Procedure 37 Minimally Invasive Exposure Techniques of the Lumbar Spine
Indications
 Conditions requiring decompression of the lumbar spine, wherein a minimally invasive surgery (MIS) technique is desired
Conditions requiring decompression of the lumbar spine, wherein a minimally invasive surgery (MIS) technique is desired

Examination/Imaging
 Although it is difficult to define the exact boundaries of a percutaneous, mini-open, or traditional “open” surgery, the application of less invasive spinal surgery principles is much more important than the length of the skin incision (Jaikumar et al, 2002; Lehman et al, 2005).
Although it is difficult to define the exact boundaries of a percutaneous, mini-open, or traditional “open” surgery, the application of less invasive spinal surgery principles is much more important than the length of the skin incision (Jaikumar et al, 2002; Lehman et al, 2005).
 The most important aspect to the success of spinal surgery is proper patient selection.
The most important aspect to the success of spinal surgery is proper patient selection.



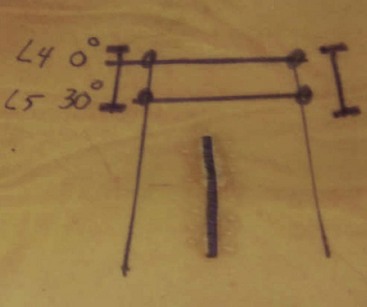
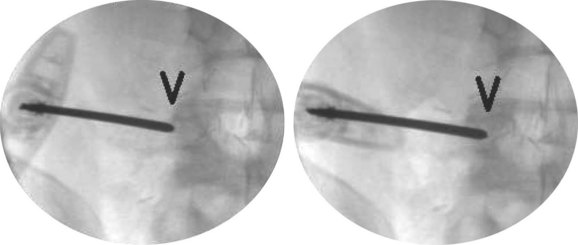
 When setting up for percutaneous pedicle instrumentation, the vertebrae should be aligned so that, on an anteroposterior (AP) image, the spinous process is centered between the pedicles, and the superior end plate is parallel to the fluoroscopy beam (the true AP view) (Figure 37-1).
When setting up for percutaneous pedicle instrumentation, the vertebrae should be aligned so that, on an anteroposterior (AP) image, the spinous process is centered between the pedicles, and the superior end plate is parallel to the fluoroscopy beam (the true AP view) (Figure 37-1).
 On the fluoroscopic lateral image, the pedicles should be superimposed, and only a single posterior cortex of the vertebral body should be seen (Figure 37-2, arrow). The edges of the superior end plate should be superimposed, forming a single radiopaque line.
On the fluoroscopic lateral image, the pedicles should be superimposed, and only a single posterior cortex of the vertebral body should be seen (Figure 37-2, arrow). The edges of the superior end plate should be superimposed, forming a single radiopaque line.


Treatment Options
• The alternative to any MIS procedure for the lumbar spine is traditional open surgery.
• With experience, MIS can be applied to essentially all degenerative conditions; however, because certain clinical situations may arise that preclude the completion of the surgery with a minimally invasive approach, the surgeon should always be prepared to extend the incision if required to adequately address the spinal pathology.
Surgical Anatomy
 The radiographic position of all relevant anatomy should be undertaken before making the initial incision.
The radiographic position of all relevant anatomy should be undertaken before making the initial incision.
 The incision should be positioned to allow optimal access to the surgical pathology.
The incision should be positioned to allow optimal access to the surgical pathology.
 The skin and fascia should be sharply divided.
The skin and fascia should be sharply divided.


 The bony landmarks should be identified before the resection of any bone.
The bony landmarks should be identified before the resection of any bone.




Surgical Anatomy Pearls
• Careful fluoroscopic localization of the surgical incision is mandatory before making the incision.
• A spinal needle inserted along the proposed trajectory of the surgical incision can be used to check the location of the incision using fluoroscopy.
• Careful palpation of surgical planes is useful before using a Kerrison instrument to remove bone from the region of the spinal canal.
Positioning
 For posterior procedures (microdiskectomy, lumbar decompression, PLF, PLIF, TLIF etc.), the patient should be positioned prone on a radiolucent spinal table or frame.
For posterior procedures (microdiskectomy, lumbar decompression, PLF, PLIF, TLIF etc.), the patient should be positioned prone on a radiolucent spinal table or frame.
 The abdomen should be free of compression (Lehman et al, 2005; Seldomridge and Phillips, 2005).
The abdomen should be free of compression (Lehman et al, 2005; Seldomridge and Phillips, 2005).
 Careful padding of all vital and bony regions should be confirmed.
Careful padding of all vital and bony regions should be confirmed.
 Access for fluoroscopy should be confirmed in the operative position.
Access for fluoroscopy should be confirmed in the operative position.



General Aspects to Posterior Tubular Retractor Surgery
 The learning curve for MIS techniques must be acknowledged and planned for.
The learning curve for MIS techniques must be acknowledged and planned for.
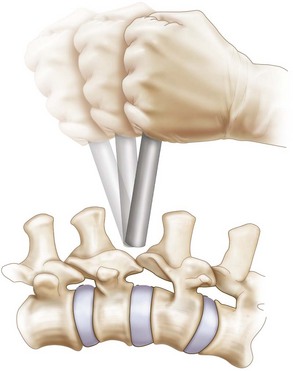
 Reconstructive procedures (Figure 37-3) are more difficult compared with decompressive procedures and should be approached farther along the learning curve of the individual surgeon. Additional time should be allotted for surgical cases in the early portion of the surgeon’s learning curve.
Reconstructive procedures (Figure 37-3) are more difficult compared with decompressive procedures and should be approached farther along the learning curve of the individual surgeon. Additional time should be allotted for surgical cases in the early portion of the surgeon’s learning curve.
 The first surgical step is to localize the precise site for all skin incisions using fluoroscopy (Seldomridge and Phillips, 2005).
The first surgical step is to localize the precise site for all skin incisions using fluoroscopy (Seldomridge and Phillips, 2005).




 In the event of a dural laceration, direct suture repair is the authors’ preferred treatment strategy for most tears (Bosacco et al, 2001). However, others have reported successful management of minor dural tears by the use of sealants without direct repair, as long as there is no tendency for nerve rootlet extravasation.
In the event of a dural laceration, direct suture repair is the authors’ preferred treatment strategy for most tears (Bosacco et al, 2001). However, others have reported successful management of minor dural tears by the use of sealants without direct repair, as long as there is no tendency for nerve rootlet extravasation.



Procedure
Step 1
 An MIS approach offers an excellent option for correcting localized spinal canal stenosis or treating herniated lumbar disks.
An MIS approach offers an excellent option for correcting localized spinal canal stenosis or treating herniated lumbar disks.



Step 1 Pearls
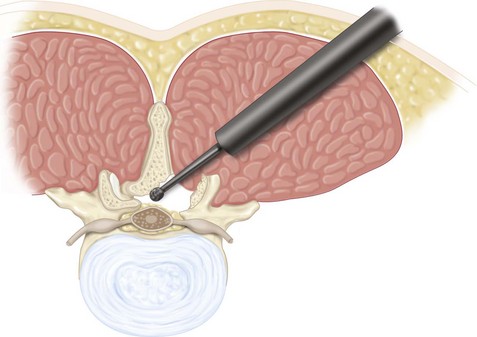
• Avoid using an overly large diameter tubular retractor for decompressive procedures, because this will push the surgeon away from the midline.
• The authors prefer to use a 14- to 18-mm diameter tube (outer diameter) for diskectomies and an 18- to 20-mm tube for stenosis decompression.
• Leave the ligamentum flavum intact during drilling of bone to protect the dura.
Step 2


 Anterior lumbar interbody fusion
Anterior lumbar interbody fusion
 Lateral transpsoas interbody fusion
Lateral transpsoas interbody fusion
Step 2 Pearls
• Penetration of the end plate during diskectomy should be avoided by the careful use of sharp instruments within the disk space.
• All cartilaginous material must be removed from the end plates to allow an optimal chance of achieving fusion.
• Avoid undersizing the interbody implants during interbody fusion, which may reduce stability of the construct and allow migration of the implant.
• Any overhanging bone that reduces the opening to the disk space should be removed to allow optimal clearance of disk material and proper sizing of the interbody implant.
Step 2 Pitfalls
• Take great care to avoid violation of the anterior annulus, which risks a major vascular injury.
• Be aware that, rarely, a conjoined nerve root may prevent safe access to the disk space when performing a TLIF or PLIF approach. In such a situation, an alternative fusion method should be undertaken.
Step 3: Instrumentation
 Minimally invasive spinal instrumentation has been simplified with the advent of percutaneous cannulated pedicle screw systems.
Minimally invasive spinal instrumentation has been simplified with the advent of percutaneous cannulated pedicle screw systems.

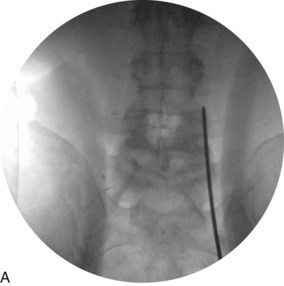
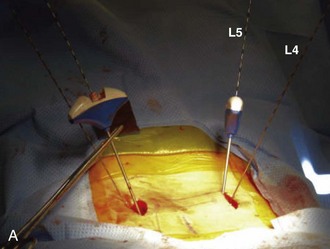
 Percutaneous pedicle screw instrumentation begins with obtaining a true AP fluoroscopic image of the vertebra (Figure 37-9, A).
Percutaneous pedicle screw instrumentation begins with obtaining a true AP fluoroscopic image of the vertebra (Figure 37-9, A).
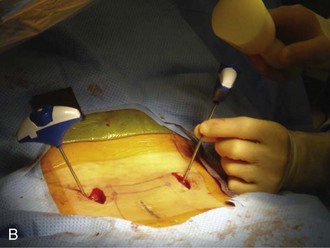
 Incisions should be localized about 1 cm lateral to the lateral margin of the pedicle visualized on the AP image (Figure 37-9, B) (Lehman et al, 2005; Seldomridge and Phillips, 2005).
Incisions should be localized about 1 cm lateral to the lateral margin of the pedicle visualized on the AP image (Figure 37-9, B) (Lehman et al, 2005; Seldomridge and Phillips, 2005).


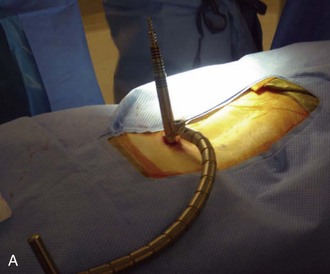
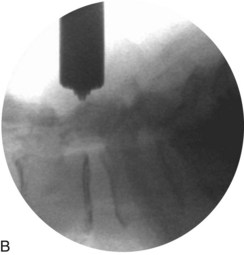
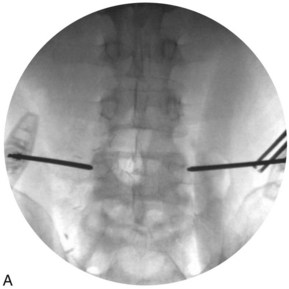
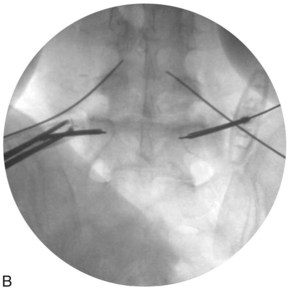
 After confirming that the tip of the needle is properly positioned (Figure 37-10, A), the tip of the needle is seated a few millimeters into the bone with gentle mallet taps (Figure 37-10, B).
After confirming that the tip of the needle is properly positioned (Figure 37-10, A), the tip of the needle is seated a few millimeters into the bone with gentle mallet taps (Figure 37-10, B).
 The position of the needle tip is again confirmed with AP fluoroscopy.
The position of the needle tip is again confirmed with AP fluoroscopy.
 Next, the needle shaft is marked 20 mm above the skin edge.
Next, the needle shaft is marked 20 mm above the skin edge.

 An AP image is again taken to assess the position of the tip of the needle, which should lie approximately
An AP image is again taken to assess the position of the tip of the needle, which should lie approximately  to
to  of the distance (from medial to lateral) across the pedicle (Figure 37-11).
of the distance (from medial to lateral) across the pedicle (Figure 37-11).
 A guidewire is inserted through the needle shaft and advanced about 15 mm into the vertebral body.
A guidewire is inserted through the needle shaft and advanced about 15 mm into the vertebral body.


 Guidewires are inserted through the Jamshidi needle (Figure 37-12, A and B).
Guidewires are inserted through the Jamshidi needle (Figure 37-12, A and B).
 Cannulated instruments, such as awls and taps, are used to prepare the pedicle for screw insertion.
Cannulated instruments, such as awls and taps, are used to prepare the pedicle for screw insertion.
 Electromyography can be used to test the tap and ensure that it has not breeched the cortex (Figure 37-13).
Electromyography can be used to test the tap and ensure that it has not breeched the cortex (Figure 37-13).
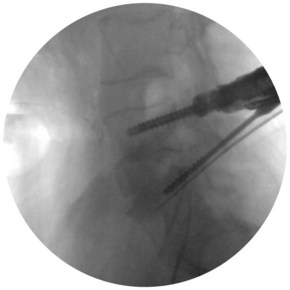
 Lateral fluoroscopy should be used to monitor the depth of instruments inserted over the guidewires (Figure 37-14).
Lateral fluoroscopy should be used to monitor the depth of instruments inserted over the guidewires (Figure 37-14).

 After tapping the pedicle holes with a cannulated tap, the cannulated pedicle screws can be placed.
After tapping the pedicle holes with a cannulated tap, the cannulated pedicle screws can be placed.
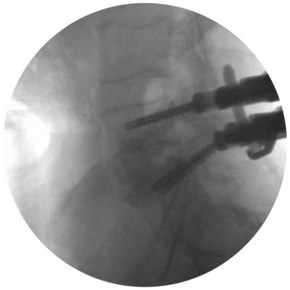
 The rod can then be introduced and locked into place (Figures 37-15 and 37-16).
The rod can then be introduced and locked into place (Figures 37-15 and 37-16).
 Final AP and lateral fluoroscopy (Figure 37-17) should confirm the fusion construct to be in an acceptable position.
Final AP and lateral fluoroscopy (Figure 37-17) should confirm the fusion construct to be in an acceptable position.
 The authors prefer to use subcuticular resorbable sutures to close the wound, resulting in a desirable cosmetic result (Figure 37-18).
The authors prefer to use subcuticular resorbable sutures to close the wound, resulting in a desirable cosmetic result (Figure 37-18).





Step 3 Pearls
• Obtaining a true AP fluoroscopic image parallel to the superior end plate of the vertebral body is paramount for the success of percutaneous screw placement.
• By marking the depth of insertion through the pedicle on the Jamshidi needle, the surgeon can safely insert the guidewires without having to switch multiple times between the AP and lateral fluoroscopy images.
Postoperative Care and Expected Outcomes




Bosacco SJ, Gardner MJ, Guille JT. Evaluation and treatment of dural tears in lumbar spine surgery: a review. Clin Orthop Relat Res. 2001;389:238-247.
German JW, Foley KT. Minimal access surgical techniques in the management of the painful lumbar motion segment. Spine. 2005;30(Suppl):S52-S59.
Jaikumar S, Kim DH, Kam AC. History of minimally invasive spine surgery. Neurosurgery. 2002;51(Suppl):S1-14.
Khoo LT, Palmer S, Laich DT, Fessler AG. Minimally invasive percutaneous posterior lumbar interbody fusion. Neurosurgery. 2002;51(Suppl):S166-S171.
Lehman RA, Vaccaro AR, Bartagnoli R, Kuklo TR. Standard and minimally invasive approaches to the spine. Orthop Clin North Am. 2005;36:281-292.
Seldomridge JA, Phillips FM. Minimally invasive spine surgery. Am J Orthop. 2005;34:224-232.
Tafazal SI, Sell PJ. Incidental durotomy in lumbar spine surgery: incidence and management. Eur Spine J. 2004;14:287-290.
Wu RH, Fraser JF, Härtl R. Minimal access versus open transforaminal lumbar interbody fusion: meta-analysis of fusion rates. Spine. 2010;35:2273-2281.


