CHAPTER 16 Adjuncts for challenging cases

Epidemiologic consideration and terminology
Large multi-surgeon series report intraoperative complications rates in the order of 2% with up to 5% of eyes with no prior co-pathology (and 9% of all eyes) not achieving vision better than 20/401. Many of these are ascribable to the situations described above.
Clinical features, diagnosis and differential diagnosis
Adjunctive devices are useful in the setting of small pupils not responding to mydriatics, iris prolapse, or intraoperative floppy iris syndrome (IFIS)2 to maintain pupil dilatation whilst stabilizing iris tissue allowing safe phacoemulsification to be completed. Usually risk factors will be apparent in the preoperative assessment, including a history of uveitis, posterior synechiae, use of alpha antagonist drugs such as tamsulosin and a history of trauma or previous intraocular surgery, but the pupil can sometimes miose intraoperatively without any predisposing conditions. It is therefore imperative for all cataract surgeons to be conversant with strategies to deal with small pupils and IFIS.
Fundamental principles
Numerous dyes have been used for the purpose of capsular staining, including indocyanine green (ICG), fluorescein, crystal violet, gentian violet, and brilliant blue G. Trypan blue marketed as Vision Blue (DORC International, Zuidland, The Netherlands) is by far the most popular in contemporary practice and is FDA (US Food and Drug Administration) approved. The Ophthalmic Technology Assessment Committee Anterior Segment Panel of the American Academy of Ophthalmology published their recommendations on capsular staining for cataract surgery in 2006 finding considerable data on the safety of trypan blue in the anterior chamber3. This dye has a well-established safety record; none the less occasional concerns have been raised about its safety, with some apoptotic cell death having been reported4. It is therefore important to use dyes only when needed and in the smallest amount which achieves the surgical outcome.
Flexible iris hook-retractors5 are versatile; aside from their use in small pupil, iris prolapse, and IFIS, they are also useful in the setting of iridoschisis and as a capsular support in cases of zonular loss or subluxed lenses.
A range of ring expanders are available including The Perfect Pupil Device (Milvella, Sydney, Australia), which is a flexible ring with a flanged groove and scalloped tabs to hold a billowing floppy iris through 315° leaving an open area of 45° to accommodate the passage of instruments. The Morcher pupil-dilator ring (Morcher, Stuttgart, Germany) is a fixed 7.5 mm polymethyl methacrylate (PMMA) ring. It is a rigid device which can be difficult to insert and remove. The Graether pupil-expander system (Eagle Vision, Memphis, TN, USA) is another option. This is an incomplete soft silicone ring, with a grooved outer surface to engage the iris which is preloaded in a disposable insertion tool. More recently, the Malyugin ring (MicroSurgical Technology, Redmond, Washington) has gained popularity and is now the device of choice for most surgeons6. This rectangular device, made of 5-0 polypropylene, uses the scroll principle to catch the pupillary margin. It is available in two sizes, 6.25 mm and 7 mm. The main advantages of this device include gentle and less traumatic fixation of the iris margin and controlled stretching of the pupil. The single use package includes a holder and inserter with the ring. The inserter is used to withdraw the ring from the holder. It also introduces the ring into the anterior chamber and removes the ring from the eye.
A 10-0 Prolene suture on CIF-4 (Ethicon, USA) needles is the preferred suture for most surgeons. The suture should be placed under a scleral flap or within a scleral pocket7. The M-CTR can increase zonular damage when it is being implanted as the ring has to be dialled into a position where the fixation islet is in the area of maximal zonular loss. Ahmed introduced the capsular tension segment (CTS)8, which is a smaller device; this can be positioned directly into the area of zonular loss, which reduces the potential to cause further damage to the zonular apparatus during implantation. The CTS is very versatile and can be used in combination with a standard CTR to achieve the same result as an M-CTR, but with less traumatic surgery (Fig. 16.1 a,b).
Operation techniques
Trypan blue has traditionally been applied in the anterior chamber after it has been filled with air, to allow it to stain the capsule whilst minimizing contact with other tissue. The air bubble limits contact of dye with the central corneal endothelium, but the meniscus encourages contact with the iris and the peripheral corneal endothelium. A more elegant technique is to fill the anterior chamber with an ophthalmic visco-elastic device (OVD) and then apply a very small aliquot of dye under OVD directly onto the capsule. This can then be spread by the applying cannula, akin to painting the anterior capsule9. This minimizes the contact of dye with other structures and is more time-efficient. A ‘top-up’ with OVD following this maneuver pushes excess dye into the periphery and allows the CCC to be initiated and completed in a controlled manner (Fig. 16.2). Trypan blue can also be deployed after the CCC has been initiated if visibility deteriorates or the edge of the CCC cannot be visualized. This is best done directly under OVD by applying a drop of dye in the area of the tear to aid visualization and retrieval of the developing CCC edge, a strategy which is very beneficial when combined with techniques to retrieve a CCC which is tearing out.
Use of flexible iris hook-retractors needs attention to technique to avoid complications such as a wide, raised iris platform between hooks, iris prolapse, or iridodialysis. Tears of either the anterior capsule or Descemet’s membrane and irregular postoperative pupil function can also ensue. The paracentesis used should be parallel to the iris plane to avoid drawing the iris forward when the hooks are engaged. OVD is used to deepen the sulcus plane and create space between the capsule and iris to avoid damaging the capsule. Overstretching of the pupil should be avoided and hooks should be placed symmetrically (Fig. 16.3). Placing the hooks in a diamond configuration with one of the hooks placed in a subincisional location allows for good surgical access.
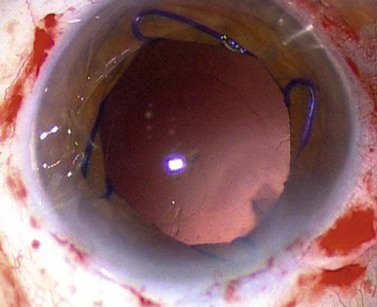
The Malyugin ring can be deployed at any stage of the procedure, either before capsulorrhexis has been done, or at a later stage if progressive miosis or IFIS is encountered. The ring is loaded into the inserter. Then, it is inserted through a 2.2 mm or larger incision. Surgeons using microincision surgery should use a separate 2.2 mm clear corneal incision as the injector will not pass through an incision smaller than 2.2 mm. The tip of the inserter is positioned at the center of the anterior chamber. As the ring is injected, it is released from the tip until the distal scroll is engaged with the distal iris. Both lateral scrolls then emerge from the tube of the inserter and simultaneously catch the iris margins. The proximal scroll is expelled from the inserter lying on top of the iris. The inserter is withdrawn from the eye, and a hook is used to push the proximal scroll into the pupillary space and engage the iris margin. Once the phacoemulsification and IOL implantation are done, the ring is then removed from the eye in the reverse order. The Malyugin ring is a flexible device which is easy to insert without the need for multiple incisions; it is particularly useful in patients in whom cutting or tearing of the iris tissue needs to be avoided, e.g. in the presence of rubeosis, chronic anterior uveitis, or systemic coagulopathy. The device provides a controlled stretching of the pupil and engages a wider area of the pupillary margin than iris hooks and is therefore less prone to tearing the sphincter. The iris rim is safely fixed in the ring’s loops, eliminating the risk of iris aspiration during phacoemulsification (Fig. 16.4).
Scleral fixation of a posterior chamber lens is an elegant technique to manage aphakia or to secure a posterior chamber lens when capsular support is inadequate. Rigid PMMA IOLs with eyelets incorporated in the haptics are available to allow secure suturing to the sclera. Foldable lenses can also be sutured to the ciliary sulcus. Late suture breakage leading to IOL decentration or frank luxation remains a concern in the long term. The use of scleral pockets without conjunctival dissection reduces the risk of late suture exposure compared with the use of scleral flaps7. Recently techniques of sutureless scleral fixation using scleral tunnels into which haptics are buried have gained popularity and potentially eliminate the potential for suture related complications10.
1 Jaycock P, Johnston RL, Taylor H, et alUK EPR user group. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye (Lond). 2009;23(1):38-49.
2 Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated with tamsulosin (Flomax). J Cataract Refract Surg. 2005;31:664-673.
3 Jacobs DS, Cox TA, Wagoner MD, et al. Capsule Staining as an Adjunct to Cataract Surgery: A Report from the American Academy of Ophthalmology. Ophthalmology. 2006;113(4):707-713.
4 Hisatomi T, Enaida H, Matsumoto H, et al. Staining ability and biocompatibility of brilliant blue G: preclinical study of brilliant blue G as an adjunct for capsule staining. Arch Ophthalmol. 2006;124:514-519.
5 Mackool RJ. Small pupil enlargement during cataract extraction: a new method. J Cataract Refract Surg. 1992;18:523-526.
6 Malyugin B. Small pupil phaco surgery: a new technique. Ann Ophthalmol (Skokie). 2007;39(3):185-193.
7 Hoffman RS, Fine IH, Packer M. Scleral fixation without conjunctival dissection. J Cataract Refract Surg. 2006;32(11):1907-1912.
8 Hasnee K, Butler M, Ahmed I. Capsular tension rings and related devices: current concepts. Current Opin Ophthalmol. 2006;17:31-41.
9 Caporossi A, Balestrazzi A, Alegente M, et al. Trypan blue staining of the anterior capsule: the one-drop technique. Ophthal Surg Lasers Imaging. 2005;36:432-434.
10 Scharioth GB, Pavlidis MM. Sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg. 2007;33(11):1851-1854.





