History
Comments
Current Medications
Comments
Current Symptoms
Comments
Physical Examination
Comments
Laboratory Data
Electrocardiogram
Findings
Comments
Chest Radiograph
Findings
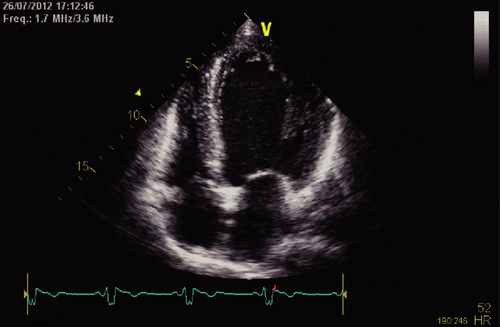
Echocardiogram
Findings
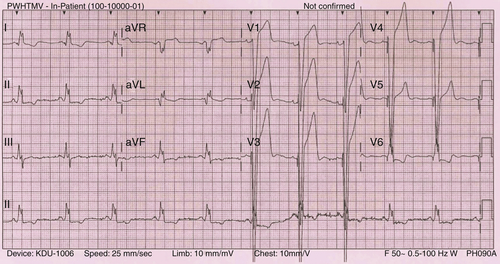
FIGURE 6-1
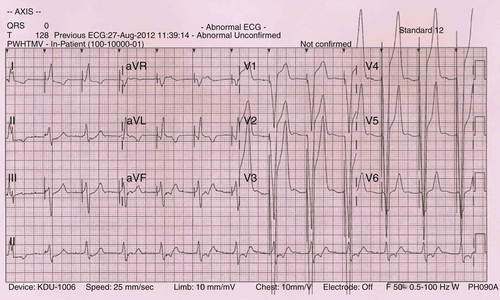
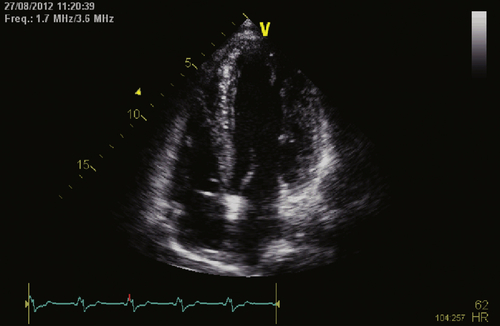
FIGURE 6-2
Findings
Focused Clinical Questions and Discussion Points
Question
Discussion
Question


Discussion
Question
Final Diagnosis
Plan of Action
Intervention
Outcome
Findings
Selected References
1. Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336:525–533.
2. Epstein A.E., DiMarco J.P. et al. American College of Cardiology/American Heart Association task force on practice guidelines (Writing committee to revise the ACC/AHA/NASPE 2002 guideline update for implantation of cardiac pacemakers and antiarrhythmia devices); American association for thoracic surgery; Society of thoracic surgeons. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities. J Am Coll Cardiol. 2008;51:e1–e62.
3. Fung J.W., Chan J.Y., Kum L.C. et al. Suboptimal medical therapy in patients with systolic heart failure is associated with less improvement by cardiac resynchronization therapy. Int J Cardiol. 2007;115:214–219.
4. Pitt B., Remme W., Zannad F. et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators. N Engl J Med. 2003;348:1309–1321.




