History
The patient is a 66-year-old woman who first came to medical attention for her heart disease 3 years ago. She had been on a cruise when she initially noticed some functional limitation. She began to have difficulty climbing the stairs and found it necessary to use the elevator. By the end of the cruise she had pedal edema to the midcalf and had to sleep semirecumbant because of shortness of breath while lying flat.
On her return home, she went to see her family doctor, who ordered an echocardiogram. This showed an ejection fraction of 20%. There was trivial mitral regurgitation. The left ventricular mass index was 153 g/m2. The left ventricular end-systolic and end-diastolic dimensions were 44 and 66 mm, respectively. An electrocardiogram (ECG) demonstrated normal sinus rhythm at 77 bpm with left bundle branch block (LBBB) and left axis deviation.
She was initially treated with a diuretic (furosemide [Lasix]) and an angiotensin-converting enzyme inhibitor (ramipril). When she became euvolemic a beta blocker was added (carvedilol) and titrated up to target doses.
She underwent a coronary angiogram, which showed no evidence of flow-limiting coronary artery disease.
Her past medical history included smoking (she stopped smoking 3 years ago, after smoking one pack per day for 20 years). She had a history of breast cancer for which she was treated with chemotherapy (including doxorubicin) and radiation. She drinks 1 to 2 glasses of wine on weekend evenings. She has no family history of cardiomyopathy.
The workup for her heart failure revealed no evidence of human immunodeficiency virus, thyroid disease, hemochromatosis, or amyloidosis. She had no recent history of viral infection.
After 9 months of therapy a repeat echocardiogram was performed and showed an ejection fraction of 30%. Her symptoms had improved such that she denied any functional limitation. An exercise stress test was performed to assess her functional ability objectively. She performed a bicycle stress test and was able to perform 3.8 metabolic equivalents. This was deemed to be below expected for her age and gender.
She was referred for a biventricular implantable cardioverter-defibrillator (ICD), but she initially refused because she felt well. During the subsequent 2 years she had one hospitalization for heart failure. At that time her weight was 5 kg over her usual dry weight. She was admitted for a total of 3 days and after intravenous diuretics was back to her baseline weight and functional status.
At a recent visit to the cardiac function clinic it was recommended again that she consider a cardiac resynchronization therapy defibrillator (CRT-D). She wished to discuss it further and was referred to a cardiac electrophysiologist.
Comments
This woman is a 66-year-old woman with nonischemic (presumably chemotherapy induced) cardiomyopathy. Although she denies functional limitation, her exercise stress test demonstrates mild functional limitation (New York Heart Association class II [NYHA]).
Current Medications
The patient takes ramipril 10 mg, carvedilol 25 mg, and spironolactone 12.5 mg in the morning and carvedilol 25 mg in the evening.
Current Symptoms
The patient currently denies orthopnea and paroxysmal nocturnal dyspnea. She is now able to walk eight blocks on the flat surfaces. However, she no longer rides her bike or does aerobics and she takes the elevator instead of the stairs when at the mall.
Comments
This patient has NYHA II heart failure symptoms despite medical therapy. Often, patients will habituate to their functional limitation and feel well. They may not realize that they have changed their lifestyle to accommodate the change in their functional decline.
Physical Examination
Comments
The patient appears mildly volume overloaded.
Laboratory Data
Comments
The blood work shows renal insufficiency (a chronic problem) and mild hyperkalemia (likely from the spironolactone).
Electrocardiogram
Findings
The 12-lead ECG shows sinus rhythm at a rate of 84 bpm and LBBB (Figure 7-1).
Comments
The patient’s LBBB QRS duration is 168 msec.
Echocardiogram
Findings
The parasternal long axis shows left ventricular dilation with left ventricular end-diastolic and end-systolic dimensions of 60 and 49 mm, respectively (Figure 7-2).
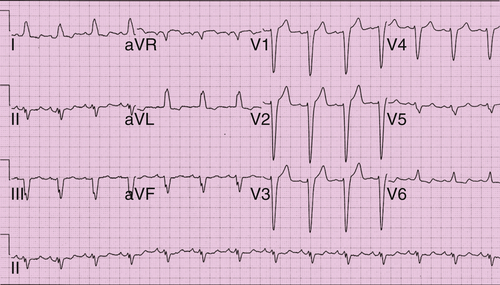
FIGURE 7-1
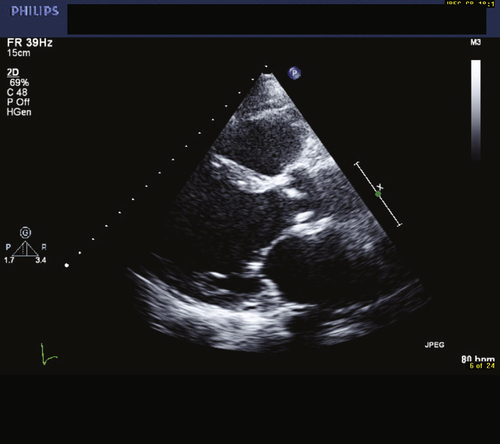
FIGURE 7-2
Comments
The left ventricle is mildly enlarged.
Findings
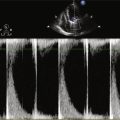
The left ventricular ejection fraction was calculated to be 22% by Simpson’s biplane method. Mild mitral regurgitation was present (Figure 7-3).
Comments
The ejection fraction is significantly reduced.
Focused Clinical Questions and Discussion Points
Question
Is there any benefit in the implantation of a biventricular pacing device in this woman?
Discussion
Both the Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) and Cardiac Resynchronization in Heart Failure (CARE-HF) trials have shown efficacy of biventricular pacing in patients with NYHA III and IV heart failure. In the COMPANION trial, Bristow and colleagues1 randomized 1520 patients with a QRS duration greater than 120 msec and an ejection fraction of less than 35% to standard medical therapy alone or in combination with a biventricular pacemaker or biventricular defibrillator. Overall, reduction in death from, or hospitalization for, heart failure by 34% in the biventricular pacemaker group and 40% in the biventricular ICD group were reported.
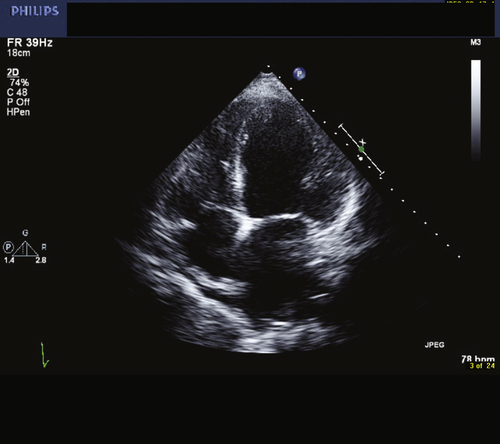
FIGURE 7-3
In CARE-HF, Cleland and colleagues2 randomized 813 patients with NYHA III and IV heart failure, an ejection fraction of 35% or less, a QRS duration of 120 msec or greater (other measures of dyssynchrony were required if the QRS duration was <150 msec), and left ventricular dilation to optimal medical therapy with or without biventricular pacing. The occurrence of death or hospitalization for a major cardiovascular event was reduced by 37% in the patients with biventricular pacing. In addition, a reduction in mortality by 36% was seen.
Both the Multicenter Automatic Defibrillator Implantation With Cardiac Resynchronization Therapy (MADIT-CRT) study and the Resynchronization–Defibrillation for Ambulatory Heart Failure Trial (RAFT) examined the efficacy of biventricular defibrillators in patients with less symptomatic heart failure.3,4 In MADIT-CRT, 1820 patients with an ejection fraction of 30% or less, a QRS of 130 msec or greater, and NYHA I or II heart failure symptoms were randomized to a biventricular ICD or ICD alone. The primary end point of death from any cause or heart-failure event occurred more frequently in the ICD alone group than the biventricular ICD group (25.3% vs. 17.2%).3
In the RAFT trial, 1798 patients with NYHA II and III heart failure, an ejection fraction of 30% or less, and a QRS of 120 msec or greater were randomized to an ICD alone or ICD plus biventricular pacing. After the mean follow-up of 40 months, the primary outcome of all-cause death or hospitalization for heart failure had occurred in 40.3% of the ICD group and 33.2% of the biventricular ICD group.
Question
Is the reduction in events with biventricular pacing seen with symptom reduction and mortality reduction or both?
Discussion
In both the MADIT-CRT trial and RAFT a reduction in heart failure in the biventricular ICD group (MADIT-CRT: relative risk reduction [RRR] = 41% in heart failure events; RAFT: RRR = 32% in heart failure hospitalizations) was seen.3,4 In RAFT, a 25% reduction in the risk for death was seen in the biventricular ICD group in contrast to the ICD alone group. However, no reduction in mortality in the biventricular ICD group in contrast to the ICD alone group was seen in the MADIT-CRT trial.
Question
Which patients with NYHA II heart failure appear to derive the most benefit from biventricular pacing? Is it expected that the patient in this case will derive benefit?
Discussion
In the MADIT-CRT trial, several prespecified subgroups were analyzed in regard to the efficacy of biventricular ICD therapy on the primary outcomes. It appeared that biventricular ICD therapy conferred a greater benefit in women than men and in patients with a QRS greater than 150 msec than in patients with a QRS less than 150 msec.3
In the RAFT trial, biventricular ICD therapy appeared to have a greater efficacy in the patients with QRS duration greater than 150 msec than in patients with a QRS duration less than 150 msec and in patients with an LBBB QRS morphology than with other morphologies.4
This patient fits the enrollment criteria for these two trials. In addition, she has an LBBB QRS morphology with a QRS of greater than 150 msec. This portends a good response to biventricular pacing. In addition, her gender would support a greater improvement with biventricular pacing.
Final Diagnosis
This patient is 66 years old and has nonischemic (presumably anthracycline induced) cardiomyopathy. She feels well but has had a heart failure admission and had functional limitation on her exercise stress test. Her ECG shows LBBB with a QRS duration of 168 msec.
Plan of Action
After a discussion with the patient regarding the risks and benefits of implantation of CRT-D or ICD, the patient wished to proceed with a CRT-D.
Intervention
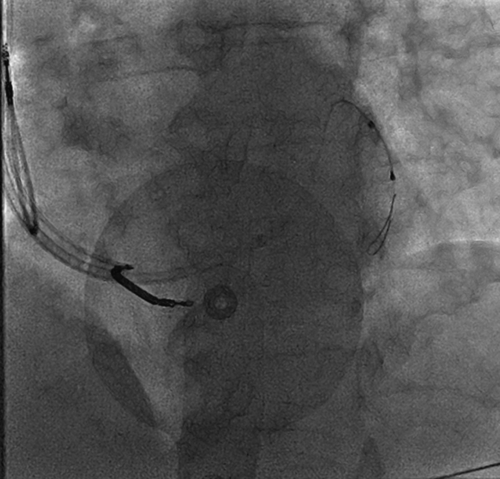
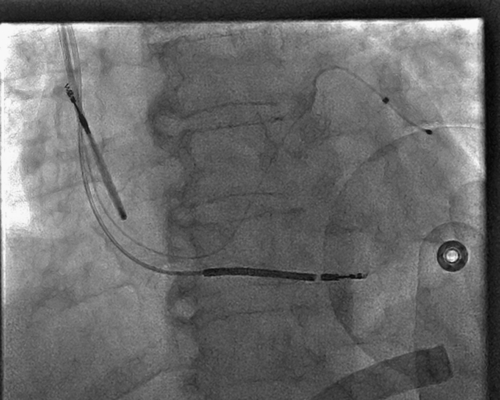
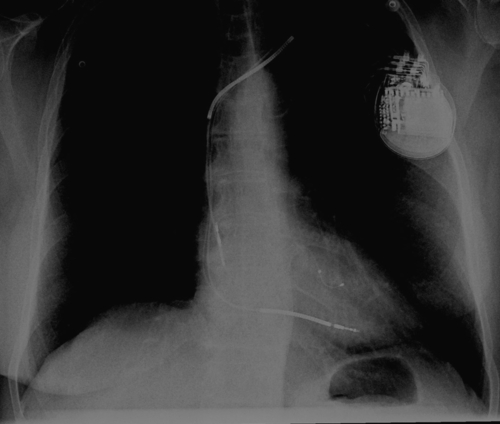
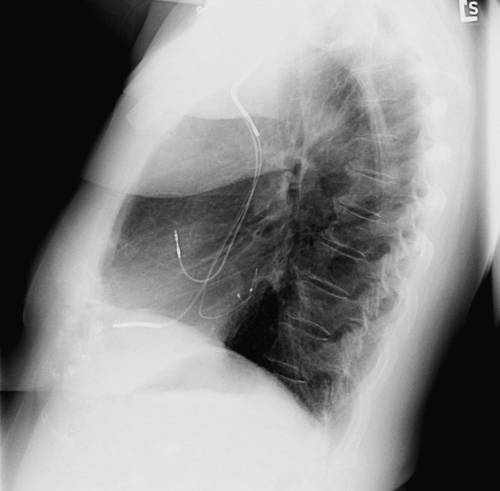
CRT-D was undertaken; the coronary sinus venogram identified a suitable posterolateral coronary sinus branch within which a left ventricular lead was inserted (Figure 7-4). Initially, the lead was inserted without the use of an angioplasty wire but could not be fully inserted (Figure 7-5). Therefore an angioplasty wire (Figure 7-6) was used to facilitate more fully advanced lead placement (Figure 7-7). The final position is identified on the posteroanterior and lateral radiographs (Figures 7-8 and 7-9).
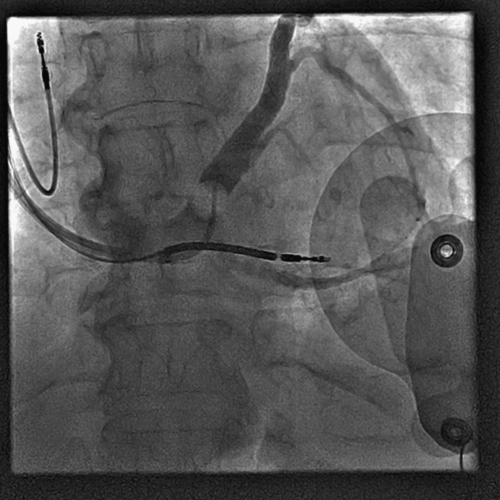
FIGURE 7-4
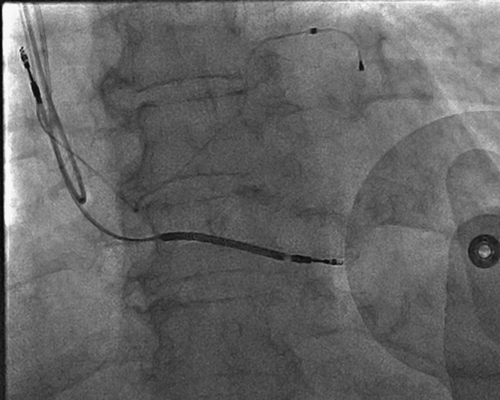
FIGURE 7-5
Selected References
1. Bristow M.R., Saxon L.A., Boehmer J. et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150.
2. Cleland J.G., Daubert J.C., Erdmann E. et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549.
3. Moss A.J., Hall W.J., Cannom D.S. et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361:1329–1338.
4. Tang A.S., Wells G.A., Talajic M. et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med. 2010;363:2385–2395.