Chapter 616 Abnormalities of the Lids
Ptosis
Although ptosis in children is often an isolated finding, it may occur in association with other ocular or systemic disorders. Systemic disorders include myasthenia gravis, muscular dystrophy, and botulism. Ocular disorders include mechanical ptosis secondary to lid tumors, blepharophimosis syndrome, congenital fibrosis syndrome, combined levator/superior rectus maldevelopment, and congenital or acquired 3rd nerve palsy. A small degree of ptosis is seen in Horner syndrome (Chapter 614). A complete ophthalmic and systemic examination is therefore important in the evaluation of a child with ptosis.
Ectropion, Entropion, and Epiblepharon
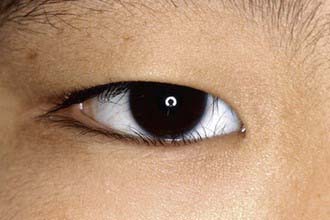
Epiblepharon is commonly seen in childhood and may be confused with entropion. In epiblepharon, a roll of skin beneath the lower eyelid lashes causes the lashes to be directed vertically and to touch the cornea (Fig. 616-1). Unlike entropion, the eyelid margin itself is not rotated toward the cornea. Epiblepharon usually resolves spontaneously. If corneal scarring begins to occur, surgical correction may be necessary.
Tumors of the Lid
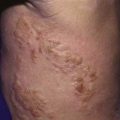
Other lid tumors arise from deeper structures (the neural, vascular, and connective tissues). Capillary hemangiomas are especially common in children (Fig. 616-2). Many tend to regress spontaneously, although they may show alarmingly rapid growth in infancy. In many cases, the best management of such hemangiomas is patient observation, allowing spontaneous regression to occur (Chapter 642). In the case of a rapidly expanding lesion, which may cause amblyopia by obstructing the visual axis or inducing astigmatism, corticosteroid, interferon, or surgical treatment should be considered. Recently, systemic propranalol has shown benefit as well. Nevus flammeus (port-wine stain), a noninvoluting hemangioma, occurs as an isolated lesion or in association with other signs of Sturge-Weber syndrome. Affected patients should be monitored for the development of glaucoma. Lymphangiomas of the lid appear as firm masses at or soon after birth and tend to enlarge slowly during the growing years. Associated conjunctival involvement, appearing as a clear, cystic, sinuous conjunctival mass, may provide a clue to the diagnosis. In some cases, there is also orbital involvement. The treatment is surgical excision.

Dray JP, Leibovitch I. Congenital ptosis and amblyopia: a retrospective study of 130 cases. J Pediatr Ophthalmol Strabismus. 2002;39:222-225.
Drolet BA, Esterly NB, Frieden IJ. Hemangiomas in children. N Engl J Med. 1999;341:173-181.
Gusek-Schneider GC, Martus P. Stimulus deprivation amblyopia in human congenital ptosis: a study of 100 patients. Strabismus. 2000;8:261-270.
Meisler DM, Raizman MB, Traboulsi EI. Oral erythromycin treatment for childhood blepharokeratitis. J AAPOS. 2000;4:379-380.
Plager DA, Snyder SK. Resolution of astigmatism after surgical resection of capillary hemangiomas in infants. Ophthalmology. 1997;104:1102-1106.
Sterker I, Grafe G. Periocular hemangiomas in childhood—functional and esthetic results. Strabismus. 2004;12:103-110.