[level-membership-for-dermatology-category]
Atypical nevi
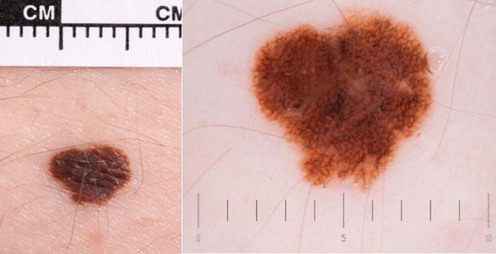
I use the term ‘atypical nevi’ to mean nevi that others might call dysplastic nevi.





Management strategy
Treatment strategies for atypical nevi:

– in the absence of worrying dermoscopic features
– reassure but give photographic information about monitoring
– if borderline consider photograph and review at 3 months
– excise if melanoma cannot be excluded after dermoscopy
– consider excision if nevus is new and/or the patient is over 50 years

– excise nevi if melanoma cannot be excluded (not usually necessary)
– assess risk based upon clinical appearance and family history
– consider genetic counseling if three or more cases of melanoma in the family, especially if those cases have multiple primaries or pancreatic cancer (www.genomel.org)
– photograph atypical nevi at high magnification and with dermoscopy
– educate the patient and partner about self-examination
– educate the family about sun protection without becoming vitamin D deficient
Specific investigations
 Dermoscopy: change in appearance
Dermoscopy: change in appearance Dermoscopy influencing decision to treat
Dermoscopy influencing decision to treat Dermoscopy in patients under follow-up for increased risk of melanoma
Dermoscopy in patients under follow-up for increased risk of melanoma Confocal microscopy: a pilot study
Confocal microscopy: a pilot study Mobile teledermatology
Mobile teledermatologyThe details of how to perform dermoscopy and the criteria for atypical nevi and melanoma are beyond the scope of this book, but there are increasing numbers of dermoscopy teaching sites on the Intranet including www.genomel.org, and an Interaction Atlas of Dermoscopy CD from Medisave.
First-line therapies
 Late diagnosis of melanomas: an assessment of the associations
Late diagnosis of melanomas: an assessment of the associations Number of melanocytic lesions excised per melanoma detected
Number of melanocytic lesions excised per melanoma detected UK melanoma treatment guidelines
UK melanoma treatment guidelines Margins of excision for atypical nevi
Margins of excision for atypical nevi[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Atypical nevi
I use the term ‘atypical nevi’ to mean nevi that others might call dysplastic nevi.
Management strategy
Treatment strategies for atypical nevi:
– in the absence of worrying dermoscopic features
– reassure but give photographic information about monitoring
– if borderline consider photograph and review at 3 months
– excise if melanoma cannot be excluded after dermoscopy
– consider excision if nevus is new and/or the patient is over 50 years
– excise nevi if melanoma cannot be excluded (not usually necessary)
– assess risk based upon clinical appearance and family history
[/not-level-membership-for-dermatology-category]
