neurosci Rev. 2002;1(2):164-177.
65 Rinehart NJ, Bradshaw JL, Brereton AV, et al. Lateralization in individuals with high-functioning autism and Asperger’s disorder: a frontostriatal model. J Autism Dev Disord. 2002;32:321-332.
66 Abell F, Krams M, Ashburner J, et al. The neuroanatomy of autism: a voxel-based whole brain analysis of structural scans. Neuroreport. 1999;10:1647-1651.
67 Carper RA, Moses P, Tigue ZD, et al. Cerebral lobes in autism: early hyperplasia and abnormal age effects. Neuroimage. 2002;16:1038-1051.
68 Giedd JN, Castellanos FX. Developmental disorders. In: Krishnan KRR, Doraiswamy PM, editors. Brain Imaging in Clinical Psychiatry. New York: Marcel Dekker; 1997:121-137.
69 Murphy DG, Critchley HD, Schmitz N, et al. Asperger syndrome: a proton magnetic resonance spectroscopy study of brain. Arch Gen Psychiatry. 2002;59:885-891.
70 Muller RA, Pierce K, Ambrose JB, et al. Atypical patterns of cerebral motor activation in autism: a functional magnetic resonance study. Biol Psychiatry. 2001;49:665-676.
71 Sokol DK. Neuroimaging in autistic spectrum disorder (ASD). J Neuroimaging. 2004;14:8-15.
72 Haznedar MM, Buchsbaum MS, Wei TC, et al. Limbic circuitry in patients with autism spectrum disorders studied with positron emission tomography and magnetic resonance imaging. Am J Psychiatry. 2000;157:1994-2001.
73 Happe F, Ehlers S, Fletcher P, et al. “Theory of mind” in the brain. Evidence from a PET scan study of Asperger syndrome. Neuroreport. 1996;8:197-201.
74 Haznedar MM, Buchsbaum MS, Metzger M, et al. Anterior cingulate gyrus volume and glucose metabolism in autistic disorder. Am J Psychiatry. 1997;154:1047-1050.
75 Silk TJ, Rinehart NJ, Bradshaw JL, et al: Visuospatial processing and the function of prefrontal-parietal networks in autism spectrum disorder: a functional MRI study. Am J Psychiatry. (In Press).
76 Fan J, McCandliss BD, Sommer T, et al. Testing the efficiency and independence of attentional networks. J Cogn Neurosci. 2002;14:340-347.
77 Muhle R, Trentacost SV, Rapin I. The genetics of autism. Pediatrics. 2004;113:472-486.
78 Tidmarsh F, Volkmar F. Diagnosis and epidemiology of autism spectrum disorders. Can J Psychiatry. 2003;48:517-523.
79 Stone JL, Merrimon B, Cantor RM, et al. Evidence for sexspecific risk alleles in autism spectrum disorder. Am J Hum Genet. 2004;75:1117-1123.
80 McCauley JL, Olson LM, Delahanty R, et al. A linkage disequilibrium map of the 1-Mb 15g12 GABA(A) receptor subunit cluster and association to autism. Am J Med Genet B Neuropsychiatr Genet. 2004;131:51-59.
81 Rabionet R, Jaworski JM, Ashley-Kock AE, et al. Analysis of the autism chromosome 2 linkage region: GAD1 and other candidate genes. Neurosci Lett. 2004;382:209-214.
82 Barkley RA. Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bull. 1997;121:65-94.
83 Barkley RA. The executive function and self-regulation: an evolutionary neuropsychological perspective. Neuropsychol Rev. 2001;11:1-29.
84 Nichols SL, Waschbusch DA. A Review of the Validity of laboratory cognitive tasks used to assess symptoms of ADHD. Child Psychiatry Hum Dev. 2004;34:297-315.
85 Casey J, Trainor RJ, Orendi JL, et al. A developmental functional MRI study of prefrontal activation during performance of a go-no-go task. J Cogn Neurosci. 1997;9:835-847.
86 Manly T, Anderson V, Nimmo-Smith I, et al. The differential assessment of children’s attention: the Test of Everyday Attention for Children (TEA-Ch), normative sample and ADHD performance. J Child Psychol Psychiatry. 2001;42:1065-1081.
87 Sheppard DM, Bradshaw JL, Mattingley JB, et al. Effects of stimulant medication on the lateralisation of line bisection judgements of ADHD children. J Neurol Neurosurg Psychiatry. 1999;66:57-63.
88 Castellanos FX, Giedd JN, Marsh JL, et al. Quantitative brain magnetic resonance imaging in attention deficit hyperactivity disorder. Arch Gen Psychiatry. 1996;53:607-616.
89 Hill DE, Yeo RA, Campbell RA, et al. Magnetic resonance imaging correlates of attention-deficit/hyperactivity disorder in children. Neuropsychology. 2003;17:496-506.
90 Sowell ER, Thompson PM, Welcome SE, et al. Cortical abnormalities in children and adolescents with attention deficit hyperactivity disorder. Lancet. 2003;362:1699-1707.
91 Rubia K, Overmeyer S, Taylor E, et al. Hypofrontality in attention deficit hyperactivity disorder during higher-order motor control: a study with functional MRI. Am J Psychiatry. 1999;156:891-896.
92 Silk T, Vance A, Rinehart NJ, et al. Fronto-parietal activation in attention deficit hyperactivity disorder, combined type: functional magnetic resonance imaging study. Br J Psychiatry. 2005;187:282-283.
93 Voeller KKS. Attention deficit hyperactivity disorder (ADHD). J Child Neurol. 2004;19:798-814.
94 Bobb AJ, Castellanos FX, Addington AM, et al. Molecular genetic studies of ADHD: 1991 to 2004. Am J Med Genet B Neuropsychiatr Genet. 2005;132:109-125.
95 Yeh M, Morley KI, Hall WD. The policy and ethical implications of genetic research on attention deficit hyperactivity disorder. Aust N Z J Psychiatry. 2004;38(1–2):10-19.
96 Volkmar F, Lord C, Bailey A, et al. Autism and pervasive developmental disorders. J Child Psychol Psychiatry. 2004;45:135-170.
97 National Research Council. Educating Young Children with Autism. Washington, DC: National Academies Press, 2001.
98 Lovaas I, Calouri K, Jada J. The nature of behavioral treatment and research with young autistic persons. In: Gillberg C, editor. Diagnosis and Treatment of Autism. New York: Plenum Press; 1989:285-305.
99 Gray CA, Garand JD. Social stories: improving responses of students with autism with accurate social information. Focus Autistic Behav. 1993;8:1-10.
100 Brereton AV, Tonge BJ. Preschoolers with Autism: An Education and Skills Training Program for Parents. London: Jessica Kingsley, 2005.
101 Aman MG. A double-blind, placebo-controlled trial of risperidone in children with autistic disorder. N Engl J Med. 2002;347:314-321.
102 Gordon CT, State RC, Nelson JE, et al. A double blind comparison clomipramine, desipramine and placebo in the treatment of autistic disorder. Archs Gen Psychiatry. 1993;50:441-447.
103 Zametkin AJ, Ernst M. Problems in the management of attention-deficit/hyperactivity disorder. N Engl J Med. 1999;340:40-46.
104 A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA Cooperative Group. Multimodal Treatment Study of Children with ADHD. Arch Gen Psychiatry. 1999;56:1073-1086.
105 Hill P. Attention deficit hyperactivity disorder. Arch Dis Child. 1998;79:381-386.
106 Solanto MV. Neuropsychopharmacological mechanisms of stimulant drug action in attention-deficit hyperactivity disorder: a review and integration. Behav Brain Res. 1998;94:127-152.
107 Hechtman L, Weiss G. Controlled prospective 15 year follow up of hyperactives as adults: non medical drug and alcohol use and antisocial behaviour. Can J Psychiatry. 1986;31:557-567.
108 Mayes SD, Crites DL, Bixler EO, et al. Methylphenidate and ADHD: influence of age, IQ and neurodevelopmental status. Dev Med Child Neurol. 1994;36:1099-1107.
109 Kratochvil CJ, Heiligenstein MD, Dittmann R, et al. Atomoxetine and methylphenidate treatment in children with ADHD: a prospective, randomized, open-label trial. J Am Acad Child Adolesc Psychiatry. 2002;41:776-784.
110 Kelsey DK, Sumner CR, Casat CD, et al. Once-daily atomoxetine treatment for children with attention deficit/hyperactivity disorder, including an assessment in the evening and morning behavior: a double-blind placebo-controlled trial. Pediatrics. 2004;114:111-118.