[level-membership-for-orthopaedics-category]Chapter 2
Anatomy
section 1 Introduction
A Osteology: The human skeleton has 206 bones: axial skeleton (80) and appendicular skeleton (126)
 Intramembranous (direct laying down of bone without a cartilage model [skull]) or enchondral (with a cartilage precursor [most bones]).
Intramembranous (direct laying down of bone without a cartilage model [skull]) or enchondral (with a cartilage precursor [most bones]).
 Enchondral growth begins in the diaphyses of long bones at primary ossification centers, most of which are present at birth (Table 2-1).
Enchondral growth begins in the diaphyses of long bones at primary ossification centers, most of which are present at birth (Table 2-1).
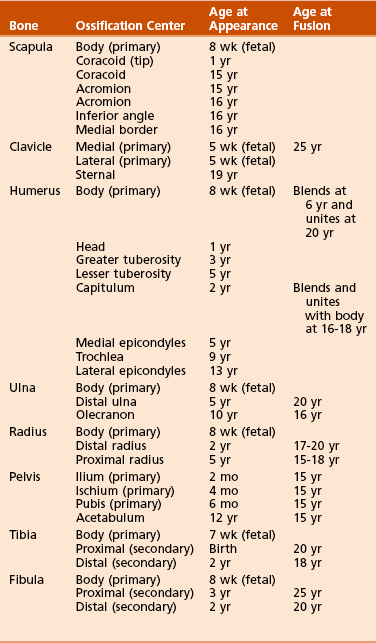
2. Secondary ossification centers usually develop in the periphery of bones and are important for growth and the treatment of childhood fractures.
3. Heterotopic ossification is the formation of bone tissue in an atypical, extraskeletal location.
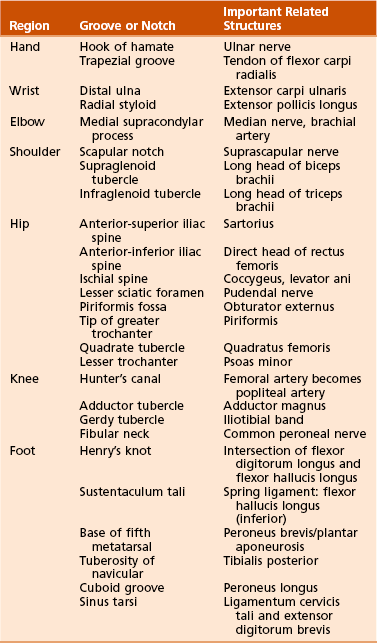
4. Anatomic landmarks of the skeleton and their related structures are listed in Table 2-2.
B Arthrology: Joints are commonly classified into three types on the basis of their freedom of movement
1. Synarthroses: joining of two bony elements with no motion during maturity; skull sutures
2. Amphiarthroses: have hyaline cartilage and intervening discs with limited motion; symphysis pubis
3. Diarthroses: characterized by hyaline cartilage, synovial membranes, capsules, and ligaments
C Myology: classification based on the arrangement of muscle fibers
2. Fusiform (e.g., biceps brachii)
3. Oblique (with tendinous interdigitation): further classified as pennate, bipennate, multipennate
 Originate from the ventral rami of spinal nerves and are distributed via several plexuses (cervical, brachial, lumbosacral)
Originate from the ventral rami of spinal nerves and are distributed via several plexuses (cervical, brachial, lumbosacral)

 Efferent (motor) fibers carry impulses from the central nervous system to muscles.
Efferent (motor) fibers carry impulses from the central nervous system to muscles.
 Afferent (sensory) fibers carry information toward the central nervous system.
Afferent (sensory) fibers carry information toward the central nervous system.








section 2 Upper Extremity
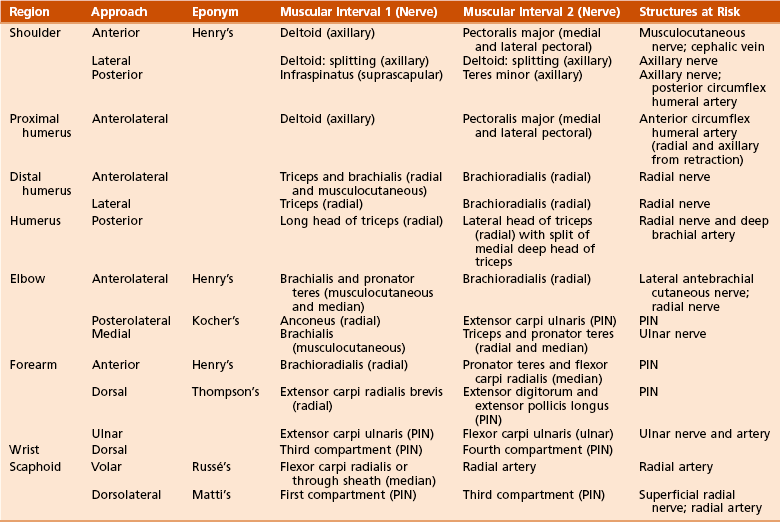
Table 2-3 summarizes upper extremity innervation. Table 2-4 summarizes standard surgical approaches to the upper extremity.
Table 2-3
Summary of Upper Extremity Innervation
| Nerves | Muscles Innervated |
| Musculocutaneous (lateral cord) | Coracobrachialis, biceps, brachialis |
| Axillary (posterior cord) | Deltoid, teres minor |
| Radial (posterior cord) | Triceps, brachioradialis, extensor carpi radialis longus and brevis |
| Posterior interosseous | Supinator, extensor carpi ulnaris, extensor digitorum, extensor digiti minimi, abductor pollicis longus, extensor pollicis longus and brevis, extensor indicis proprius |
| Median (medial and lateral cord) | Pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, abductor pollicis brevis, supinator head of flexor pollicis brevis, opponens pollicis, first and second lumbrical muscles |
| Anterior interosseous | Flexor digitorum profundus (first and second), flexor pollicis longus, pronator quadratus |
| Ulnar (medial cord) | Flexor carpi ulnaris, flexor digitorum profundus (third and fourth), palmaris brevis, abductor digiti minimi, opponens digiti minimi, flexor digiti minimi, third and fourth lumbrical muscles, interossei, adductor pollicis, deep head of flexor pollicis brevis |
 Spans the second through seventh ribs and serves as an attachment for 17 muscles and four ligaments
Spans the second through seventh ribs and serves as an attachment for 17 muscles and four ligaments
 Glenoid is retroverted approximately 5 degrees.
Glenoid is retroverted approximately 5 degrees.





 It is the fulcrum for lateral movement of the arm.
It is the fulcrum for lateral movement of the arm.

 The clavicle is the first bone in the body to ossify (at 5 weeks of gestation) and the last to fuse (medial epiphysis at 25 years of age; see Table 2-1). Fracture of the clavicle is the most common musculoskeletal birth injury.
The clavicle is the first bone in the body to ossify (at 5 weeks of gestation) and the last to fuse (medial epiphysis at 25 years of age; see Table 2-1). Fracture of the clavicle is the most common musculoskeletal birth injury.
B Arthrology: one major articulation (glenohumeral joint) and several minor articulations (sternoclavicular, acromioclavicular, scapulothoracic joints)
1. Glenohumeral joint (Figure 2-1): Spheroidal, ball and socket, with the greatest joint range of motion; motion is at the expense of stability with static and dynamic restraints.
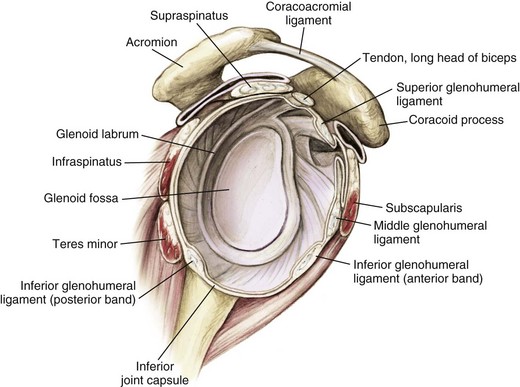
 Static restraints include the articular anatomy, glenoid labrum, negative pressure, capsule, and ligaments.
Static restraints include the articular anatomy, glenoid labrum, negative pressure, capsule, and ligaments.

 Important glenohumeral stabilizers summarized in Table 2-5
Important glenohumeral stabilizers summarized in Table 2-5
Table 2-5
| Structure | Function |
| Coracohumeral ligament | Primary restraint in inferior translation of the adducted arm and to external rotation |
| Glenoid labrum | Increases surface area, static stabilizer |
| Superior glenohumeral ligament | Primary restraint in external rotation of the adducted or slightly abducted arm Primary restraint in inferior translation of the adducted arm |
| Middle glenohumeral ligament (absent up to 30% of shoulders) | Primary stabilizer in anterior translation, with the arm abducted to 45 degrees |
| Inferior glenohumeral ligament complex | Primary stabilizer for anterior and inferior translation in abduction |
 This joint is double-gliding, with an articular disc.
This joint is double-gliding, with an articular disc.

 The sternoclavicular joint rotates 30 degrees with shoulder motion.
The sternoclavicular joint rotates 30 degrees with shoulder motion.
 Plane/gliding joint with a fibrocartilaginous disc
Plane/gliding joint with a fibrocartilaginous disc

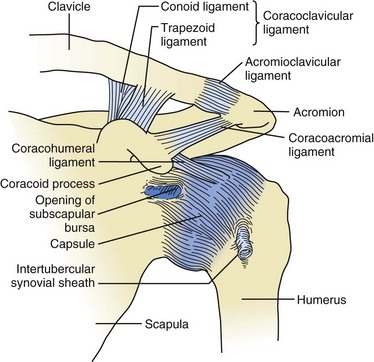
Figure 2-2 Ligaments about the shoulder. The acromioclavicular ligaments (superior, inferior, anterior, and posterior) prevent anteroposterior translation of the distal clavicle. The superior ligament is the most important and is reinforced by fibers from the trapezius and deltoid muscles. The coracoclavicular ligaments—conoid (posteromedial) and trapezoid (anterolateral)—prevent superior translation of the distal clavicle. The coracoacromial ligament should be preserved in massive rotator cuff defects because it provides superior restraint to the humeral head. Bleeding encountered during release of the coracoacromial ligament comes from the acromial branch of the thoracoacromial artery (second part of axillary artery; see Figure 2-6). (Adapted from Jenkins DB: Hollinshead’s functional anatomy of the limbs and back, ed 6, Philadelphia, 1991, Saunders, p 71.)



 Though not a true joint, this attachment allows scapular movement against the posterior rib cage.
Though not a true joint, this attachment allows scapular movement against the posterior rib cage.
 Fixed primarily by the scapular muscular attachments.
Fixed primarily by the scapular muscular attachments.
 Glenohumeral motion in comparison with scapulothoracic motion is in a 2:1 ratio.
Glenohumeral motion in comparison with scapulothoracic motion is in a 2:1 ratio.






1. Muscles connecting the upper limb to the vertebral column: trapezius, latissimus, both rhomboid muscles, and levator scapulae
2. Muscles connecting the upper limb to the thoracic wall: both pectoralis muscles, subclavius, and serratus anterior
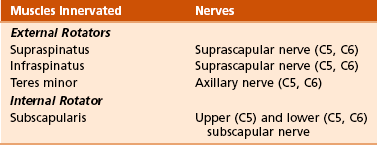
3. Muscles acting on the shoulder joint itself: deltoid, teres major, and the four rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis)
 The rotator cuff muscles depress and stabilize the humeral head against the glenoid; all attach to the greater tuberosity except the subscapularis, which has a lesser tuberosity insertion (shoulder internal rotator).
The rotator cuff muscles depress and stabilize the humeral head against the glenoid; all attach to the greater tuberosity except the subscapularis, which has a lesser tuberosity insertion (shoulder internal rotator).

 Table 2-6 presents the specific characteristics of these muscles, and Figure 2-4 and Table 2-7 describe the four layers of shoulder musculature.
Table 2-6 presents the specific characteristics of these muscles, and Figure 2-4 and Table 2-7 describe the four layers of shoulder musculature.
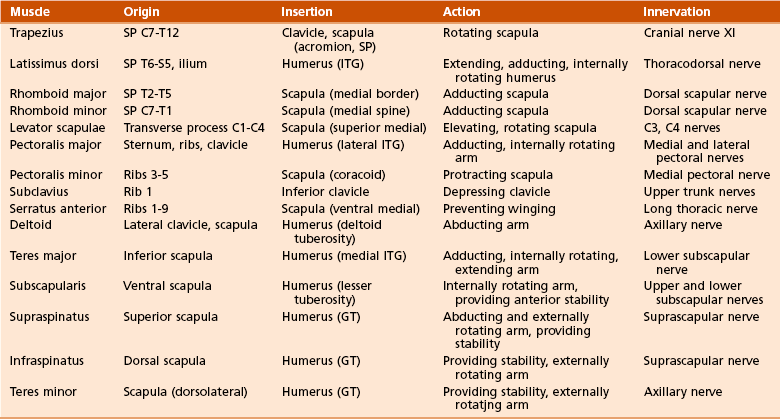
Table 2-7
Shoulder-Supporting Anatomic Layers
| Layer | Structures |
| I | Deltoid; pectoralis major; trapezius |
| II | Clavipectoral fascia; conjoined tendon, short head of biceps, and coracobrachialis |
| III | Deep layer of subdeltoid bursa; rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis [SITS]) |
| IV | Glenohumeral joint capsule; coracohumeral ligament |
1. Anatomy of brachial plexus (Figure 2-5)
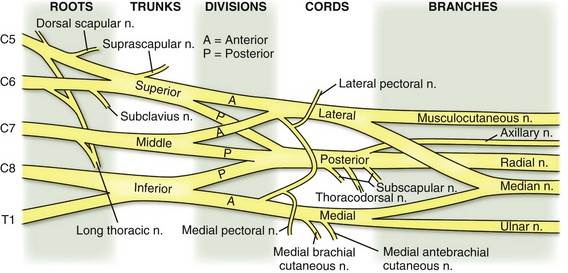

 The brachial plexus is formed from the ventral primary rami of C5 to T1 and lies under the clavicle between the scalenus anterior and scalenus medius.
The brachial plexus is formed from the ventral primary rami of C5 to T1 and lies under the clavicle between the scalenus anterior and scalenus medius.
 Dorsal rami of C5 to T1 innervate the dorsal neck musculature and skin.
Dorsal rami of C5 to T1 innervate the dorsal neck musculature and skin.

 Five roots (C5 to T1, although contributions from C4 and T2 can be small)
Five roots (C5 to T1, although contributions from C4 and T2 can be small)
 Three trunks (upper, middle, lower)
Three trunks (upper, middle, lower)
 Six divisions (two from each trunk)
Six divisions (two from each trunk)
 Three cords (named because of their anatomic relationship to the axillary artery: posterior, lateral, and medial); the termination of each cord is shown in Table 2-8
Three cords (named because of their anatomic relationship to the axillary artery: posterior, lateral, and medial); the termination of each cord is shown in Table 2-8
Table 2-8
Brachial Plexus Cord Terminations
| Cord | Termination |
| Lateral | Musculocutaneous nerve* Lateral pectoral nerve |
| Posterior | Radial and axillary nerve* Upper and lower subscapular nerve Thoracodorsal nerve |
| Medial | Ulnar nerve* Medial pectoral nerve Medial brachial cutaneous nerve Medial antebrachial cutaneous nerve |
| Medial and lateral | Median nerve* |
 Multiple branches: four preclavicular branches (from roots and upper trunk):
Multiple branches: four preclavicular branches (from roots and upper trunk):




2. Muscle innervation: innervation of all rotator cuff muscles derived from C5 and C6 of the brachial plexus (Table 2-9; see also Table 2-3)












 The left subclavian artery arises directly from the aorta, and the right subclavian artery arises from the brachiocephalic trunk.
The left subclavian artery arises directly from the aorta, and the right subclavian artery arises from the brachiocephalic trunk.




F Surgical approaches to the shoulder (Table 2-12; see Table 2-4):
Table 2-12
Surgical Approaches to the Shoulder
| Approach | Interval | Structures at Risk |
| Anterior (Henry’s) | Deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerve) | Axillary nerve limits inferior exposure; place arm in adduction and external rotation Musculocutaneous nerve: avoid vigorous retraction and medial dissection to the conjoined tendon/coracobrachialis |
| Lateral | Deltoid splitting (axillary nerve) | Avoid deltoid split >5 cm below acromion, to avoid damaging axillary nerve |
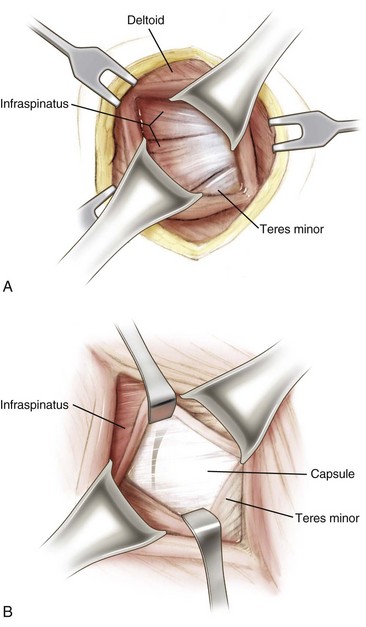
| Posterior | Infraspinatus (suprascapular nerve) and teres minor (axillary nerve) | Dissection inferior to the teres minor puts quadrangular space structures at risk: axillary nerve and posterior humeral circumflex artery Avoid excessive medial retraction on infraspinatus, which can injure suprascapular nerve |
1. Anterior (Henry’s) approach (Figure 2-7)
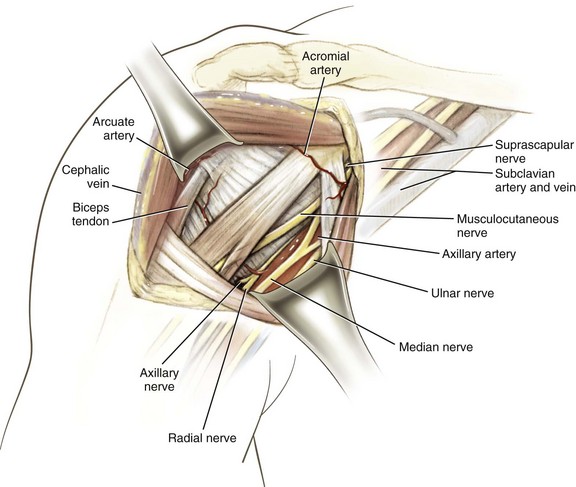
 Interval: deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves)
Interval: deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves)

 Dissect the cephalic vein, and retract it laterally with the deltoid, thereby exposing the underlying subscapularis.
Dissect the cephalic vein, and retract it laterally with the deltoid, thereby exposing the underlying subscapularis.




















G Arthroscopy (discussed in Chapter 4, Sports Medicine)
 Articulates with the smaller scapular glenoid cavity
Articulates with the smaller scapular glenoid cavity
 Retroverted 30 degrees (in relation to the transepicondylar axis of the humerus)
Retroverted 30 degrees (in relation to the transepicondylar axis of the humerus)

2. Anatomic neck, directly below the humeral head, serves as an attachment for the shoulder capsule.
3. Surgical neck is lower and is more often involved in fractures.
4. Greater tuberosity is lateral to the humeral head.
 Serves as the attachment for the supraspinatus, infraspinatus, and teres minor muscles (anterior to posterior, respectively)
Serves as the attachment for the supraspinatus, infraspinatus, and teres minor muscles (anterior to posterior, respectively)
5. Lesser tuberosity, located anteriorly, has only one muscular insertion: the last rotator cuff muscle, the subscapularis.
6. Bicipital groove (for the tendon of the long head of the biceps brachii) is a bony groove between the two tuberosities.
7. Humeral shaft has a posterior spiral groove (for the radial nerve) adjacent to the deltoid tuberosity and approximately 13 cm above the articular surface of the trochlea.
8. Distally, the humerus flares into medial and lateral epicondyles.




 Elbow is composed of a hinge joint (the humeroulnar articulation) and a pivot joint (the humeroradial articulation) (Table 2-13).
Elbow is composed of a hinge joint (the humeroulnar articulation) and a pivot joint (the humeroradial articulation) (Table 2-13).
Table 2-13
| Articulation | Components |
| Humeroulnar | Trochlea and trochlear notch |
| Humeroradial | Capitulum and radial head |
| Proximal radioulnar | Radial notch and radial head |

 Elbow joint has capsuloligamentous tissues (Figure 2-9) that are a key source of testable material.
Elbow joint has capsuloligamentous tissues (Figure 2-9) that are a key source of testable material.
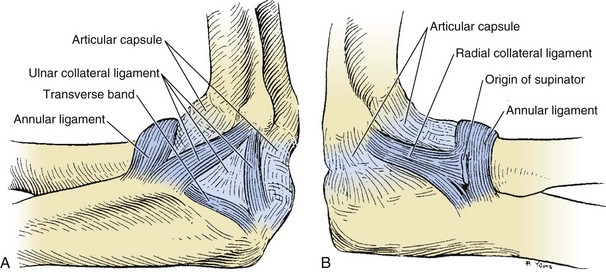



Table 2-14
| Ligament | Components | Comments |
| Medial collateral | Anterior bundle of MCL (ulnar collateral); posterior bundle; transverse bundle (Cooper ligament) | Anterior bundle (strongest of all elbow ligaments): anterior band taut from 60 degrees of flexion to full extension, posterior band taut from 60-120 degrees of flexion |
| Lateral collateral | LUCL; annular ligament; quadrate (annular ligament to radial neck) and oblique cord | Deficiency of LUCL results in posterolateral rotator instability |
LUCL, lateral ulnar collateral ligament; MCL, medial collateral ligament.
 The medial collateral ligament (MCL) (anterior, posterior, and transverse bundles) arises from the anteroinferior portion of the medial humeral epicondyle and provides stability in valgus stress.
The medial collateral ligament (MCL) (anterior, posterior, and transverse bundles) arises from the anteroinferior portion of the medial humeral epicondyle and provides stability in valgus stress.





C Muscles: four muscles of the arm controlling elbow motion (Table 2-15)

1. Flexors (biceps, brachialis, and brachioradialis); the brachialis attaches to the coronoid at 11 mm distal to the tip
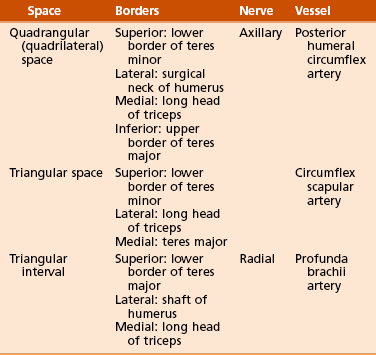
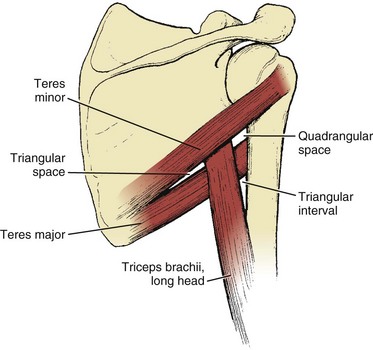
2. Extensors (triceps); also helps form borders for three important spaces (Figure 2-10 and Table 2-16)







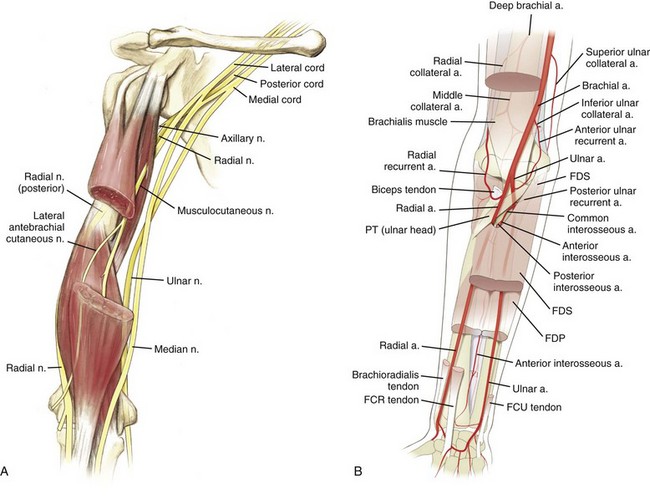
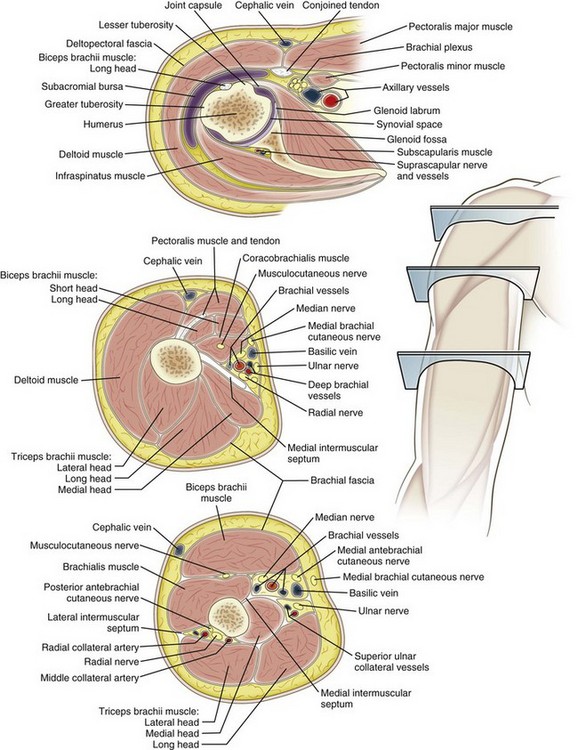
 Four major nerves traverse the arm; two give off branches to arm musculature, and two innervate the distal musculature (Figure 2-11). Most of the cutaneous innervation of the arm arises directly from the brachial plexus.
Four major nerves traverse the arm; two give off branches to arm musculature, and two innervate the distal musculature (Figure 2-11). Most of the cutaneous innervation of the arm arises directly from the brachial plexus.
 Musculocutaneous nerve (lateral cord):
Musculocutaneous nerve (lateral cord):
 Pierces the coracobrachialis 5 to 8 cm distal to the coracoid
Pierces the coracobrachialis 5 to 8 cm distal to the coracoid
 Branches to supply the coracobrachialis, the biceps, and the brachialis
Branches to supply the coracobrachialis, the biceps, and the brachialis

 Radial nerve (posterior cord):
Radial nerve (posterior cord):
 Spirals around the humerus (medial to lateral) in the spiral groove at a distance of approximately 13 cm from the trochlea
Spirals around the humerus (medial to lateral) in the spiral groove at a distance of approximately 13 cm from the trochlea

 Median nerve (medial and lateral cords):
Median nerve (medial and lateral cords):
 Accompanies the brachial artery along the arm, crossing it during its course (lateral to medial)
Accompanies the brachial artery along the arm, crossing it during its course (lateral to medial)
 Supplies some branches to the elbow joint but has no branches in the arm itself
Supplies some branches to the elbow joint but has no branches in the arm itself

 Passes medial to the brachial artery in the arm and then runs behind the medial epicondyle of the humerus, where it is superficial
Passes medial to the brachial artery in the arm and then runs behind the medial epicondyle of the humerus, where it is superficial







2. Compressive neuropathies (Table 2-17)
Table 2-17
Nerve Compression Syndromes of the Arm and Forearm
| Syndrome | Nerve Involved | Sites of Compression |
| Pronator | Median | Supracondylar process of humerus and ligament of Struthers Lacertus fibrosis (bicipital aponeurosis) Pronator teres Arch of flexor digitorum superficialis |
| AIN | AIN of median | Deep head of pronator teres Flexor digitorum superficialis Aberrant vessels Accessory muscles (i.e., Gantzer’s muscles) |
| Cubital tunnel | Ulnar | Arcade of Struthers Medial intermuscular septum Medial epicondyle Cubital tunnel Proximal edge of flexor carpi ulnaris (Osborne fascia) Deep flexor pronator aponeurosis |
| PIN Radial tunnel |
PIN of radial | Fibrous bands Recurrent leash of Henry Extensor carpi radialis brevis Arcade of Frohse (proximal edge of superficial head of supinator) Supinator distal margin |
| Superficial radial nerve | Superficial radial | Between the brachioradialis and extensor carpi radialis longus |
AIN, anterior interosseous nerve; PIN, posterior interosseous nerve.
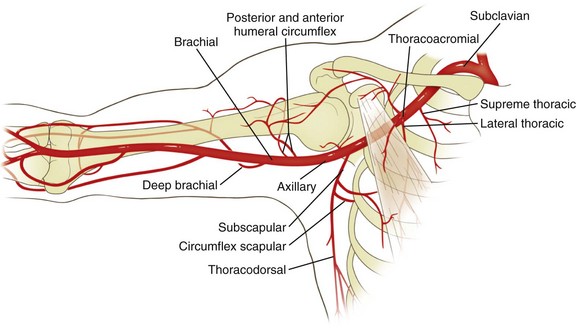
 Originates at the lower border of the tendon of the teres major and continues to the elbow, where it bifurcates into the radial and ulnar arteries (see Figure 2-11)
Originates at the lower border of the tendon of the teres major and continues to the elbow, where it bifurcates into the radial and ulnar arteries (see Figure 2-11)
 Lies medial in the arm, curving laterally to enter the cubital fossa
Lies medial in the arm, curving laterally to enter the cubital fossa

 Deep brachial (also known as the profunda, this artery accompanies the radial nerve posteriorly in the triangular interval)
Deep brachial (also known as the profunda, this artery accompanies the radial nerve posteriorly in the triangular interval)
 Superior and inferior ulnar collateral arteries
Superior and inferior ulnar collateral arteries
 The nutrient and muscular branches
The nutrient and muscular branches
 The supratrochlear artery (the least flexible branch)
The supratrochlear artery (the least flexible branch)
 These collateral vessels can bind up the brachial artery with distal humerus fractures
These collateral vessels can bind up the brachial artery with distal humerus fractures
F Surgical approaches to the humerus. (Table 2-18)
Table 2-18
Surgical Approaches to the Humerus
| Approach | Interval | Structures at Risk |
| Anterolateral—proximal | Proximal—deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerve) Distal—brachialis (radial and musculocutaneous nerve) |
Radial nerve; axillary nerve; anterior humeral circumflex artery |
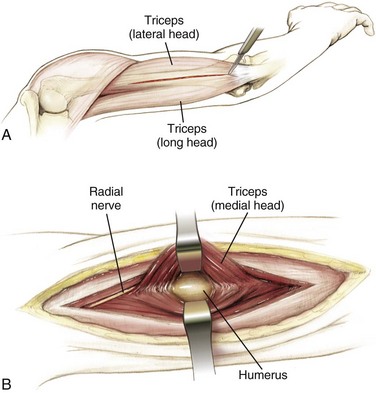
| Posterior | Triceps (radial nerve); lateral and long heads | Radial nerve; deep brachial artery |
| Anterolateral—distal | Brachialis (musculocutaneous and radial nerve) and brachioradialis (radial nerve) | Radial nerve |
| Lateral | Triceps (radial nerve) and brachioradialis (radial nerve) | Radial nerve with proximal extension |
1. Anterolateral approach to the humerus (Figure 2-13)
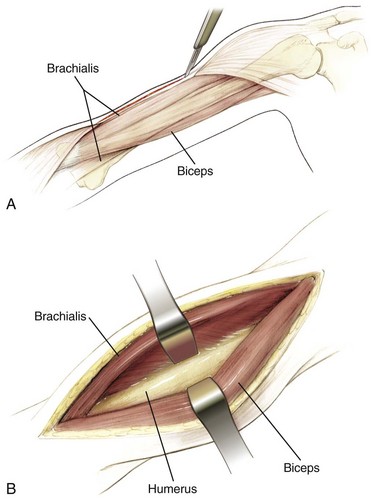
 Interval: deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves) proximally and between the fibers of the brachialis (radial and musculocutaneous nerves) distally
Interval: deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves) proximally and between the fibers of the brachialis (radial and musculocutaneous nerves) distally



 Risks: The radial and axillary nerves are at risk for injury mainly because of forceful retraction.
Risks: The radial and axillary nerves are at risk for injury mainly because of forceful retraction.








G Surgical approaches to the elbow (Table 2-19)
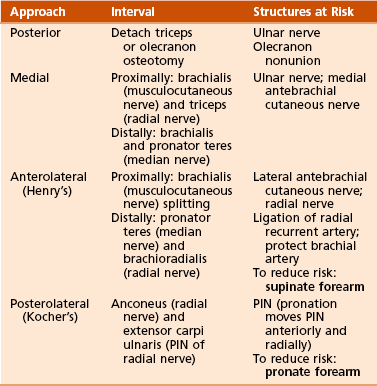
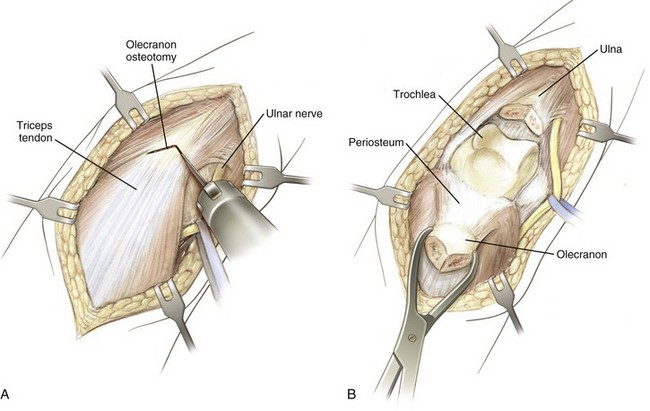
1. Posterior approach to the elbow (Figure 2-15)








2. Medial approach to the elbow (Figure 2-16)
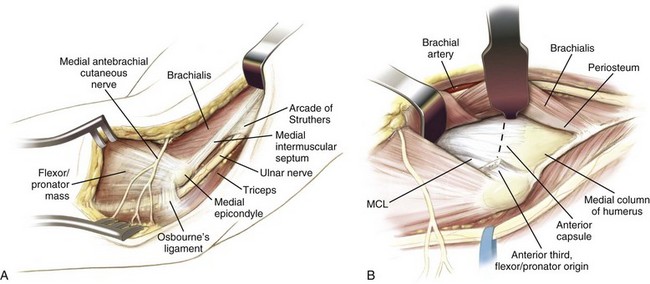
 Interval: between the brachialis (musculocutaneous nerve) and the triceps (radial nerve) proximally and between the brachialis and pronator teres (median nerve) distally.
Interval: between the brachialis (musculocutaneous nerve) and the triceps (radial nerve) proximally and between the brachialis and pronator teres (median nerve) distally.

 Risks: The ulnar and medial antebrachial cutaneous nerves are in the field and must be protected.
Risks: The ulnar and medial antebrachial cutaneous nerves are in the field and must be protected.
3. Lateral or posterolateral (Kocher’s) approach to the elbow (Figure 2-17)
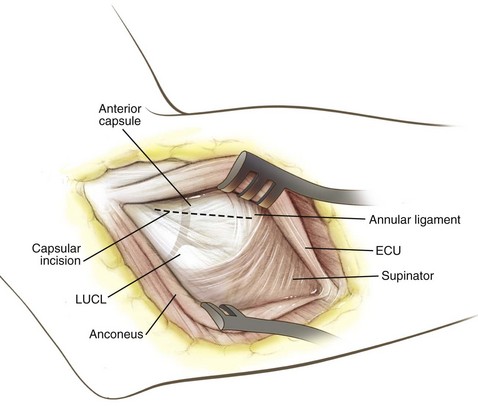
 Interval: between the anconeus (radial nerve) and the origin of the main extensor (extensor carpi ulnaris, posterior interosseous nerve [PIN])
Interval: between the anconeus (radial nerve) and the origin of the main extensor (extensor carpi ulnaris, posterior interosseous nerve [PIN])


4. Proximal extension of lateral approach
 Interval: along lateral intercondylar ridge, between triceps and extensor carpi radialis longus (ECRL) (brachioradialis nerve)
Interval: along lateral intercondylar ridge, between triceps and extensor carpi radialis longus (ECRL) (brachioradialis nerve)
 Dissection: Subperiosteally expose the anterior humerus and lateral column.
Dissection: Subperiosteally expose the anterior humerus and lateral column.
 Risks: retractor placed under brachialis anteriorly to protect radial nerve, distally limited by PIN
Risks: retractor placed under brachialis anteriorly to protect radial nerve, distally limited by PIN
A Osteology: includes the ulna and radius, which articulate with the humerus (principally the ulna) and carpi (principally the radius)
 Proximally, the ulna is composed of two curved processes, the olecranon and the coronoid processes, with an intervening trochlear notch.
Proximally, the ulna is composed of two curved processes, the olecranon and the coronoid processes, with an intervening trochlear notch.
 Distally, the ulna tapers and ends in a lateral head and a medial styloid process.
Distally, the ulna tapers and ends in a lateral head and a medial styloid process.



B Arthrology: proximally includes the elbow joint (discussed earlier) and distally includes the wrist
1. Distal radioulnar articulation (most stable in supination)
 This joint is ellipsoid and involves the distal radius and the scaphoid, lunate, and triquetrum.
This joint is ellipsoid and involves the distal radius and the scaphoid, lunate, and triquetrum.
 It is usually located at the level of the crease of the proximal wrist flexion.
It is usually located at the level of the crease of the proximal wrist flexion.


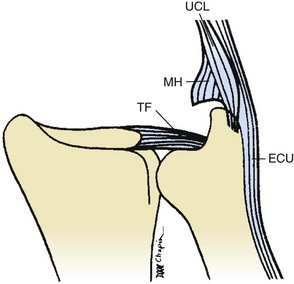
3. Triangular fibrocartilage complex (Figure 2-19): originates from the most ulnar portion of the radius and extends into the caput ulnae and the wrist aspect of the ulna to the base of the fifth metacarpal; includes the components listed in Table 2-20
Table 2-20
Components of the Triangular Fibrocartilage Complex
| Component | Origin | Insertion |
| Dorsal and volar radioulnar ligament | Ulnar radius | Caput ulnae |
| Articular disc | Radius/ulna | Triquetrum |
| Prestyloid recess | Disc | Meniscus homolog |
| Meniscus homolog | Ulna/disc | Triquetrum/ulnar collateral ligament |
| Ulnar collateral ligament | Ulna | Fifth metacarpal |
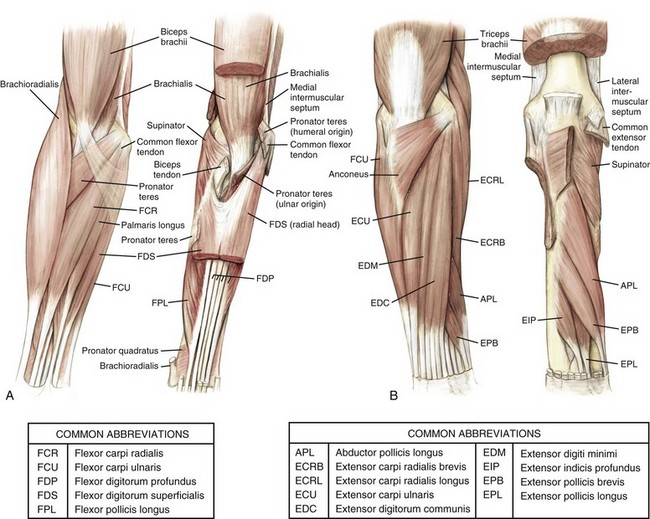
C Muscles (Figure 2-20 and Table 2-21): arranged according to both location and function
Table 2-21
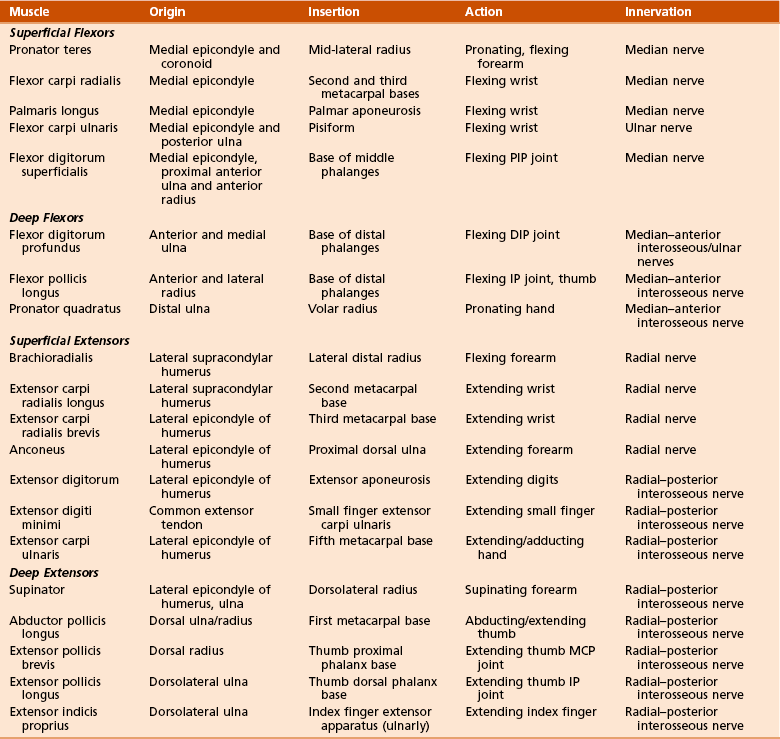
1. Volar flexors (superficial and deep)
2. Dorsal extensors (superficial and deep): tennis elbow (lateral epicondylitis) involves primarily the extensor carpi radialis brevis (ECRB)
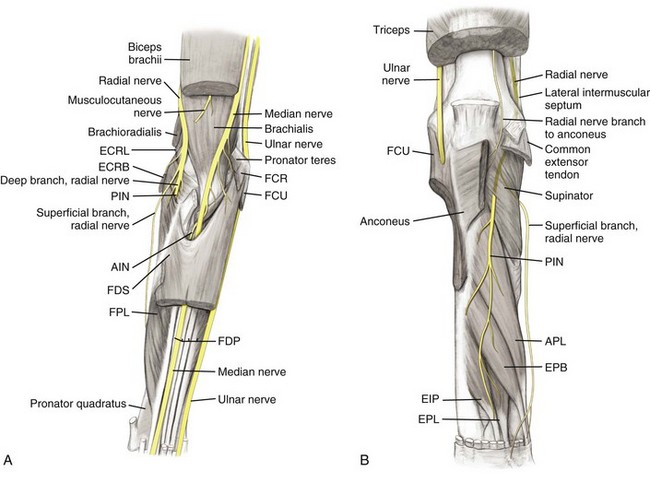
1. Anatomy: nerves of upper arm continue into the forearm (Figure 2-21, Table 2-22)
Table 2-22
Neuroanatomic Relationships in the Forearm
| Nerve | Relationships |
| Radial | Between brachialis and brachioradialis |
| Posterior interosseous | Splits supinator |
| Superficial radial | Between brachioradialis and extensor carpi radialis longus |
| Median | Medial to brachial artery at elbow |
| Anterior interosseous | Splits pronator teres and runs between flexor digitorum superficialis and flexor digitorum profundus Between flexor pollicis longus and flexor digitorum profundus |
| Ulnar | Between flexor carpi ulnaris and flexor digitorum profundus |







 This nerve is medial to the brachial artery at the elbow and superficial to the brachialis muscle.
This nerve is medial to the brachial artery at the elbow and superficial to the brachialis muscle.

 It becomes more superficial at the flexor retinaculum, where it continues into the hand.
It becomes more superficial at the flexor retinaculum, where it continues into the hand.



 Enters the forearm between the two heads of the FCU, which it supplies
Enters the forearm between the two heads of the FCU, which it supplies
 Runs between the FCU and FDP, innervating the ulnar half of this muscle
Runs between the FCU and FDP, innervating the ulnar half of this muscle
 Lies more superficial at the wrist and enters the hand through the Guyon canal
Lies more superficial at the wrist and enters the hand through the Guyon canal
 Cutaneous nerves (see Figure 2-12)
Cutaneous nerves (see Figure 2-12)
 Lateral antebrachial cutaneous nerve: the continuation of the musculocutaneous nerve that passes lateral to the cephalic vein after emerging laterally from between the biceps and brachialis at the elbow
Lateral antebrachial cutaneous nerve: the continuation of the musculocutaneous nerve that passes lateral to the cephalic vein after emerging laterally from between the biceps and brachialis at the elbow
 Medial antebrachial cutaneous nerve: a branch from the medial cord of the brachial plexus
Medial antebrachial cutaneous nerve: a branch from the medial cord of the brachial plexus
 Posterior antebrachial cutaneous nerve:a branch of the radial nerve given off in the arm
Posterior antebrachial cutaneous nerve:a branch of the radial nerve given off in the arm





 Enters cubital fossa (bordered by the two epicondyles, the brachioradialis, and the pronator teres and overlying the brachialis and supinator)
Enters cubital fossa (bordered by the two epicondyles, the brachioradialis, and the pronator teres and overlying the brachialis and supinator)
 Then divides at the level of the radial neck into the radial and ulnar arteries (Table 2-24)
Then divides at the level of the radial neck into the radial and ulnar arteries (Table 2-24)
Table 2-24
Vascular Anatomic Relationships in the Forearm
| Artery | Relationships |
| Radial | On pronator teres deep to brachioradialis Enters wrist between brachioradialis and flexor carpi radialis |
| Ulnar | Proximally between FDS and FDP Distally on FDP between flexor carpi ulnaris and FDS |
FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis.
 This artery initially runs on the pronator teres, deep to the brachioradialis.
This artery initially runs on the pronator teres, deep to the brachioradialis.
 It continues to the wrist between this muscle and the flexor carpi radialis (FCR).
It continues to the wrist between this muscle and the flexor carpi radialis (FCR).
 Forearm branches include the recurrent radial (see earlier discussion) and muscular branches.
Forearm branches include the recurrent radial (see earlier discussion) and muscular branches.



F Surgical approaches to the forearm (Table 2-25)
Table 2-25
Surgical Approaches to the Forearm
| Approach | Interval | Structures at Risk |
| Anterior (Henry’s) | Brachioradialis (radial nerve) and pronator teres (median nerve) Distally: flexor carpi radialis (median nerve) |
Ligate leash of Henry (radial artery branches) Superficial branch of radial nerve |
| Dorsal posterior (Thompson’s) | Extensor carpi radialis brevis (radial nerve) and extensor digitorum communis (PIN) Distally: extensor pollicis longus |
PIN: avoid excessive retraction of supinator |
| Ulnar | Extensor carpi ulnaris (PIN) and flexor carpi ulnaris (ulnar nerve) |
1. Anterior (Henry’s) approach (Figure 2-22)
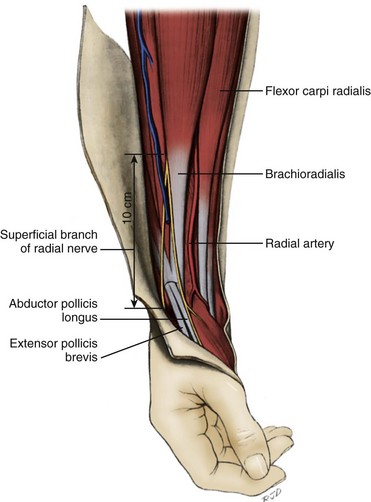
 Interval: between the brachioradialis (radial nerve) and pronator teres or FCR distally (median nerve)
Interval: between the brachioradialis (radial nerve) and pronator teres or FCR distally (median nerve)

 Proximally: Isolate and ligate the leash of Henry (radial artery branches) proximally, and strip the supinator from its insertion subperiosteally; supination of the forearm displaces the PIN ulnarly.
Proximally: Isolate and ligate the leash of Henry (radial artery branches) proximally, and strip the supinator from its insertion subperiosteally; supination of the forearm displaces the PIN ulnarly.
 Middle third: Pronate the forearm and incise the insertion of the pronator teres subperiosteally.
Middle third: Pronate the forearm and incise the insertion of the pronator teres subperiosteally.





2. Dorsal (posterior; Thompson’s) approach (Figure 2-23)
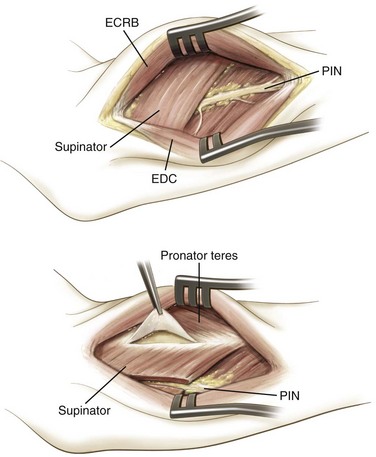
 Interval: between the ECRB (radial nerve) and extensor digitorum or EPL distally (PIN)
Interval: between the ECRB (radial nerve) and extensor digitorum or EPL distally (PIN)







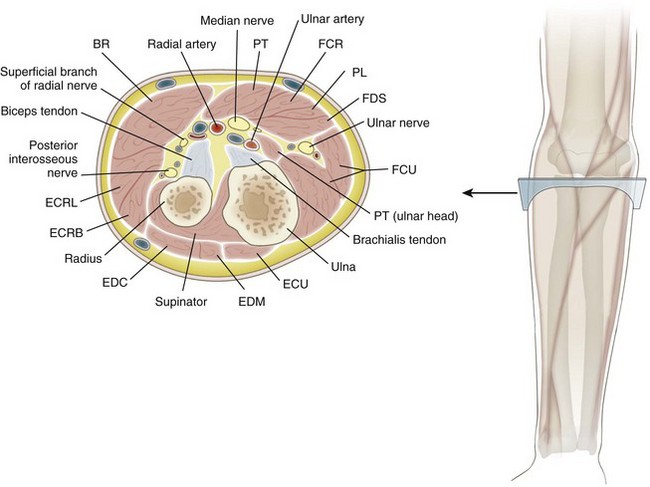
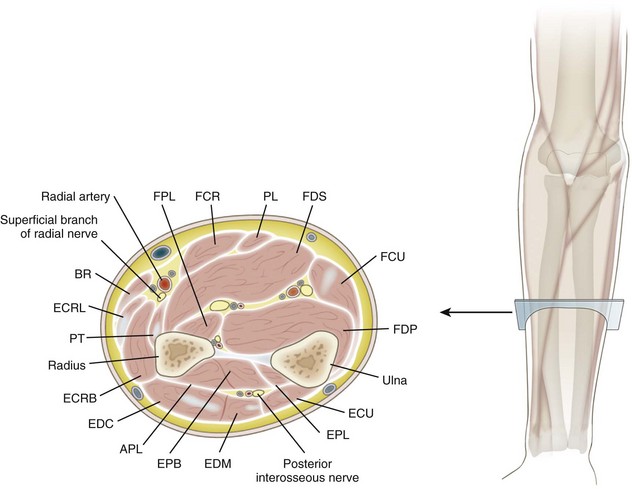
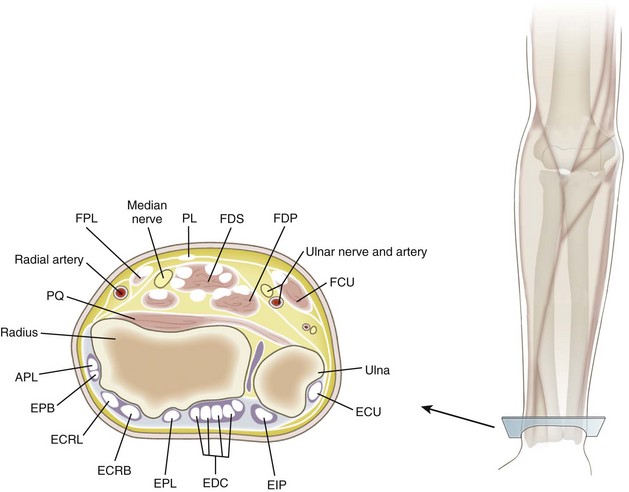
G Cross-sectional diagrams of proximal forearm (Figure 2-24), mid-forearm (Figure 2-25), and distal forearm (Figure 2-26)
 Ossification begins at the capitate (usually present at 1 year of age) and proceeds in a counterclockwise direction, according to posteroanterior radiographs of the right hand.
Ossification begins at the capitate (usually present at 1 year of age) and proceeds in a counterclockwise direction, according to posteroanterior radiographs of the right hand.
 Hamate is the second carpus to ossify (by ages 1 to 2 years).
Hamate is the second carpus to ossify (by ages 1 to 2 years).





 Pisiform, which is a large sesamoid bone, is the last to ossify (by age 9 years).
Pisiform, which is a large sesamoid bone, is the last to ossify (by age 9 years).
 Several key features are important to recognize in the individual carpal bones (Table 2-26).
Several key features are important to recognize in the individual carpal bones (Table 2-26).
Table 2-26
| Carpal Bone | Distinctive Features | Number of Articulations |
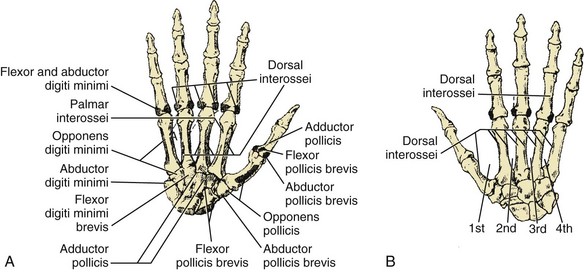
| Scaphoid | Tubercle (TCL, APB), distal vascular supply | 5 |
| Lunate | Half-moon–shaped | 5 |
| Triquetrum | Pyramid-shaped | 3 |
| Pisiform | Spheroidal (TCL, FCU) | 1 |
| Trapezium | FCR groove, tubercle (opponens, APB, flexor pollicis brevis, TCL) | 4 |
| Trapezoid | Wedge-shaped | 4 |
| Capitate | Largest bone, central location | 7 |
| Hamate | Hook (TCL) | 5 |
 These bones have two ossification centers:
These bones have two ossification centers:
 One for the body (primary center of ossification), which ossifies at 8 weeks of gestation (like most long bones)
One for the body (primary center of ossification), which ossifies at 8 weeks of gestation (like most long bones)
 One at the neck, which usually appears before 3 years of age
One at the neck, which usually appears before 3 years of age

 Several characteristics allow the identification of the individual metacarpals (Table 2-27).
Several characteristics allow the identification of the individual metacarpals (Table 2-27).
Table 2-27
| Metacarpal | Distinctive Features |
| I (Thumb) | Short, stout; base is saddle-shaped |
| II (Index) | Longest, largest base; medial at base |
| III (Middle) | Styloid process |
| IV (Ring) | Small quadrilateral base, narrow shaft |
| V (Small) | Tubercle at base (extensor carpi ulnaris) |
 Each hand has 14 phalanges (three for each finger and two for the thumb), which are similar.
Each hand has 14 phalanges (three for each finger and two for the thumb), which are similar.

 Bases of the proximal phalanges are oval and concave, with the smaller heads ending in two condyles.
Bases of the proximal phalanges are oval and concave, with the smaller heads ending in two condyles.
 Middle phalanges have two concave facets at their bases and pulley-shaped heads.
Middle phalanges have two concave facets at their bases and pulley-shaped heads.
 Distal phalanges are smaller and have palmar ungual tuberosities distally.
Distal phalanges are smaller and have palmar ungual tuberosities distally.
 The wrist is an ellipsoid joint and made up of the distal radius, scaphoid, lunate, triquetrum, and ligamentous structures (Table 2-28).
The wrist is an ellipsoid joint and made up of the distal radius, scaphoid, lunate, triquetrum, and ligamentous structures (Table 2-28).
Table 2-28
| Structure | Attachments | Distinctive Features |
| Articular capsule | Surrounds joint | Reinforced by volar and dorsal radiocarpal ligament |
| Volar (radiocarpal ligament) | Radius, ulna, scaphoid, lunate, triquetrum, capitate | Oblique ulnar, strong |
| Dorsal radiocarpal ligament | Radius, scaphoid, lunate, triquetrum | Oblique radial, weak |
| Ulnar collateral ligament | Ulna, triquetrum, pisiform, transverse carpal ligament | Fan-shaped, two fascicles |
| Radial collateral ligament | Radius, scaphoid, trapezium, transverse carpal ligament | Radial artery adjacent |
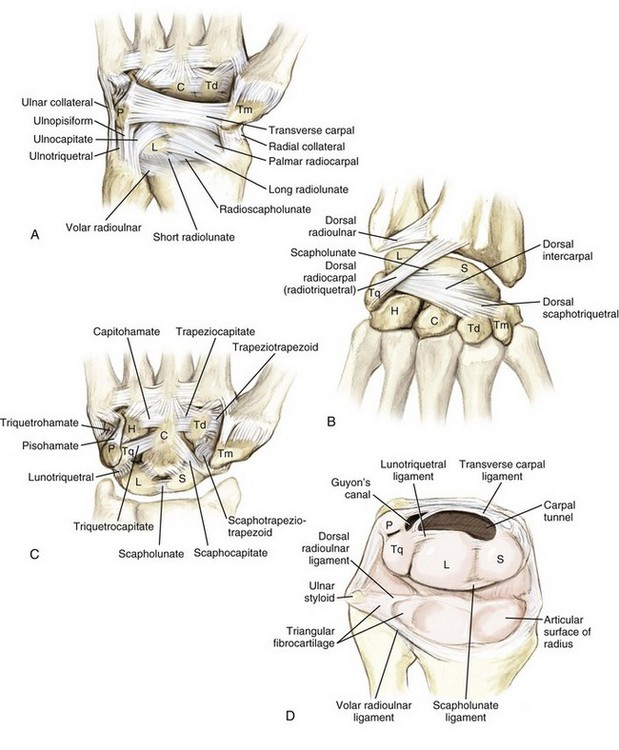
 The palmar/volar radiocarpal ligament is the strongest supporting structure, although it has a weak area on the radial side (the space of Poirier) that lends less support to the scaphoid, lunate, and trapezoid (Figure 2-27).
The palmar/volar radiocarpal ligament is the strongest supporting structure, although it has a weak area on the radial side (the space of Poirier) that lends less support to the scaphoid, lunate, and trapezoid (Figure 2-27).







 The pisotriquetral joint has a thin articular capsule.
The pisotriquetral joint has a thin articular capsule.
 The ulnar collateral and palmar radiocarpal ligaments also connect the pisiform proximally.
The ulnar collateral and palmar radiocarpal ligaments also connect the pisiform proximally.
 The pisohamate ligament and pisometacarpal ligaments help extend the pull of the FCU.
The pisohamate ligament and pisometacarpal ligaments help extend the pull of the FCU.








3. Carpometacarpal (CMC) joints








 This structure covers the dorsum of the wrist and contains six synovial sheaths (Figure 2-28).
This structure covers the dorsum of the wrist and contains six synovial sheaths (Figure 2-28).
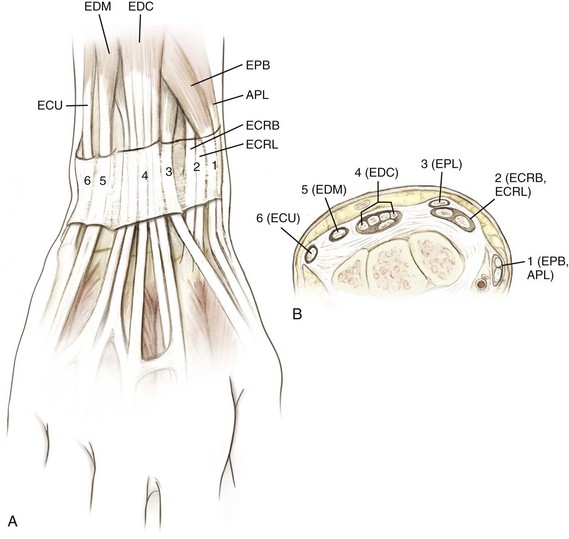
Figure 2-28 Extensor compartments of the wrist (1 to 6). See Table 2-29. APL, abductor pollicis longus; ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radialis longus; ECU, extensor carpi ulnaris; EDC, extensor digitorum communis; EDM, extensor digiti minimi; EPB, extensor pollicis brevis; EPL, extensor pollicis longus. (Modified from Miller MD, et al: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, Figure HW-6.)
 Orientation of the extensor tendons at the wrist is a key testable item (Table 2-29).
Orientation of the extensor tendons at the wrist is a key testable item (Table 2-29).
Table 2-29
| Compartment | Contents | Pathologic Condition |
| I | Abductor pollicis longus, extensor pollicis brevis | De Quervain’s tenosynovitis |
| II | Extensor carpi radialis longus, brevis | Extensor tendinitis (intersection syndrome) |
| III | Extensor pollicis longus | Rupture at Lister’s tubercle (after wrist fractures) Drummer’s tendinitis of the wrist |
| IV | Extensor digitorum communis, extensor indicis proprius | Extensor tenosynovitis |
| V | Extensor digiti minimi | Rupture (rheumatoid arthritis: Vaughn-Jackson syndrome) |
| VI | Extensor carpi ulnaris | Snapping at ulnar styloid |





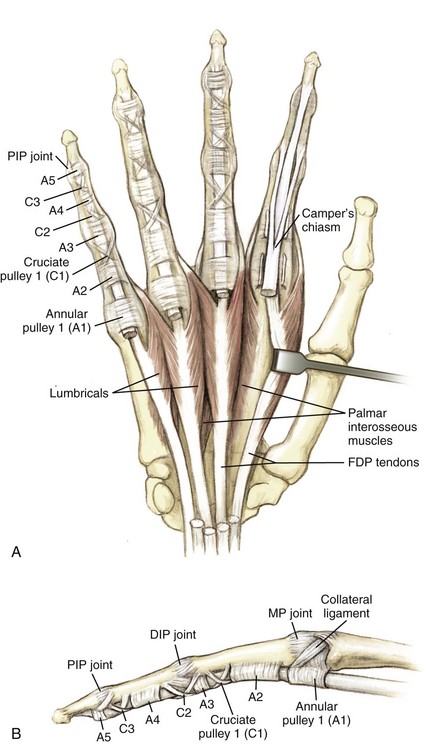
 Transverse carpal ligament (TCL)
Transverse carpal ligament (TCL)
 This is one component of the flexor retinaculum, which serves as the roof of the carpal tunnel (Figure 2-29).
This is one component of the flexor retinaculum, which serves as the roof of the carpal tunnel (Figure 2-29).
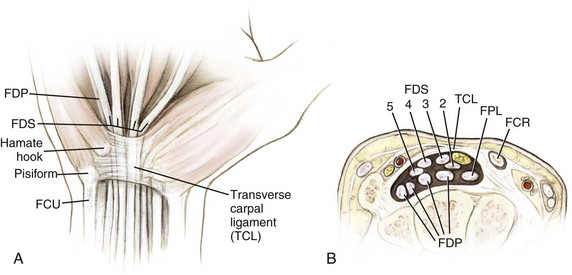

 Carpal tunnel decreases in volume with wrist flexion.
Carpal tunnel decreases in volume with wrist flexion.
 This tunnel contains the median nerve and nine tendons (one FPL, four FDS, and four FDP).
This tunnel contains the median nerve and nine tendons (one FPL, four FDS, and four FDP).

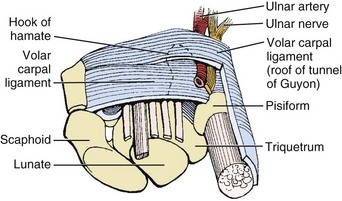
 The flexor retinaculum also forms the floor of Guyon’s canal, which is bordered as well by the hook of the hamate and the pisiform and is covered by the volar carpal ligament; the ulnar nerve can become entrapped in this canal (Figure 2-30).
The flexor retinaculum also forms the floor of Guyon’s canal, which is bordered as well by the hook of the hamate and the pisiform and is covered by the volar carpal ligament; the ulnar nerve can become entrapped in this canal (Figure 2-30).
 Triangular fibrocartilage complex
Triangular fibrocartilage complex
 This complex is formed by the triangular fibrocartilage, ulnocarpal ligaments (volar ulnolunate and ulnotriquetral ligaments), and a meniscal homolog.
This complex is formed by the triangular fibrocartilage, ulnocarpal ligaments (volar ulnolunate and ulnotriquetral ligaments), and a meniscal homolog.
 Injury to this structure is a common cause of ulnar wrist pain (see Figure 2-19).
Injury to this structure is a common cause of ulnar wrist pain (see Figure 2-19).
 Intrinsic apparatus (Table 2-30)
Intrinsic apparatus (Table 2-30)
Table 2-30
| Structure | Attachments | Significance |
| Sagittal bands | Covers MCP joint | Allows MCP extension |
| Transverse (sagittal) | Volar plate fibers | Allows MCP flexion (interossei) |
| Lateral bands | Covers PIP joint | Allows PIP extension (lumbrical muscles) |
| Oblique retinacular ligament (Landsmeer) | A4 pulley, terminal tendon | Allows DIP extension (passive) |
A4, annular 4; DIP, distal interphalangeal; MCP, metacarpophalangeal; PIP, proximal interphalangeal.

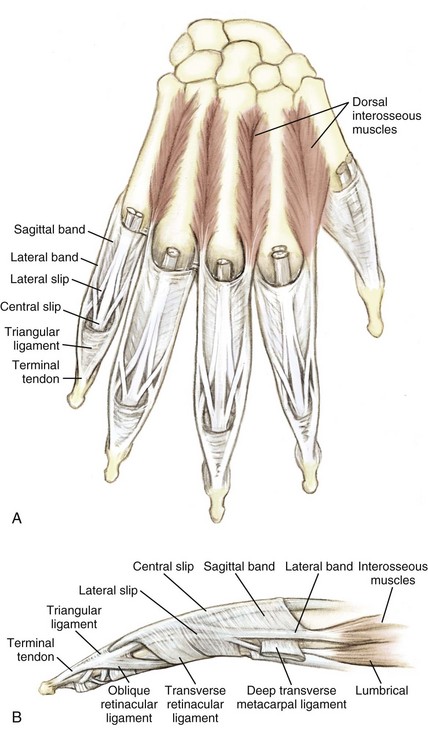






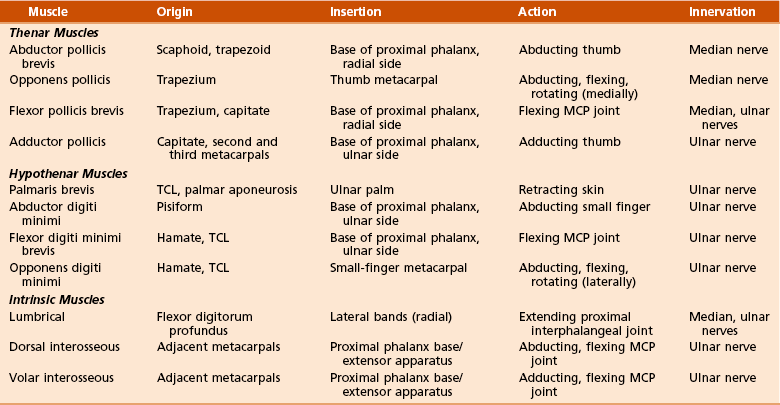
C Muscles (Table 2-31); origins and insertions (Figure 2-33)

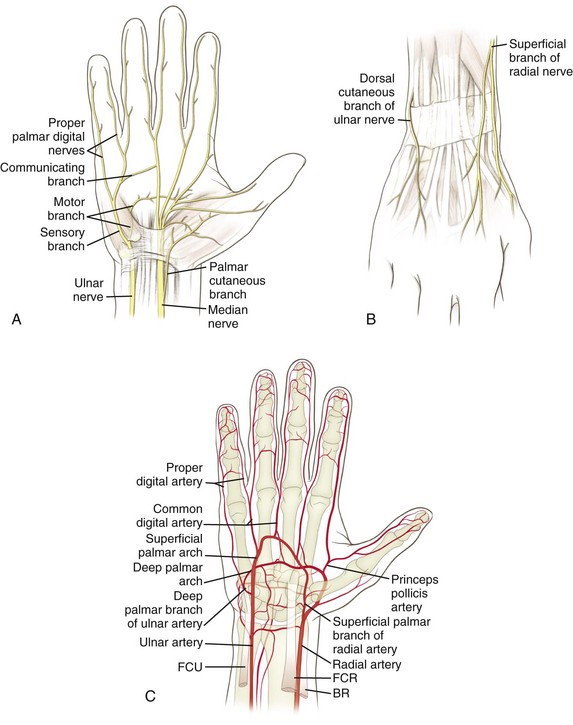

 This nerve enters the wrist just under the TCL, between the FDS and FCR.
This nerve enters the wrist just under the TCL, between the FDS and FCR.

 The deep (muscular) branch runs radially and innervates the thenar muscles.
The deep (muscular) branch runs radially and innervates the thenar muscles.







2. Innervation of the wrist and hand (Table 2-32)
Table 2-32
Innervation of the Wrist and Hand
| Nerve | Muscles Innervated |
| Median (medial and lateral cord) | Abductor pollicis brevis, superficial head of flexor pollicis brevis, opponens pollicis, first and second lumbrical muscles |
| Ulnar (medial cord) | Abductor digiti minimi, opponens digiti minimi, flexor digiti minimi, third and fourth lumbrical muscles, interossei, adductor pollicis, deep head of flexor pollicis brevis |
 At the wrist, the radial artery reaches the dorsum of the carpus by passing between (1) the FCR and (2) the APL and EPB tendons (snuffbox).
At the wrist, the radial artery reaches the dorsum of the carpus by passing between (1) the FCR and (2) the APL and EPB tendons (snuffbox).

 It forms the deep palmar arch in the hand.
It forms the deep palmar arch in the hand.
 The dorsal carpal branch of the radial artery enters the scaphoid dorsally and distally.
The dorsal carpal branch of the radial artery enters the scaphoid dorsally and distally.



F Surgical approaches to the wrist and hand (Table 2-33)
Table 2-33
Surgical Approaches to the Wrist
| Approach | Interval | Structures at Risk |
| Dorsal wrist | Third (extensor pollicis longus) and fourth (extensor digitorum communis) compartments | Transection of the innervation of the posterior interosseous nerve to the wrist capsule can be performed |
| Volar wrist | Flexor carpi radialis | Palmar cutaneous branch of median nerve |
| Volar scaphoid | Flexor carpi radialis and radial artery | Radial artery |
| Dorsolateral scaphoid | First and third compartments | Superficial radial nerve and radial artery |
1. Dorsal approach to the wrist (Figure 2-35)
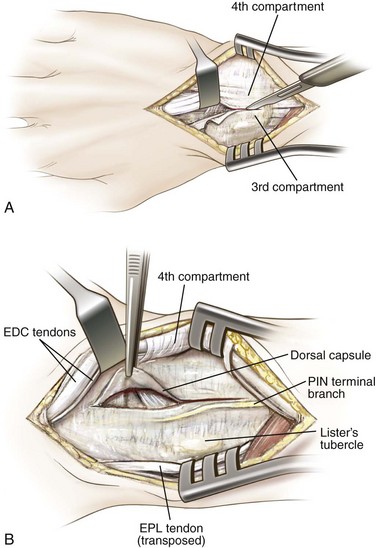
 Interval: between the third and fourth extensor compartments (EPL and extensor digitorum)
Interval: between the third and fourth extensor compartments (EPL and extensor digitorum)




 Risks: Do not violate the interosseous scapholunate ligament.
Risks: Do not violate the interosseous scapholunate ligament.
2. Carpal tunnel release (Figure 2-36)
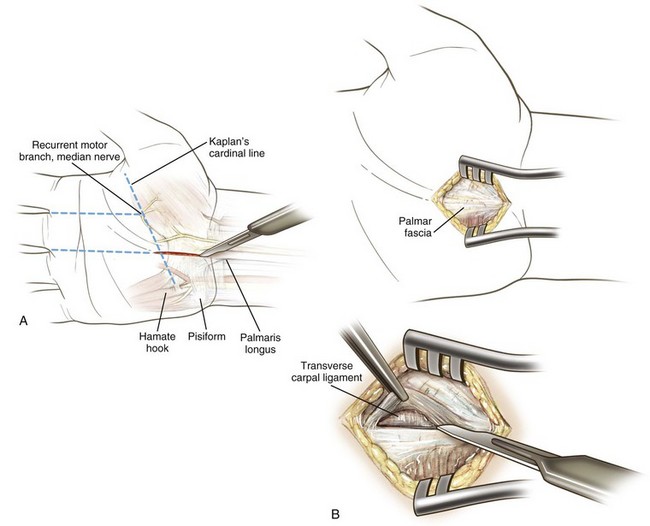
 Incision is usually made in line with the fourth ray to avoid the palmar cutaneous branch of the median nerve.
Incision is usually made in line with the fourth ray to avoid the palmar cutaneous branch of the median nerve.

3. Volar (Russé’s) approach to the scaphoid
 Interval: between the FCR and radial artery
Interval: between the FCR and radial artery
 An approach through the radial aspect of the FCR sheath: often easier and protects the radial artery
An approach through the radial aspect of the FCR sheath: often easier and protects the radial artery
4. Dorsolateral approach to the scaphoid
 Using an incision within the anatomic snuffbox (first and third dorsal wrist compartment) helps protect the superficial radial nerve and radial artery (deep).
Using an incision within the anatomic snuffbox (first and third dorsal wrist compartment) helps protect the superficial radial nerve and radial artery (deep).





section 3 Spine
1. Thirty-three vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 fused sacral, and 4 fused coccygeal
 Normal curves are cervical lordosis, thoracic kyphosis, lumbar lordosis, and sacral kyphosis.
Normal curves are cervical lordosis, thoracic kyphosis, lumbar lordosis, and sacral kyphosis.

 Important spine topographic landmarks are listed in Table 2-34.
Important spine topographic landmarks are listed in Table 2-34.
Table 2-34
| Topographic Landmark | Spinal Level |
| Mandible | C2-C3 |
| Hyoid cartilage | C3 |
| Thyroid cartilage | C4-C5 |
| Cricoid cartilage | C6 |
| Vertebra prominens | C7 |
| Scapular spine | T3 |
| Distal tip of scapula | T7 |
| Iliac crest | L4-L5 |
 The atlas (C1) has no vertebral body and no spinous process.
The atlas (C1) has no vertebral body and no spinous process.





 Atlantoaxial joint is diarthrodial.
Atlantoaxial joint is diarthrodial.
 Pannus in rheumatoid arthritis can affect this articulation and result in instability (see Chapter 8, Spine).
Pannus in rheumatoid arthritis can affect this articulation and result in instability (see Chapter 8, Spine).


 The vertebral artery travels in the transverse foramina of C6 to C1.
The vertebral artery travels in the transverse foramina of C6 to C1.


 Unique features include costal facets (present on all 12 vertebral bodies and the transverse processes of T1 to T9) and a rounded vertebral foramen.
Unique features include costal facets (present on all 12 vertebral bodies and the transverse processes of T1 to T9) and a rounded vertebral foramen.

 Lumbar vertebrae are the largest vertebrae and are higher anteriorly than posteriorly, significantly contributing to the lumbar lordosis.
Lumbar vertebrae are the largest vertebrae and are higher anteriorly than posteriorly, significantly contributing to the lumbar lordosis.










 Anterior longitudinal ligament (ALL)
Anterior longitudinal ligament (ALL)

 Thickest at center of vertebral body and thinnest at periphery
Thickest at center of vertebral body and thinnest at periphery
 Characterized by separate fibers extending from one to five levels
Characterized by separate fibers extending from one to five levels

 Posterior longitudinal ligament
Posterior longitudinal ligament
 Weaker than the anterior longitudinal ligament
Weaker than the anterior longitudinal ligament
 Extends from occiput (tectorial membrane) to the posterior sacrum
Extends from occiput (tectorial membrane) to the posterior sacrum



 Strong, yellow, elastic ligament connecting the laminae
Strong, yellow, elastic ligament connecting the laminae

 Hypertrophy of the ligamentum flavum is said to contribute to nerve root compression.
Hypertrophy of the ligamentum flavum is said to contribute to nerve root compression.




1. Spine stability (Denis model): the three-column system (Table 2-35)
Table 2-35
| Column | Composition |
| Anterior | Anterior longitudinal ligament, anterior two thirds of annulus and vertebral body |
| Middle | Posterior third of body and annulus, posterior longitudinal ligament |
| Posterior | Pedicles, facets and facet capsules, spinous processes, posterior ligaments that include interspinous and supraspinous ligaments, ligamentum flavum |

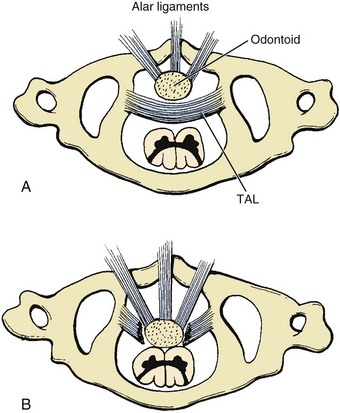
 Composed of two articular capsules (anterior and posterior) and the tectorial membrane (a cephalad extension of the posterior longitudinal ligament)
Composed of two articular capsules (anterior and posterior) and the tectorial membrane (a cephalad extension of the posterior longitudinal ligament)
 Further stabilization by the ligamentous attachments to the dens
Further stabilization by the ligamentous attachments to the dens









 The orientation of the facets of the spine dictates the plane of motion at each relative level.
The orientation of the facets of the spine dictates the plane of motion at each relative level.
 Facet orientation varies with the spinal level (Table 2-36).
Facet orientation varies with the spinal level (Table 2-36).
Table 2-36
| Spinal Level | Orientation of Sagittal Facet | Orientation of Coronal Facet |
| Cervical | 35 Degrees at C2, increasing to 55 degrees at C7 | Neutral, 0 degrees |
| Thoracic | 60 Degrees at T1, increasing to 70 degrees at T12 | 20 Degrees posterior |
| Lumbar | 137 Degrees at L1, decreasing to 118 degrees at L5 | 45 Degrees anterior |



 Annulus fibrosus: obliquely oriented composed of type I collagen
Annulus fibrosus: obliquely oriented composed of type I collagen
 Central nucleus pulposus: made of type II collagen and softer than the annulus
Central nucleus pulposus: made of type II collagen and softer than the annulus
 Nucleus pulposus: high polysaccharide content and approximately 88% water
Nucleus pulposus: high polysaccharide content and approximately 88% water
 Aging: results in the loss of water and conversion to fibrocartilage
Aging: results in the loss of water and conversion to fibrocartilage
 Intervertebral discs: account for 25% of the total height of the spinal column
Intervertebral discs: account for 25% of the total height of the spinal column


Table 2-37
| Muscle | Relationships |
| Longus capitis | Anterior to longus colli Posterior to sympathetic chain |
| Longus colli | Anterior to vertebral artery Posterior to longus capitis |
1. Neck: functional classification (anterior and posterior regions)

 This region contains the superficial platysma muscle (cranial nerve VII innervated), stylohyoid and digastric muscles (cranial nerve VII innervated) above the hyoid, and “strap” muscles below the hyoid.
This region contains the superficial platysma muscle (cranial nerve VII innervated), stylohyoid and digastric muscles (cranial nerve VII innervated) above the hyoid, and “strap” muscles below the hyoid.


















 The spinal cord extends from the brainstem to the inferior border of L1, where it terminates as the conus medullaris.
The spinal cord extends from the brainstem to the inferior border of L1, where it terminates as the conus medullaris.


 The cord also varies in diameter (widest at the origin of the plexuses).
The cord also varies in diameter (widest at the origin of the plexuses).
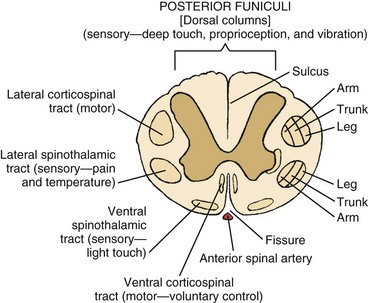
 In cross-section, the cord is observed to have both geographic and functional boundaries (Figure 2-38). It is divided in the midline anteriorly by a fissure and posteriorly by the sulcus.
In cross-section, the cord is observed to have both geographic and functional boundaries (Figure 2-38). It is divided in the midline anteriorly by a fissure and posteriorly by the sulcus.
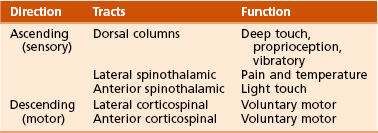
 Functional anatomy: The functions of the ascending (sensory) and descending (motor) tracts are summarized in Table 2-38.
Functional anatomy: The functions of the ascending (sensory) and descending (motor) tracts are summarized in Table 2-38.
 The posterior funiculi (dorsal columns) are located dorsally and receive ascending fibers, which deliver deep tactile, proprioceptive, and vibratory sensations.
The posterior funiculi (dorsal columns) are located dorsally and receive ascending fibers, which deliver deep tactile, proprioceptive, and vibratory sensations.
 The lateral spinothalamic tract transmits sensations of pain and temperature.
The lateral spinothalamic tract transmits sensations of pain and temperature.


 Sacral structures are the most peripheral in the lateral corticospinal tracts; cervical structures are more medial.
Sacral structures are the most peripheral in the lateral corticospinal tracts; cervical structures are more medial.
 This is why central cord syndrome affects the upper extremities more than the lower extremities.
This is why central cord syndrome affects the upper extremities more than the lower extremities.
 The ventral (anterior) spinothalamic tract transmits light tactile sensation.
The ventral (anterior) spinothalamic tract transmits light tactile sensation.
 Ventral (anterior) corticospinal tract delivers cortical messages of voluntary contraction.
Ventral (anterior) corticospinal tract delivers cortical messages of voluntary contraction.


 Incomplete spinal cord injury patterns are summarized in Table 2-39.
Incomplete spinal cord injury patterns are summarized in Table 2-39.
Table 2-39
Patterns of Incomplete Spinal Cord Injury
| Pattern of Injury | Functional Deficit | Recovery |
| Central (most common) | Upper extremity affected more than lower extremity, usually quadriparetic with sacral sparing; flaccid paralysis of upper extremity and spastic paralysis of lower extremity | 75% |
| Anterior | Complete motor deficit | 10% (worst prognosis) |
| Brown-Séquard | Unilateral cord injury with ipsilateral motor deficit, contralateral pain, and temperature deficit (two levels below injury) | >90% recovery |

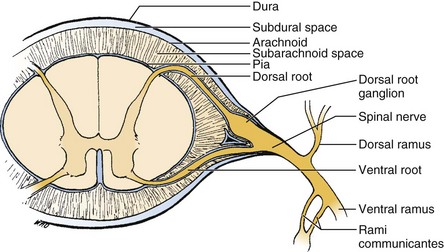
 There are 31 pairs of spinal nerves: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal.
There are 31 pairs of spinal nerves: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal.

 The nerve becomes “extradural” as it approaches the intervertebral foramen (the dura becomes epineurium) at all levels above L1.
The nerve becomes “extradural” as it approaches the intervertebral foramen (the dura becomes epineurium) at all levels above L1.
 Below this level, the nerves are contained within the cauda equina.
Below this level, the nerves are contained within the cauda equina.


 Ventral rami supply the anteromedial trunk and limbs.
Ventral rami supply the anteromedial trunk and limbs.


 In the lumbar spine, the nerve root traverses the respective disc space above the named vertebral body and exits the respective foramen under the pedicle (Figure 2-40).
In the lumbar spine, the nerve root traverses the respective disc space above the named vertebral body and exits the respective foramen under the pedicle (Figure 2-40).
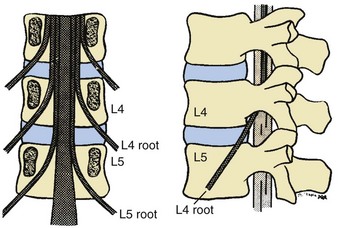
 Herniated discs usually impinge on the traversing nerve root and facet joint.
Herniated discs usually impinge on the traversing nerve root and facet joint.
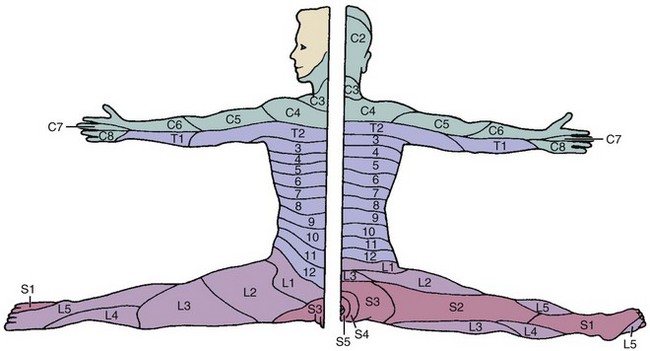
 For example, a disc herniation at the level of L4 to L5 would cause compression of the traversing L5 nerve root, resulting in a positive tension sign (straight-leg raise) and diminished strength in the hip abductors and extensor hallucis longus (EHL) and pain and numbness in the lateral leg to the dorsum of the foot (see Figure 2-12).
For example, a disc herniation at the level of L4 to L5 would cause compression of the traversing L5 nerve root, resulting in a positive tension sign (straight-leg raise) and diminished strength in the hip abductors and extensor hallucis longus (EHL) and pain and numbness in the lateral leg to the dorsum of the foot (see Figure 2-12).


 Key testable neurologic levels are listed in Table 2-40.
Key testable neurologic levels are listed in Table 2-40.
Table 2-40
Key Testable Neurologic Levels
| Neurologic Level | Representative Muscle | Reflex |
| C5 | Deltoid | Biceps |
| C6 | Wrist extension | Brachioradialis |
| C7 | Wrist flexion | Triceps |
| C8 | Finger flexion | |
| T1 | Interossei | |
| L4 | Tibialis anterior | Patellar |
| L5 | Toe extensors | |
| S1 | Peroneal | Achilles |
 Nerve root compression: A summary of the findings of nerve root compression is highlighted in Chapter 8, Spine (Tables 8-2 [cervical] and 8-7 [lumbar]). Dermatomes are key testable items (see Figure 2-12).
Nerve root compression: A summary of the findings of nerve root compression is highlighted in Chapter 8, Spine (Tables 8-2 [cervical] and 8-7 [lumbar]). Dermatomes are key testable items (see Figure 2-12).
 Cervical sympathetic chain posterior and medial to the carotid sheath
Cervical sympathetic chain posterior and medial to the carotid sheath


 Three ganglia of cervical sympathetic chain: superior, middle, and inferior (Table 2-41)
Three ganglia of cervical sympathetic chain: superior, middle, and inferior (Table 2-41)
Table 2-41
| Ganglion | Location | Comments |
| Superior | C2-C3 | Largest |
| Middle | C6 | Variable |
| Inferior | C7-T1 | Stellate |
 Disruption of the inferior ganglia can lead to Horner’s syndrome (ptosis, miosis [pupillary constriction], and anhidrosis).
Disruption of the inferior ganglia can lead to Horner’s syndrome (ptosis, miosis [pupillary constriction], and anhidrosis).

 Sympathetic ganglia: 11 in the thoracic region, 4 in the lumbar region, and 4 in the sacral region
Sympathetic ganglia: 11 in the thoracic region, 4 in the lumbar region, and 4 in the sacral region
1. Spinal blood supply from segmental arteries
 Located at vertebral midbodies via the aorta (which lies on the left side of the vertebral column; the inferior vena cava and azygos vein are on the right).
Located at vertebral midbodies via the aorta (which lies on the left side of the vertebral column; the inferior vena cava and azygos vein are on the right).
 Primary supply to the dura and posterior elements is from the dorsal branches.
Primary supply to the dura and posterior elements is from the dorsal branches.

2. Vertebral artery (a branch of the subclavian artery)
 Ascends through the transverse foramina of C1 to C6 (anterior to and not through C7) posterior to the longus colli muscle and then posterior to the lateral masses; courses along the cephalic surface of the posterior arch of C1 (atlas); and passes ventromedially around the spinal cord and through the foramen magnum before uniting at the midline basilar artery
Ascends through the transverse foramina of C1 to C6 (anterior to and not through C7) posterior to the longus colli muscle and then posterior to the lateral masses; courses along the cephalic surface of the posterior arch of C1 (atlas); and passes ventromedially around the spinal cord and through the foramen magnum before uniting at the midline basilar artery

3. Artery of Adamkiewicz (great anterior medullary artery)
 Enters through the left intervertebral foramen in the lower thoracic spine from T8 to T12; it supplies the interior two thirds of the anterior cord
Enters through the left intervertebral foramen in the lower thoracic spine from T8 to T12; it supplies the interior two thirds of the anterior cord



F Surgical approaches to the spine (Table 2-42, Figure 2-41)
Table 2-42
Surgical Approaches to the Spine
| Approach | Interval | Structures at Risk |
| Anterior cervical | Carotid sheath and the trachea | Recurrent laryngeal nerve Sympathetic ganglion |
| Posterior cervical | Midline approach between paracervical muscle | Vertebral artery |
| Anterior thoracic | Transverse between ribs two levels above surgical site | Intercostal neurovascular bundle; to avoid, dissect over top of rib |
| Posterior thoracolumbar | Midline approach over spinous processes | Posterior primary rami and segmental vessels; protect nerve root |
| Anterior lumbar (transperitoneal) | Between segmentally innervated rectus abdominis | Presacral plexus of parasympathetic nerve |
1. Anterior approach to the cervical spine
 Incision: transverse and based on the desired level (e.g., for C5, the carotid triangle should be entered)
Incision: transverse and based on the desired level (e.g., for C5, the carotid triangle should be entered)









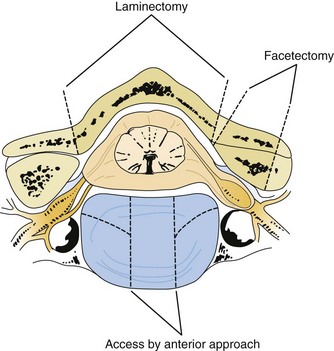
2. Posterior approach to the cervical spine


 After a midline approach through the ligamentum nuchae, reflect the superficial (trapezius) and intermediate (splenius, semispinalis, longissimus capitis) layers laterally; the vertebrae are exposed.
After a midline approach through the ligamentum nuchae, reflect the superficial (trapezius) and intermediate (splenius, semispinalis, longissimus capitis) layers laterally; the vertebrae are exposed.
 Access to the spinal canal is through laminectomy or facetectomy.
Access to the spinal canal is through laminectomy or facetectomy.




3. Anterior (transthoracic) approach to the thoracic spine
 Incision: transverse, made approximately two ribs above the level of interest
Incision: transverse, made approximately two ribs above the level of interest







4. Posterior approach to the thoracolumbar spine
 Incision: straight, midline, over the spinous processes and carried down through the thoracolumbar fascia
Incision: straight, midline, over the spinous processes and carried down through the thoracolumbar fascia







5. Anterior approach to the lumbar spine (transperitoneal)
 Incision: longitudinal, from below the umbilicus to just above the pubic symphysis
Incision: longitudinal, from below the umbilicus to just above the pubic symphysis






6. Anterolateral approach to the lumbar spine (retroperitoneal)
 Incision: oblique, centered over the twelfth rib to the lateral border of the rectus abdominis muscle
Incision: oblique, centered over the twelfth rib to the lateral border of the rectus abdominis muscle











[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]Chapter 2
Anatomy
section 1 Introduction
A Osteology: The human skeleton has 206 bones: axial skeleton (80) and appendicular skeleton (126)
Intramembranous (direct laying down of bone without a cartilage model [skull]) or enchondral (with a cartilage precursor [most bones]).
Enchondral growth begins in the diaphyses of long bones at primary ossification centers, most of which are present at birth (Table 2-1).
2. Secondary ossification centers usually develop in the periphery of bones and are important for growth and the treatment of childhood fractures.
3. Heterotopic ossification is the formation of bone tissue in an atypical, extraskeletal location.
4. Anatomic landmarks of the skeleton and their related structures are listed in Table 2-2.
B Arthrology: Joints are commonly classified into three types on the basis of their freedom of movement
1. Synarthroses: joining of two bony elements with no motion during maturity; skull sutures
2. Amphiarthroses: have hyaline cartilage and intervening discs with limited motion; symphysis pubis
3. Diarthroses: characterized by hyaline cartilage, synovial membranes, capsules, and ligaments
C Myology: classification based on the arrangement of muscle fibers
2. Fusiform (e.g., biceps brachii)
3. Oblique (with tendinous interdigitation): further classified as pennate, bipennate, multipennate
Originate from the ventral rami of spinal nerves and are distributed via several plexuses (cervical, brachial, lumbosacral)
Efferent (motor) fibers carry impulses from the central nervous system to muscles.
Afferent (sensory) fibers carry information toward the central nervous system.
section 2 Upper Extremity
Table 2-3 summarizes upper extremity innervation. Table 2-4 summarizes standard surgical approaches to the upper extremity.
Table 2-3
Summary of Upper Extremity Innervation
| Nerves | Muscles Innervated |
| Musculocutaneous (lateral cord) | Coracobrachialis, biceps, brachialis |
| Axillary (posterior cord) | Deltoid, teres minor |
| Radial (posterior cord) | Triceps, brachioradialis, extensor carpi radialis longus and brevis |
| Posterior interosseous | Supinator, extensor carpi ulnaris, extensor digitorum, extensor digiti minimi, abductor pollicis longus, extensor pollicis longus and brevis, extensor indicis proprius |
| Median (medial and lateral cord) | Pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, abductor pollicis brevis, supinator head of flexor pollicis brevis, opponens pollicis, first and second lumbrical muscles |
| Anterior interosseous | Flexor digitorum profundus (first and second), flexor pollicis longus, pronator quadratus |
| Ulnar (medial cord) | Flexor carpi ulnaris, flexor digitorum profundus (third and fourth), palmaris brevis, abductor digiti minimi, opponens digiti minimi, flexor digiti minimi, third and fourth lumbrical muscles, interossei, adductor pollicis, deep head of flexor pollicis brevis |
Spans the second through seventh ribs and serves as an attachment for 17 muscles and four ligaments
Glenoid is retroverted approximately 5 degrees.
It is the fulcrum for lateral movement of the arm.
The clavicle is the first bone in the body to ossify (at 5 weeks of gestation) and the last to fuse (medial epiphysis at 25 years of age; see Table 2-1). Fracture of the clavicle is the most common musculoskeletal birth injury.
B Arthrology: one major articulation (glenohumeral joint) and several minor articulations (sternoclavicular, acromioclavicular, scapulothoracic joints)
1. Glenohumeral joint (Figure 2-1): Spheroidal, ball and socket, with the greatest joint range of motion; motion is at the expense of stability with static and dynamic restraints.
Static restraints include the articular anatomy, glenoid labrum, negative pressure, capsule, and ligaments.
Important glenohumeral stabilizers summarized in Table 2-5
Table 2-5
| Structure | Function |
| Coracohumeral ligament | Primary restraint in inferior translation of the adducted arm and to external rotation |
| Glenoid labrum | Increases surface area, static stabilizer |
| Superior glenohumeral ligament | Primary restraint in external rotation of the adducted or slightly abducted arm Primary restraint in inferior translation of the adducted arm |
| Middle glenohumeral ligament (absent up to 30% of shoulders) | Primary stabilizer in anterior translation, with the arm abducted to 45 degrees |
| Inferior glenohumeral ligament complex | Primary stabilizer for anterior and inferior translation in abduction |
This joint is double-gliding, with an articular disc.
The sternoclavicular joint rotates 30 degrees with shoulder motion.
Plane/gliding joint with a fibrocartilaginous disc
Figure 2-2 Ligaments about the shoulder. The acromioclavicular ligaments (superior, inferior, anterior, and posterior) prevent anteroposterior translation of the distal clavicle. The superior ligament is the most important and is reinforced by fibers from the trapezius and deltoid muscles. The coracoclavicular ligaments—conoid (posteromedial) and trapezoid (anterolateral)—prevent superior translation of the distal clavicle. The coracoacromial ligament should be preserved in massive rotator cuff defects because it provides superior restraint to the humeral head. Bleeding encountered during release of the coracoacromial ligament comes from the acromial branch of the thoracoacromial artery (second part of axillary artery; see Figure 2-6). (Adapted from Jenkins DB: Hollinshead’s functional anatomy of the limbs and back, ed 6, Philadelphia, 1991, Saunders, p 71.)
Though not a true joint, this attachment allows scapular movement against the posterior rib cage.
Fixed primarily by the scapular muscular attachments.
Glenohumeral motion in comparison with scapulothoracic motion is in a 2:1 ratio.
1. Muscles connecting the upper limb to the vertebral column: trapezius, latissimus, both rhomboid muscles, and levator scapulae
2. Muscles connecting the upper limb to the thoracic wall: both pectoralis muscles, subclavius, and serratus anterior
3. Muscles acting on the shoulder joint itself: deltoid, teres major, and the four rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis)
The rotator cuff muscles depress and stabilize the humeral head against the glenoid; all attach to the greater tuberosity except the subscapularis, which has a lesser tuberosity insertion (shoulder internal rotator).
Table 2-6 presents the specific characteristics of these muscles, and Figure 2-4 and Table 2-7 describe the four layers of shoulder musculature.
Table 2-7
Shoulder-Supporting Anatomic Layers
| Layer | Structures |
| I | Deltoid; pectoralis major; trapezius |
| II | Clavipectoral fascia; conjoined tendon, short head of biceps, and coracobrachialis |
| III | Deep layer of subdeltoid bursa; rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis [SITS]) |
| IV | Glenohumeral joint capsule; coracohumeral ligament |
1. Anatomy of brachial plexus (Figure 2-5)
The brachial plexus is formed from the ventral primary rami of C5 to T1 and lies under the clavicle between the scalenus anterior and scalenus medius.
Dorsal rami of C5 to T1 innervate the dorsal neck musculature and skin.
Five roots (C5 to T1, although contributions from C4 and T2 can be small)
Three trunks (upper, middle, lower)
Six divisions (two from each trunk)
Three cords (named because of their anatomic relationship to the axillary artery: posterior, lateral, and medial); the termination of each cord is shown in Table 2-8
Table 2-8
Brachial Plexus Cord Terminations
| Cord | Termination |
| Lateral | Musculocutaneous nerve* Lateral pectoral nerve |
| Posterior | Radial and axillary nerve* Upper and lower subscapular nerve Thoracodorsal nerve |
| Medial | Ulnar nerve* Medial pectoral nerve Medial brachial cutaneous nerve Medial antebrachial cutaneous nerve |
| Medial and lateral | Median nerve* |
Multiple branches: four preclavicular branches (from roots and upper trunk):
2. Muscle innervation: innervation of all rotator cuff muscles derived from C5 and C6 of the brachial plexus (Table 2-9; see also Table 2-3)
The left subclavian artery arises directly from the aorta, and the right subclavian artery arises from the brachiocephalic trunk.
F Surgical approaches to the shoulder (Table 2-12; see Table 2-4):
Table 2-12
Surgical Approaches to the Shoulder
| Approach | Interval | Structures at Risk |
| Anterior (Henry’s) | Deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerve) | Axillary nerve limits inferior exposure; place arm in adduction and external rotation Musculocutaneous nerve: avoid vigorous retraction and medial dissection to the conjoined tendon/coracobrachialis |
| Lateral | Deltoid splitting (axillary nerve) | Avoid deltoid split >5 cm below acromion, to avoid damaging axillary nerve |
| Posterior | Infraspinatus (suprascapular nerve) and teres minor (axillary nerve) | Dissection inferior to the teres minor puts quadrangular space structures at risk: axillary nerve and posterior humeral circumflex artery Avoid excessive medial retraction on infraspinatus, which can injure suprascapular nerve |
1. Anterior (Henry’s) approach (Figure 2-7)
Interval: deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves)
Dissect the cephalic vein, and retract it laterally with the deltoid, thereby exposing the underlying subscapularis.
G Arthroscopy (discussed in Chapter 4, Sports Medicine)
Articulates with the smaller scapular glenoid cavity
Retroverted 30 degrees (in relation to the transepicondylar axis of the humerus)
2. Anatomic neck, directly below the humeral head, serves as an attachment for the shoulder capsule.
3. Surgical neck is lower and is more often involved in fractures.
4. Greater tuberosity is lateral to the humeral head.
Serves as the attachment for the supraspinatus, infraspinatus, and teres minor muscles (anterior to posterior, respectively)
5. Lesser tuberosity, located anteriorly, has only one muscular insertion: the last rotator cuff muscle, the subscapularis.
6. Bicipital groove (for the tendon of the long head of the biceps brachii) is a bony groove between the two tuberosities.
7. Humeral shaft has a posterior spiral groove (for the radial nerve) adjacent to the deltoid tuberosity and approximately 13 cm above the articular surface of the trochlea.
8. Distally, the humerus flares into medial and lateral epicondyles.
Elbow is composed of a hinge joint (the humeroulnar articulation) and a pivot joint (the humeroradial articulation) (Table 2-13).
Table 2-13
| Articulation | Components |
| Humeroulnar | Trochlea and trochlear notch |
| Humeroradial | Capitulum and radial head |
| Proximal radioulnar | Radial notch and radial head |
Elbow joint has capsuloligamentous tissues (Figure 2-9) that are a key source of testable material.
Table 2-14
| Ligament | Components | Comments |
| Medial collateral | Anterior bundle of MCL (ulnar collateral); posterior bundle; transverse bundle (Cooper ligament) | Anterior bundle (strongest of all elbow ligaments): anterior band taut from 60 degrees of flexion to full extension, posterior band taut from 60-120 degrees of flexion |
| Lateral collateral | LUCL; annular ligament; quadrate (annular ligament to radial neck) and oblique cord | Deficiency of LUCL results in posterolateral rotator instability |
LUCL, lateral ulnar collateral ligament; MCL, medial collateral ligament.
The medial collateral ligament (MCL) (anterior, posterior, and transverse bundles) arises from the anteroinferior portion of the medial humeral epicondyle and provides stability in valgus stress.
C Muscles: four muscles of the arm controlling elbow motion (Table 2-15)
1. Flexors (biceps, brachialis, and brachioradialis); the brachialis attaches to the coronoid at 11 mm distal to the tip
2. Extensors (triceps); also helps form borders for three important spaces (Figure 2-10 and Table 2-16)
Four major nerves traverse the arm; two give off branches to arm musculature, and two innervate the distal musculature (Figure 2-11). Most of the cutaneous innervation of the arm arises directly from the brachial plexus.
Musculocutaneous nerve (lateral cord):
Pierces the coracobrachialis 5 to 8 cm distal to the coracoid
Branches to supply the coracobrachialis, the biceps, and the brachialis
Radial nerve (posterior cord):
Spirals around the humerus (medial to lateral) in the spiral groove at a distance of approximately 13 cm from the trochlea
Median nerve (medial and lateral cords):
Accompanies the brachial artery along the arm, crossing it during its course (lateral to medial)
Supplies some branches to the elbow joint but has no branches in the arm itself
Passes medial to the brachial artery in the arm and then runs behind the medial epicondyle of the humerus, where it is superficial
2. Compressive neuropathies (Table 2-17)
Table 2-17
Nerve Compression Syndromes of the Arm and Forearm
| Syndrome | Nerve Involved | Sites of Compression |
| Pronator | Median | Supracondylar process of humerus and ligament of Struthers Lacertus fibrosis (bicipital aponeurosis) Pronator teres Arch of flexor digitorum superficialis |
| AIN | AIN of median | Deep head of pronator teres Flexor digitorum superficialis Aberrant vessels Accessory muscles (i.e., Gantzer’s muscles) |
| Cubital tunnel | Ulnar | Arcade of Struthers Medial intermuscular septum Medial epicondyle Cubital tunnel Proximal edge of flexor carpi ulnaris (Osborne fascia) Deep flexor pronator aponeurosis |
| PIN Radial tunnel |
PIN of radial | Fibrous bands Recurrent leash of Henry Extensor carpi radialis brevis Arcade of Frohse (proximal edge of superficial head of supinator) Supinator distal margin |
| Superficial radial nerve | Superficial radial | Between the brachioradialis and extensor carpi radialis longus |
AIN, anterior interosseous nerve; PIN, posterior interosseous nerve.
Originates at the lower border of the tendon of the teres major and continues to the elbow, where it bifurcates into the radial and ulnar arteries (see Figure 2-11)
Lies medial in the arm, curving laterally to enter the cubital fossa
Deep brachial (also known as the profunda, this artery accompanies the radial nerve posteriorly in the triangular interval)
Superior and inferior ulnar collateral arteries
The nutrient and muscular branches
The supratrochlear artery (the least flexible branch)
These collateral vessels can bind up the brachial artery with distal humerus fractures
F Surgical approaches to the humerus. (Table 2-18)
Table 2-18
Surgical Approaches to the Humerus
| Approach | Interval | Structures at Risk |
| Anterolateral—proximal | Proximal—deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerve) Distal—brachialis (radial and musculocutaneous nerve) |
Radial nerve; axillary nerve; anterior humeral circumflex artery |
| Posterior | Triceps (radial nerve); lateral and long heads | Radial nerve; deep brachial artery |
