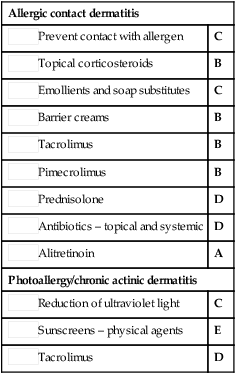
| Allergic contact dermatitis |
 Prevent contact with allergen Prevent contact with allergen |
C |
 Topical corticosteroids Topical corticosteroids |
B |
 Emollients and soap substitutes Emollients and soap substitutes |
C |
 Barrier creams Barrier creams |
B |
 Tacrolimus Tacrolimus |
B |
 Pimecrolimus Pimecrolimus |
B |
 Prednisolone Prednisolone |
D |
 Antibiotics – topical and systemic Antibiotics – topical and systemic |
D |
 Alitretinoin Alitretinoin |
A |
| Photoallergy/chronic actinic dermatitis |
 Reduction of ultraviolet light Reduction of ultraviolet light |
C |
 Sunscreens – physical agents Sunscreens – physical agents |
E |
 Tacrolimus Tacrolimus |
D |



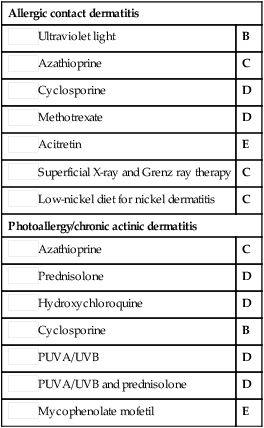
 Ultraviolet light
Ultraviolet light Azathioprine
Azathioprine Cyclosporine
Cyclosporine Methotrexate
Methotrexate Acitretin
Acitretin Superficial X-ray and Grenz ray therapy
Superficial X-ray and Grenz ray therapy Low-nickel diet for nickel dermatitis
Low-nickel diet for nickel dermatitis Azathioprine
Azathioprine Prednisolone
Prednisolone Hydroxychloroquine
Hydroxychloroquine Cyclosporine
Cyclosporine PUVA/UVB
PUVA/UVB PUVA/UVB and prednisolone
PUVA/UVB and prednisolone Mycophenolate mofetil
Mycophenolate mofetil