History
Current Medications
Current Symptoms
Physical Examination
Laboratory Data
Electrocardiogram
Findings
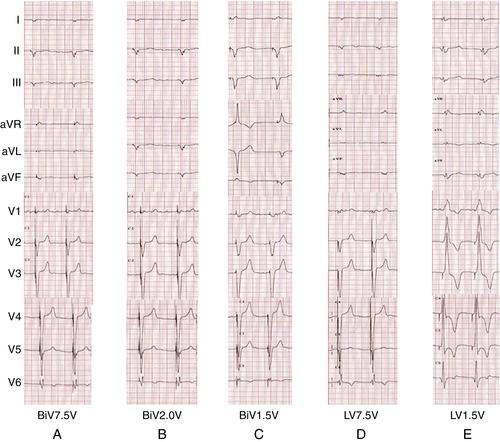
FIGURE 43-1
Focused Clinical Questions and Discussion Points
Question
Discussion
Final Diagnosis
Plan of Action
Selected References
1. Bulava A., Ansalone G., Ricci R. et al. Triple-site pacing in patients with biventricular device-incidence of the phenomenon and cardiac resynchronization benefit. J Interv Card Electrophysiol. 2004;10:37–45.
2. Champagne J., Healey J.S., Krahn A.D., ELECTION Investigators et al., et al. The effect of electronic repositioning on left ventricular pacing and phrenic nerve stimulation. Europace. 2011;13:409–415.
3. Dendy K.F., Powell B.D., Cha Y.M. et al. Anodal stimulation: an underrecognized cause of nonresponders to cardiac resynchronization therapy. Indian Pacing Electrophysiol J. 2011;11:64–72.
4. Tamborero D., Mont L., Alanis R. et al. Anodal capture in cardiac resynchronization therapy implications for device programming. Pacing Clin Electrophysiol. 2006;29:940–945.
5. Thibault B., Roy D., Guerra P.G. et al. Anodal right ventricular capture during left ventricular stimulation in CRT-implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2005;28:613–619.
6. van Gelder B.M., Bracke F.A., Meijer A. The effect of anodal stimulation on V-V timing at varying V-V intervals. Pacing Clin Electrophysiol. 2005;28:771–776.
7. Yoshida K., Seo Y., Yamasaki H. et al. Effect of triangle ventricular pacing on haemodynamics and dyssynchrony in patients with advanced heart failure: a comparison study with conventional bi-ventricular pacing therapy. Eur Heart J. 2007;28:2610–2619.



