[level-membership-for-dermatology-category]
Allergic contact dermatitis and photoallergy



First-line therapies
 Prevent contact with allergen
Prevent contact with allergen Topical corticosteroids
Topical corticosteroids Emollients and soap substitutes
Emollients and soap substitutes Barrier creams
Barrier creams Tacrolimus
Tacrolimus Pimecrolimus
Pimecrolimus Prednisolone
Prednisolone Antibiotics – topical and systemic
Antibiotics – topical and systemic Alitretinoin
Alitretinoin Reduction of ultraviolet light
Reduction of ultraviolet light Sunscreens – physical agents
Sunscreens – physical agents Tacrolimus
Tacrolimus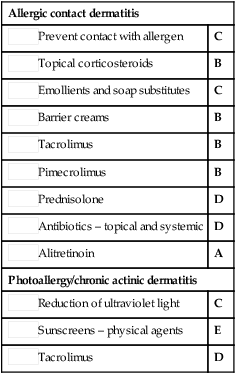
Second-line therapies
 Ultraviolet light
Ultraviolet light Azathioprine
Azathioprine Cyclosporine
Cyclosporine Methotrexate
Methotrexate Acitretin
Acitretin Superficial X-ray and Grenz ray therapy
Superficial X-ray and Grenz ray therapy Low-nickel diet for nickel dermatitis
Low-nickel diet for nickel dermatitis Azathioprine
Azathioprine Prednisolone
Prednisolone Hydroxychloroquine
Hydroxychloroquine Cyclosporine
Cyclosporine PUVA/UVB
PUVA/UVB PUVA/UVB and prednisolone
PUVA/UVB and prednisolone Mycophenolate mofetil
Mycophenolate mofetil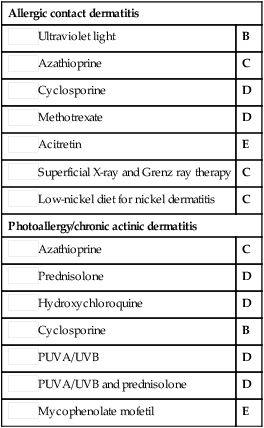

[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Allergic contact dermatitis and photoallergy
