CHAPTER 29. Hematological Care
Wanda Rodriguez
OBJECTIVES
At the conclusion of this chapter, the reader will be able to:
1. Describe normal and abnormal laboratory values and initiate appropriate nursing interventions as needed.
2. Describe the nursing care of a patient with a hematological disorder.
3. Describe the nursing interventions for a patient with a disorder in hemostasis.
4. Describe nursing responsibilities associated with blood and blood component transfusions.
5. Identify the types of transfusion reactions and the appropriate nursing interventions.
I. OVERVIEW
A. Common blood dyscrasias in the following areas:
1. Hematology
2. Hemostasis
B. Chapter broadly presents:
1. Clinical signs
2. Laboratory results
3. Nursing interventions
II. PERIANESTHESIA ISSUES RELATE TO HEMATOLOGY
A. Preoperative clinical assessment with laboratory tests
1. Alterations affect outcomes, especially oxygenation and hemostasis.
a. Critically assess potential for:
(1) Anemia
(2) Coagulopathy
b. Review clinical indications and medical history.
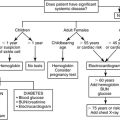
c. No established minimum value for presurgical hemoglobin (Hgb)
d. Routine laboratory screening is neither required nor recommended for every preoperative patient.
(1) When preoperative Hgb low, continue with surgery as planned depending on:
(a) Acuity of anemia
(b) Patient’s cardiopulmonary response
(c) Surgical urgency
e. Preoperative hemoglobin selectively recommended for:
(1) Neonates to detect physiological anemia
(2) Elderly patients
(3) Menstruating women
(4) Bone marrow suppression
(5) Malignancy
(6) Genetically determined anemic conditions
f. Preanesthetic screening may uncover unrecognized coagulopathy.
(1) Documented coagulation disorder seldom appropriate for surgery in the nonacute ambulatory setting.
2. American Society of Anesthesiologists (ASA) “Practice Guidelines for Perioperative Blood Transfusion and Adjuvant Therapies”
a. Preoperative intervention recommendations
(1) Discontinue anticoagulation in advance of surgery.
(2) Delay surgery in elective cases until drug effects (e.g., warfarin, clopidogrel, aspirin) dissipate.
B. Transfusion is not innocuous; there are potential risks.
1. Complications cannot be overlooked or minimized.
a. Hemolytic reactions (Refer to section V, subsection C.)
b. Transfusion-related acute lung injury
(1) Occurs usually within 2 hours of beginning of transfusion or appears within 6 hours
(2) Food and Drug Administration (FDA) reporting indicates leading cause of transfusion-related fatality
(3) In-hospital mortality rate: 5% to 10%
(4) Causes
(a) Antibodies in plasma against human white blood cell antigen lead to immune-mediated response.
(b) Lipid inflammatory agents mediate granulocyte antigens.
(5) Signs and symptoms
(a) Acute dyspnea
(b) Noncardiogenic pulmonary edema
(c) Frothy sputum
(d) Diffuse bilateral infiltrates
(e) Crackles
(f) Fever
(g) Tachycardia
(h) Hypotension
(6) Treatment
(a) Stop transfusion.
(b) Administer oxygen.
(c) Intubate.
(d) Place on mechanical ventilation.
(e) Hypotension not responding to fluids, administer vasopressors.
(f) Involves noncardiogenic pulmonary edema
(g) No diuretics as can worsen the situation
(h) Nonsteroidal anti-inflammatory drugs (NSAIDs)
(i) Prostaglandins
c. Transfusion transmitted
(1) Human immunodeficiency virus (HIV)
(2) Cytomegalovirus (CMV)
(a) Carried by 70% of donors
(3) Viral infections such as hepatitis
(a) Hepatitis not detected by donor testing: long “seronegative” period; most (>90%) transmitted hepatitis is hepatitis C.
(4) Especially threatening to the immunosuppressed
(a) Occurs 3 to 6 weeks post transfusion of large amounts of fresh blood
(5) Bacterial contamination: in blood bank
(a) Stored units can cause severe septicemia.
(b) Mortality nearly 60% because of endotoxins producing gram-negative organisms
(c) FDA reporting indicates third most common cause of transfusion- related fatality
d. Transfusion-related immunomodulation
(1) Immunosuppression occurs after transfusion.
(2) May cause reactivation of latent viruses such as CMV
(3) Causal relationship not proven but linked in recurrence of:
(a) Resected malignancies (especially colorectal cancer)
(b) Inflammatory bowel disease
(c) Spontaneous abortions
(4) Associated in development of postoperative infections
(5) Leukocyte-depleted transfusions suggested as an alternative
2. Weigh against serious anemia risk: oxygen deficit, decreased perfusion
a. If mild:
(1) Palpitations
(2) Tachycardia
(3) New ejection murmur
b. If severe:
(1) Stroke
(2) Myocardial infarction
c. ASA “Practice Guidelines for Perioperative Blood Transfusion and Adjuvant Therapies”
(1) Intraoperative and postoperative management recommendations
(a) “Red blood cells should usually be administered when the hemoglobin level is low (e.g., less than 6 g/dL in a young healthy patient), especially when anemia is acute.”
(b) “Red blood cells are usually unnecessary when the level is more than 10 g/dL.”
(c) “These conclusions may be altered in the presence of:
(i) Anticipated blood loss.
(ii) Active critical (i.e., myocardium, central nervous system, or renal) organ ischemia.”
(2) “The determination of whether intermediate Hgb concentrations (i.e., 6-10 g/dL) justify or require red blood cell transfusion should be based on:
(a) Any ongoing indication of organ ischemia
(b) Potential or actual ongoing bleeding (rate and magnitude)
(c) The patient’s intravascular volume status
(d) The patient’s risk factors for complications of inadequate oxygenation.”
(3) “These risk factors include a:
(a) Low cardiopulmonary reserve
(b) High oxygen consumption.”
3. Metabolic effects of stored blood: a 35- to 42-day “shelf life”
a. Toxic enzymes from dead white blood cells (WBCs) and platelets “significant” after 14 days of storage
b. Hypocalcemia: ionized calcium binds with citrate used to preserve stored blood.
c. Aging blood results in:
(1) Hyperkalemia: potassium released from cell lysis
(2) Acidosis
(3) Independent risk factors for multiple organ failure
d. Postoperative infection and immunosuppression risk
(1) May not be evident for months posttransfusion
(2) After spinal fusion, joint replacement, transfusion associated with iatrogenic wound infection, longer hospital stay, and more days of fever, antibiotic therapy
(3) Tumor recurrence linked to transfusion, unproven
C. Autologous transfusion: alternative to allogenic transfusion
1. Preoperative autologous donation. Patient predonates units of own blood.
a. Patients may be ineligible for presurgical donation because of:
(1) Weight
(2) Age
(3) Restrictions
(4) Anemia
(5) Cardiac conditions
b. Advantages
(1) Prevention of disease transmission
(2) Some adverse transfusion reactions
(3) Reassurance about blood risks
c. Disadvantages
(1) Higher cost
(2) Wastage of unused blood
(3) Potential for clerical error
(4) Likelihood of requiring transfusion due to risk of perioperative anemia
2. Reinfusion of salvaged blood intraoperatively or postoperatively
a. Recovered red blood cells (RBCs) have oxygen transport properties equivalent to allogenic transfusions.
b. As long as the salvaged blood stays connected with the patient’s circulation, intraoperative blood salvage is often acceptable to Jehovah’s Witnesses.
3. Acute normovolemic hemodilution
a. Removal of patient’s blood and restoring intravascular volume with:
(1) Crystalloid
(2) Colloid
b. Done before start of the operative procedure after induction
c. Dilution of patient’s blood reduces RBC losses, when blood is lost during surgery.
d. Reinfusion can occur at any time during or after surgery.
D. Alternatives to allogenic transfusions
1. Epoetin alfa (recombinant human erythropoietin)
a. Stimulates erythropoiesis in the bone marrow
b. Frequently used in:
(1) Cancer-related anemia
(2) Anemia with renal insufficiency
(3) Anemia in the critically ill
c. Products: Epogen or Procrit
2. Antifibrinolytic agents
a. Blood loss reduction after surgery, especially cardiac, and in trauma
b. Products
(1) Aprotinin (Trasylol)
(2) Aminocaproic acid (Amicar)
(3) Tranexamic acid (Cyklokapron)
c. FDA issued a Public Health Advisory for aprotinin.
(1) Adverse effects
(a) Myocardial infarction
(b) Stroke
(c) Renal dysfunction
E. Bloodless medicine programs
1. Team approach in providing best medical care to all patients using alternative to allogenic transfusions
2. Advocating for patients who do not accept transfusions (e.g., Jehovah’s Witness)
III. HEMATOLOGY COMPONENTS: BLOOD CELLS AND CLOTTING FACTORS
A. Hemoglobin: carried on RBCs
1. RBC physiology (Box 29-1)
a. Critical transporter of oxygen to tissues
(1) Carried on hemoglobin molecule to tissues
(2) Normally concave on both sides (biconcave)
(3) Proportion (percentage) in total blood volume is hematocrit.
b. Produced in bone marrow and removed by the spleen
c. Production stimulated by erythropoietin, which is produced by the kidney
d. Life span approximately 120 days
BOX 29-1
HEMATOLOGY: NORMAL LABORATORY VALUES*
Red blood cells (RBCs)
▪ Male: 4.6-6.2 million per microliter
▪ Female: 4.2-5.4 million per microliter
Hemoglobin (Hgb)
▪ Male: 13-18 grams per deciliter (g/dL)
▪ Female: 12-16 g/dL
Hematocrit (HCT): proportion of RBCs in circulating blood volume
▪ Male: 40%-54%
▪ Female: 37%-47%
White blood cells (WBCs): 4500-11,000 per microliter
Differential:
▪ Segmented neutrophils: 54%-62%
▪ Band neutrophils: 3%-5%
▪ Lymphocytes: 25%-33%
▪ Monocytes: 3%-7%
▪ Eosinophils: 1%-3%
▪ Basophils: 0-1%
Platelets: 150,000-400,000 per microliter
Prothrombin time (PT): 12-14 seconds
Usually expressed as International Normalized Ratio (INR): 0.7-1.8
Activated partial thromboplastin time (APTT): 30-40 seconds
Partial Prothrombin time (PTT): 25-41 seconds
Fibrinogen level: 200-400 mg/100 mL
Thrombin time (TT): 14-16 seconds
Fibrin degradation (split) products: 2-10 mcg/mL
D-dimer <250 ng/mL
*Guidelines only: normal values vary with clinical laboratory.
2. Anemia: hemoglobin or RBC deficit; hematocrit reduction
a. Cardiovascular symptoms vary with hemoglobin level and acuity of cell loss: weakness and fatigue common.
b. Assess and suspect acutely low hemoglobin if:
(1) Low oxygen saturation as measured by pulse oximetry (Sp o 2), particularly if intraoperative blood loss was significant
(2) Hypotension, perhaps noted by orthostatic changes when head of bed raised or ambulatory surgery patient stands
(3) Tachycardia, likely a compensatory way to sustain cardiac output and sustain normal blood pressure
(a) A multipurpose indicator representing a response by sympathetic nerves of the autonomic system
(b) Consider hypovolemia.
(i) With or without low hemoglobin
(ii) Heart rate increases
(c) Heart rate increased with:
(i) Stress
(ii) Anxiety
(iii) Fever
(d) Patients who cannot respond with tachycardia
(i) Patients taking beta-blocker medications
(ii) Patients with transplanted hearts, which are denervated and so lack autonomic responses
c. Causes of hemoglobin deficit
(1) Loss
(a) Hemorrhagic: usually acute as in:
(i) Trauma
(ii) Surgical loss
(iii) Gastrointestinal
(iv) Uterine
(v) Nasal
(vi) Vascular
(b) Hemodilution from fluid volume expansion
(i) Normal during pregnancy
(ii) Replacement with non-RBC colloid or crystalloids
(c) Researchers implicate laboratory draws (phlebotomy) as source of accumulated blood loss, especially for intensive care unit patients: up to 40 to 70 mL daily.
(2) Inadequate RBC production
(a) Insufficient vitamin B 12 (intrinsic factor) needed for erythropoiesis
(i) Postgastrectomy: insufficient hydrochloric acid secretion along with atrophy of gastric parietal cells
(ii) Pernicious anemia: autoimmune destruction and atrophy of the gastric parietal cells along with insufficient hydrochloric acid secretion
(b) Endocrine factors: insufficient erythropoietin production, as in:
(i) Chronic renal failure
(ii) Addison’s disease
(iii) Thyroid diseases
(c) Liver disease: drug or alcoholic induced
(d) Aplasia: bone marrow suppression
(i) Decreased
[a] Hemoglobin
[b] RBCs
[c] WBCs
[d] Platelet count
(ii) Etiology
[a] Malignancy: infiltration of marrow
[b] Chemotherapy
[c] Chemical or radiation exposure: dose dependent
[d] Medications: phenytoin, chloramphenicol
(e) Inflammatory conditions
(i) Rheumatoid arthritis
(ii) Autoimmune diseases such as lupus erythematosus
(iii) About 15% of asymptomatic HIV-positive patients are anemic.
(f) Genetic predisposition: mutation or recessive traits
(i) Alters a link in the chain of hemoglobin formation
(ii) Produces hemolytic anemias such as:
[a] Sickle cell anemia (Box 29-2)
[1] Affects 1% of African Americans
[2] Hypoxia, fever, acidosis spur RBC change from biconcave to sickled.
[3] Severe pain: joints, limbs, abdomen
[4] Jaundice, ischemia, organ infarction
BOX 29-2
SICKLE CELL ANEMIA: PREDISPOSED BY HEREDITY
Genetic Characteristics
Most commonly, patients inherit the HbS trait from both parents.
Specific stimuli cause RBCs to alter shape and function.
Forms mutant HbS rather than normal HbA
Trait carried by 10% of African Americans
Fewer than 1% of African Americans develop disease.
Clinical Concerns
Abnormal HbS cell forms have decreased affinity for oxygen.
Oxygen deficit causes cells to change shape and sickle.
Sickled cells rupture or clog small vessels.
Sickling crisis stimulated by:
▪ Altered temperature: fever or cold
▪ Acidosis and hypoventilation
▪ Dehydration
▪ Changes in altitude
Clinical Outcomes
Chronic anemia one of the hallmark clinical signs and exacerbations
Sluggish peripheral circulation due to sludging or vaso-occlusion
▪ Thrombosis, organ infarction
▪ Cerebral changes, altered renal function, cardiopulmonary compromise
▪ Limb ulcerations, necrosis
Ischemic pain, especially at limbs, joints, bones, and abdomen
Infection susceptibility
Nursing Responsibility: Crisis Prevention and Anemia Management
Ensure oxygenation: Prevent hypoventilation, acidosis.
▪ Monitor respiratory quality, rate, and depth.
▪ Provide supplemental oxygen; titrate to oxygen saturation.
▪ Adequately reverse muscle relaxants.
▪ Position patient for effective lung expansion.
▪ Early mobility
Promote peripheral circulation: minimize vasoconstriction.
▪ Maintain normothermia.
▪ Ensure adequate hydration to reduce blood viscosity.
▪ Regularly assess limb, organ ischemia.
▪ Limit peripheral blood stagnation.
▪ Monitor renal labs, urine volume.
Reduce stress.
▪ Analgesia: manage pain.
▪ Antibiotics: prevent or control infection.
▪ Calming environment
Avoid if possible vasodilators—may cause hypotension
Avoid if possible vasoconstrictors—may cause circulatory stasis
Other therapies
▪ Transfusions
▪ Hydroxyurea
▪ Cytotoxic agent that can elevate HbF levels, decreasing HbS formation
HbA, Hemoglobin A (adult hemoglobin); HbF, hemoglobin F (fetal hemoglobin); HbS, hemoglobin S (sickle cell hemoglobin); RBCs, red blood cells.
[b] Thalassemia (Cooley’s)
[1] Major: early death, altered growth, transfusion dependency
[2] Minor (trait): few symptoms, hemoglobin <12 g/dL
[c] Spherocytosis
[1] RBCs spherical rather than biconcave disks; survival reduced to 14 days
(3) Destruction of RBCs: normal vitamin B 12 levels
(a) Pharmaceuticals, burns: destroys or impairs function
(b) Excessive physical stress
(c) Hemolysis: cell trauma, destruction, or consumption
(i) Defective prosthetic heart valves or blood pumps
(ii) Infection: bacterial or viral
(4) Inadequate intake of folic acid or iron
(a) Malnutrition: dietary lack, alcoholism, chronic anorexia
(b) Malabsorption as a result of ileal disease, surgical resection
d. Perianesthesia nursing interventions and evaluation related to anemia
(1) Need sufficient RBC numbers and hemoglobin level to bind oxygen for delivery to tissues
(2) No absolute minimum hemoglobin measure established, although acute loss may cause more hemodynamic instability than chronic deficit
(a) Hemoglobin of 9 to 10 g/dL is desired.
(b) Anesthesia may be safely administered to patients with hemoglobin of 6 to 7 g/dL, such as:
(i) Patients with chronic renal failure whose erythropoietin is suppressed
(ii) Acutely ill Jehovah’s Witnesses who refuse blood on religious principles
(c) Acute anemia is unlikely in ambulatory surgery setting.
(3) Fully saturate circulating hemoglobin.
(a) Monitor oxygen saturation, ensure adequate oxygenation, limit oxygen demand.
(i) Stimulate the sedated patient.
(ii) Position the patient for optimal lung expansion.
(iii) Deliver supplemental oxygen by mask or nasal cannula, with or without humidity.
(iv) Provide analgesia to promote deep breathing.
(v) Reduce stress: provide anxiolytics if safe.
(vi) Remember that hypoxia alters acid-base balance.
(b) Measure hemoglobin.
(i) Particularly if oxygen saturation decreases
(ii) Monitor postoperative blood and volume losses from drains, dressings, suction.
(iii) Prevent profound hypotension.
[a] Increase preload (volume) and support cardiac output: hydrate with crystalloid, colloid if necessary.
[b] Anticipate orthostatic effects: gradual position changes to upright, noting blood pressure and heart rate.
[c] Transfuse if ordered by physician per facility protocol.
3. Polycythemia: exaggerated RBC, hemoglobin, hematocrit, WBC production
a. Increased RBC production unrelated to erythropoietin level
(1) Blood volume and viscosity profoundly increased: cause unknown
(2) Hypertension, vein engorgement, cardiac arrhythmia, thrombosis, tissue hypoxia can result.
(3) One form (polycythemia vera) occurs in adults older than 60 years, primarily men.
(a) Erythropoietin level low
b. Physiological response by bone marrow as:
(1) Adaptive response to altitude: normal compensation to environment
(2) Pharmaceutical response to parenteral erythropoietin given to patients with chronic renal failure
(3) Compensatory response to “perceived” hypoxemia associated with chronic cardiopulmonary conditions
(a) Valvular or structural cardiac anomalies impede cardiac outflow and therefore oxygen delivery to tissue.
(b) Pulmonary obstructive diseases such as asthma, emphysema
(c) Pulmonary hypertension, pheochromocytoma
c. Assessment, intervention, evaluation
(1) Laboratory tests: hemoglobin >18 g/dL, hematocrit >54%, RBCs, WBCs, platelet count elevated
(2) Symptoms: ruddy complexion, headache, weakness, angina, palpitations, hypertension, splenomegaly, claudication, phlebitis
(3) Treatment: chronic anticoagulation, splenectomy, phlebotomy
B. Leukocytes: WBCs
1. Physiology: mediate immune response with assorted WBC cell types
a. Primary functions
(1) Neutrophils—phagocytosis
(2) Lymphocytes—antibody production and cell-mediated immunity
(3) Monocytes—phagocytosis and antibody production,
(4) Eosinophils and basophils—allergic hypersensitivity reactions
2. Leukocytosis: increased WBC production up to 100,000 per microliter and anemia
a. Appropriate inflammatory response to “invasion” by foreign substances or infection
b. Pathological response: bone marrow proliferation, elementary WBCs
(1) Acute lymphocytic leukemia
(a) More common in children, with:
(i) Pain
(ii) Fatigue
(iii) Bleeding
(iv) Enlarged lymph nodes
(v) Enlarged liver
(vi) Enlarged spleen
(vii) History of fever with no apparent cause
(b) Cure rate in children is 80%.
(c) Treatment: eradicate leukemic cells from marrow, lymph tissue, and/or residual disease from central nervous system.
(i) Chemotherapy
(ii) Targeted drug therapy
(iii) Radiation therapy
(iv) Bone marrow–stem cell transplantation
(2) Chronic lymphocytic leukemia
(a) Affects men older than 50 years with enlarged spleen and neck lymph nodes
(b) Symptoms may develop slowly due to the abnormal cells increasing at slower rate.
(c) Treatment: alleviate symptoms and slow down progression.
(i) Chemotherapy, stem cell transplantation, and/or radiation for palliative care
(3) Acute myelocytic leukemia
(a) Characterizes 80% of all adult leukemias
(b) Produces fever, bruising, pallor, joint pain, fatigue, enlarged liver, spleen
(c) Treatment: eradicate leukemic stem cell.
(i) Chemotherapy, immunotherapy, bone marrow transplant, and/or radiation therapy
(4) Hodgkin’s disease (Hodgkin’s lymphoma)
(a) Originates with enlarged lymph nodes, starting at neck, axilla
(b) Common in early adulthood between the ages of 20 and 40 years with fever, night sweats, weight loss, fatigue, liver and spleen enlargement
(c) Symptoms will manifest anywhere in the body depending on the location.
(d) Treatment: combined chemotherapy and radiotherapy
(5) Non-Hodgkin’s lymphomas
(a) Large group of cancers that originate in the lymphatic system
(b) Two classifications
(i) Indolent: grow slowly and fewer symptoms
[a] Diffuse large B-cell lymphoma, follicular lymphoma
(ii) Aggressive
[a] Burkitt’s lymphoma, diffuse small non–cleaved cell lymphoma
(c) Swollen lymph nodes, neck, axilla, or groin, fever, night sweats, abdominal pain or swelling
(d) Treatment: different therapies and approaches for indolent (low or high tumor burden) and aggressive
(i) Indolent
[a] Low tumor burden: radiotherapy and/or combined with chemotherapy
[b] High tumor burden: biology-based therapies (e.g., monoclonal antibodies, interferon, or vaccines)
(ii) Aggressive
[a] Early: chemotherapy combined with radiotherapy
[b] Recurrent: high-dose chemotherapy and bone marrow or stem cell transplantation
(6) Multiple myeloma
(a) Malignancy of the plasma cell that produces immunoglobulin
(b) Affects adults older than 70 years with bone pain, fractures, bleeding, and bruising
(c) Common in men and in African Americans
(d) Treatment: alleviate symptoms and slow down progression.
(i) High-dose chemotherapy with stem cell transplantation
(ii) Corticosteroids alone or with other drugs such as:
[a] Thalidomide
[b] Lenalidomide (Revlimid)
[c] Bortezomib (Velcade)
c. Perianesthesia interventions and evaluation
(1) Increase oxygen delivery with supplemental oxygen.
(2) Prevent tissue damage, bruising.
(a) Use soft-tipped suction catheters.
(b) Position gently; pad stretcher siderails if indicated.
(c) Apply pressure; monitor venous, arterial puncture sites.
(3) Transfuse blood components as ordered.
(4) Prevent infection: respect protective isolation precautions when WBC, platelets dangerously low.
(a) Provide post anesthesia care unit (PACU) care in operating room or patient’s room per hospital policy rather than PACU.
3. Leukopenia: production reduced to fewer than 5000 per microliter of blood
a. Bone marrow suppression by:
(1) Disease
(2) Immunosuppression
(3) Radiation
(4) Toxins
(5) Drugs
b. Patient safety may require protective isolation to prevent exposure to iatrogenic infection.
4. Perianesthesia nursing assessments and interventions
a. Report deviation from normal parameters.
(1) Preadmission tests might be first recognition of infection or leukemia.
(2) Leukopenia and unusual bruising may coexist with anemias and platelet dysfunction.
b. Obtain accurate history: ask pointed preanesthetic questions.
(1) Fevers, with or without chills?
(2) Easy bruising or bleeding?
(3) Increased fatigue?
(4) Pain, especially in joints?
c. Think “protection.”
(1) Avoid pressure to skin and joints, and provide soft surfaces against skin.
(2) Prevent hematoma during venipuncture and suctioning.
(3) Isolate as required: infectious versus protective.
IV. COAGULATION: A CHAIN OF EVENTS TO ENSURE HEMOSTASIS
A. Physiology: clotting is an intricate balance that requires:
1. Adequate liver function to produce a cascade of interrelated clotting factors that circulate until activated
2. Functional platelets, normal calcium, and specific enzymes
a. Platelets “plug” injury site.
b. About 66% circulate for their 7- to 10-day life span, rest in spleen.
c. Aspirin renders platelets less “sticky.”
3. Vascular integrity ensures a smooth, “healthy” endothelial wall for:
a. Adherence of a platelet plug bound by a fibrin clot
b. Appropriate local constriction to limit local blood flow
4. Synergy among a host of clotting factors (proteins) along the coagulation pathway
a. Coagulation factors (Box 29-3)
(1) Vitamin K–dependent factors are factors II, VII, IX, and X.
(2) Platelets affect factor XIII.
BOX 29-3
CLOTTING FACTORS*
| Factor I | Fibrinogen |
| Factor II | Prothrombin |
| Factor III | Tissue thromboplastin |
| Factor IV | Calcium ions |
| Factor V | Proaccelerin |
| Factor VII | Prothrombin conversion accelerator |
| Factor VIII | Antihemophilic factor A/von Willebrand factor |
| Factor IX | Christmas factor (autoprothrombin II) |
| Factor X | Stuart factor (autoprothrombin I) |
| Factor XI | Plasma thromboplastin antecedent |
| Factor XII | Hageman factor (enzyme) |
| Factor XIII | Fibrin-stabilizing factor |
b. Naturally occurring coagulation inhibitors include:
(1) Alpha-1 antitrypsin
(2) Protein C
(3) Antithrombin 3
c. Clotting pathways (Table 29-1)
(1) Extrinsic pathway: triggered by tissue injury; thromboplastin released and a sequence of events leading to fibrin clot formation
(2) Intrinsic pathway: occurs within blood; proenzyme (factor VII) activated, spurs a cascade of clotting factors
| Extrinsic | Intrinsic | |
|---|---|---|
| Response | Tissue | Within blood |
| Activates | Thromboplastin (factor III) | Circulating clotting factors and platelets |
| Result |
Prothrombin (made in liver) converted to thrombin via plasma proteins, enzymes, and clotting factors
Fibrin forms from thrombin
|
Platelets aggregate, form plug |
| Laboratory tests | PT and INR | PTT |
d. Fibrin
(1) Strands of structural support for platelet plug; formed when fibrinogen activated
(2) Effect limited to injury site to prevent massive coagulation
B. Laboratory assessments of coagulation (see Box 29-1)
1. Prothrombin time (PT): assesses conversion of prothrombin to thrombin and factors I, II, V, VII, and X
a. Specific monitor for Warfarin (Coumadin), which affects the external coagulation pathway
b. If prolonged: significant bleeding risk during surgery, trauma, or soft tissue injury and must correct preprocedure
(1) Liver disease, vitamin K deficiency
(2) Fibrinogen; prothrombin; clotting factors V, VII, X
c. Clinical interventions to correct abnormal lab values
(1) Vitamin K injections
(2) Fresh frozen plasma
2. International normalized ratio (INR): standardized method of reporting the PT
a. Used to monitor Warfarin (Coumadin)
3. Partial thromboplastin time (PTT): assesses intrinsic coagulation pathway
a. Monitor if administering heparin.
b. Detects alteration in clotting factors I, II, V, VIII, IX through XII
4. Thrombin time (TT): assesses thrombin activity to stimulate fibrin creation at coagulation’s final stage
a. Prolonged by fibrinogen (factor I) deficiency
5. Platelet count: number, shape, and size of circulating platelets
a. Surgical bleeding is rare if numbers are 100,000 or greater.
b. Anticipate spontaneous bleeding if platelet numbers <20,000.
c. Aspirin alters function for the 7-day life of a platelet.
d. NSAIDs alter platelet function, with recovery within 2 days.
C. Coagulopathies: acquired or hereditary disorders of clotting sequence
1. Idiopathic immune thrombocytopenic purpura (ITP): characterized by spontaneous bleeding
a. Autoimmune disorder: active antiplatelet antibodies and profoundly reduced platelet numbers, causing epistaxis, petechiae, bruising
b. Acutely affects young children after immunization or viral infection with chicken pox, mumps, or measles
c. Chronic ITP affects adults, primarily women, younger than 50 years.
d. Treatment: depends on severity
(1) In children: no treatment; may go away on its own within 6 months
(2) In adults: no treatment for mild to moderate with no bleeding
(3) Modalities: corticosteroids, intravenous immunoglobin, or splenectomy
2. Disseminated intravascular coagulopathy (DIC): clotting factor consumption in response to surgery, pregnancy toxemia, sepsis, cancer, trauma, or multiple transfusions
a. Simultaneous active bleeding and intravascular (capillary) clotting
(1) Prolonged
(a) PT
(b) PTT
(c) INR
(d) TT
(2) Decreased
(a) Platelets
(b) Fibrinogen
(3) Increased
(a) Fibrin degradation (split) products (degree of fibrinolysis)
(b) D-dimer (breakdown of fibrin)
b. Reflects severe, overwhelming response to organ system crisis
c. Treatment focus is replacing clotting factors and correcting imbalances.
(1) Administer blood and coagulation factors as ordered.
(2) Administer volume resuscitation and, if indicated for refractory shock, inotropes as ordered.
d. Occurrence in ambulatory surgery setting is highly unlikely.
3. Hereditary coagulopathies
a. Hemophilia: sex-linked clotting factor deficiency affecting men
(1) Hemophilia A: clotting factor VIII lacking
(a) Significant bleeding into tissues and joints if active factor VIII is <5%
(b) PTT prolonged and PT normal
(2) Hemophilia B (Christmas disease): clotting factor IX lacking
(a) Prevents formation of stable clots; regular infusions of cryoprecipitate or fresh frozen plasma (FFP) likely
(b) Intraoperative FFP needed to support factor IX
(c) PTT, PT, and TT all within normal limits
(3) Drug approved for use of bleeding, prophylaxis: NovoSeven (recombinant factor VIIa product)
(a) No human plasma used in its manufacture, nor stabilized with albumin
(b) Risk of transmission of human virus essentially zero
b. Von Willebrand’s disease: common disorder affecting men and women with mucous membrane bleeding, epistaxis, mild bruising
(1) Defective von Willebrand factor (vWF)
(a) Reduced activity of factor VIII: PTT increased
(b) Platelet “stickiness” impaired, numbers adequate
(2) Preoperative therapies
(a) Desmopressin (DDAVP) can increase vWF.
(b) Cryoprecipitate (has factor VIII) in scheduled twice-daily doses
D. Perianesthesia nursing assessments and interventions
1. Preanesthesia
a. Identify at-risk patients: coagulation risk and bleeding history.
(1) Risk of intraspinal or epidural hematoma increases if an anticoagulated patient receives regional anesthesia.
(2) Undetected coagulopathy can underlie persistent postsurgical bleeding.
b. Document date and time of most recent anticoagulant medication.
(1) Coumadin, heparin, clopidogrel
(2) Aspirin, NSAIDs
(3) Chemotherapy agents that suppress bone marrow
c. A patient with a significant bleeding disorder is an unlikely candidate for outpatient surgery with discharge home.
2. Postanesthesia
a. Observe often for insidious bleeding.
(1) Always look under the patient as well as at the wound itself.
(2) Increasing abdominal girth after laparoscopic procedures
(3) An obese patient can accumulate a lot of blood in the abdomen before distention or tenderness is evident.
(4) Oozing and bruising from incisions or venipuncture sites
b. Link vital signs and oxygenation changes with bleeding potential.
(1) Continuously monitor oxygen saturation, observe respiratory quality. Persistently low Sp o2 may indicate undetected hemoglobin loss.
(2) Measure hemoglobin: anemia often associated with coagulopathy.
(3) Support blood pressure with adequate fluid volume.
(a) Maintain IV patency and limit venipuncture.
(b) Consider central or arterial line for laboratory sampling.
(4) Transfuse selected blood components as indicated per physician order.
V. TRANSFUSION PHYSIOLOGY: BLOOD CELL COMPATIBILITY
A. Blood and blood components
1. Whole blood: 1 unit = 500 mL with hematocrit of approximately 35%
a. Used if profound bleeding or desired component unavailable
b. Contains RBCs, plasma, WBCs, and platelets
c. Must be ABO identical
d. Irradiated whole blood: donor leukocytes inactivated
(1) Reduce risk of graft-versus-host disease
2. Packed RBCs: 1 unit = 250 to 300 mL with hematocrit of approximately 60%
a. Most commonly transfused component: used to restore oxygen-carrying capacity
b. Contains
(1) RBCs
(2) Nonfunctional WBC
(3) Platelets
(4) Minimal plasma
c. Must be ABO compatible
d. In the average adult who is not bleeding or hemolyzing:
(1) Hemoglobin increases by 1 g/dL.
(2) Hct increases by 3% per 1 unit.
e. Leukocyte-reduced RBCs
(1) Indication
(a) History of multiple febrile nonhemolytic transfusion reactions
(b) Frequent transfusion candidates—risk for alloimmunization to leukocyte antigens
(c) Targeted populations—immunocompromised (prevent CMV infection)
f. Irradiated RBCs
(1) Leukocytes inactivated; reduce risk of graft-versus-host disease
(2) Highly immunocompromised (e.g., bone marrow or solid organ transplant)
3. Platelet concentrates:
a. One pack = 50 to 300 mL
b. One unit of platelets increases platelet count (5000-10,000 for average sized adult)
c. Restore clotting ability
d. Pooled platelets donor but some patients may require single platelet donor
4. Available depending on the indication, leukocyte-reduced or irradiated
a. Treats:
(1) Leukemia
(2) DIC
(3) Bleeding caused by thrombocytopenia
(4) Platelet suppression caused by chemotherapy or radiation
5. FFP: 1 unit = 125 to 260 mL
a. Unconcentrated plasma containing all coagulation factors except platelets
b. Must be ABO compatible; use within 24 hours after thawing.
c. Treats:
(1) Coagulation deficiencies secondary to liver disease
(2) DIC
(3) Antithrombin III deficiency
(4) Dilutional coagulopathy after massive blood replacement
6. Cryoprecipitate antihemophilic factor (Cryo)
a. ABO-compatible preferred
(1) Rh type does not need to be considered.
b. Concentrated factors derived from FFP, ABO compatibility preferred
(1) Rh type need not be considered.
c. Contains:
(1) Fibrinogen
(2) Factors
(a) VIII
(b) vWF
(c) XIII
d. Use within 4 hours after thawing to treat:
(1) Hemophilia A
(2) DIC
(3) Von Willebrand’s disease
(4) Obstetric complications
(5) Fibrinogen deficiency
7. Granulocytes
a. Usage
(1) Neutropenic patients with documented infections and do not respond to antibiotics
(2) Hereditary neutrophil function defects
b. Must be ABO compatible
c. Irradiated: reduces risk of graft-versus-host disease
8. Serum albumin: 5% solution, up to 500 mL; 25% solution, up to 100 mL
a. Sterile product contains:
(1) 96% albumin
(2) 4% globulin
(3) Other proteins
b. Obtained from pooled plasma, heat treated to inactivate hepatitis virus
c. Widely used for its oncotic properties
d. Treats:
(1) Hypovolemia: expands plasma volume
(2) Hypoproteinemia
9. Plasma protein fraction (Plasmanate, PPF) 1 unit = 50, 250, or 500 mL
a. Contains:
(1) 88% albumin
(2) 12% globulins
(3) No coagulation factors
b. Obtained from pooled plasma, heat treated to inactivate hepatitis virus
c. Treats:
(1) Hypovolemia: a volume expander
(2) Hypoproteinemia
B. Four major blood types: A, B, AB, O
1. A or B antigens, or both, carried on surface of RBCs
2. Form blood type A, B, or AB (Table 29-2)
a. “Universal recipient”
(1) Blood type AB
(2) Produces no antibodies
b. “Universal donor”
(1) Blood type O
c. Plasma carries naturally occurring antibodies to antigens not present on the red cell.
| Patient Blood Type | Compatible Donor | Antigen | Antibody |
|---|---|---|---|
| A | A or O | A | B |
| B | B or O | B | A |
| AB | AB, or A, B, O | AB | None |
| O | O only | None | AB |
C. Rh type: determined primarily by the D antigen
1. Positive or negative antigen carried on surface of RBCs
a. Rh + (positive for the D antigen) occurs in more than 80% of people.
b. Rh − (negative for the D antigen) occurs in less than 20%.
2. Rh +, must receive Rh + cells; and Rh −, must receive Rh − cells.
3. Detection crucial to prevent:
a. Significant antibody stimulation from multiple transfusions: makes crossmatching for future transfusions difficult
b. Hemolytic disease of newborn antibodies produced in Rh − woman pregnant with Rh + fetus
(1) Give RhoGAM per physician order to Rh − mother to prevent hemolysis of a future baby’s blood whether after full-term birth, miscarriage, or abortion.
VI. ADMINISTERING BLOOD AND BLOOD PRODUCTS
A. Why transfuse? Indications
1. Restore circulating volume.
2. Increase oxygen transport to tissues.
3. Replace coagulation factors or correct bleeding.
4. Replace granulocytes or treat sepsis.
B. Accuracy required to ensure patient safety; for every blood component
1. Check patient orders.
2. Verify correct patient and blood component: follow facility policy.
3. Verify patient consent for transfusion.
4. At patient’s bedside, two (2) licensed staff simultaneously match information on patient, blood component, and blood bank compatibility label.
a. Patient name and hospital identification number
b. Donor number on blood product
c. ABO and Rh type
d. Expiration date of component
5. Report any identification discrepancy to blood bank immediately and delay transfusion.
6. Prepare to transfuse.
a. Prime blood tubing with normal saline; cover filter in drip chamber.
(1) D 5W (5% dextrose in water) is hypotonic and causes hemolysis.
(2) Ringer’s lactate contains calcium, can initiate coagulation.
(3) Change blood tubing and filter after every 2 units: filter traps clots and coagulant debris.
(4) Never add medications to a unit of blood or piggyback into tubing—this includes narcotic analgesics delivered by patient-controlled analgesia.
b. Gently mix contents and examine unit carefully for bubbles, plasma discoloration.
c. Explain procedure and transfusion need to patient.
d. Verify:
(1) IV patent
(2) Nonreddened site
(3) An 18- or 19-gauge catheter
e. Before starting transfusion, measure and document patient’s temperature, blood pressure, vital signs, and heart rate.
f. Keep patient warm for comfort.
(1) Use blood warmer, particularly if transfusing multiple units.
(2) Apply warm blankets, active rewarming device.
(3) Note transfusion reaction signals:
(a) New-onset of chills
(b) Shivering
(c) Immediately stop blood transfusion.
g. Start infusion slowly, and remain with patient for initial 15 to 20 minutes of infusion: document vital signs and observe for transfusion reaction.
h. Frequently monitor infusion and patient response.
(1) Rate: 30 minutes to 4 hours according to acuity, patient tolerance
(a) Apply pressure bag to rapidly administer cells or volume.
(b) FDA regulations require a transfusion to be completed within 4 hours.
(2) Document vital signs if clinical change and after infusion.
i. Should a transfusion reaction occur, notify:
(1) Blood bank
(2) Surgeon
(3) Anesthesiologist
(4) Follow established protocols of institution.
C. Transfusion complications
1. Hemolytic reaction is a severe reaction caused by:
a. ABO incompatibility: immediate hemolysis of RBCs after infusion of the first few milliliters of blood
b. Human clerical error: patient or blood component not properly identified and matched; usual cause of hemolytic reactions
c. Assessment and observations
(1) Burning sensation along vein receiving transfusion
(2) Sudden fever (temperature >104° F [40° C]) and chills
(3) Hypotension, hematuria, and hemolysis with:
(a) Hematuria, flank pain, and renal failure
(b) Dyspnea, tachypnea, tachycardia, palpitations, substernal pain
(4) Abnormal bleeding or DIC
d. Be especially vigilant with the anesthetized or sedated patient.
(1) Immediately report unexplained, significant oozing.
(2) Patient cannot report pain, anxiety.
(3) Difficult to distinguish hypotension caused by transfusion reaction from hypotension caused by hypovolemic shock
(4) Muscle relaxant may limit shivering response.
e. Intervention and evaluation
(1) Discontinue transfusion immediately!
(2) Assess and document patient’s clinical condition.
(3) Infuse normal saline (use new tubing) and inform physician.
(4) Complete transfusion reaction profile and return.
(a) Facility’s investigation form to blood bank
(b) Intact set of blood component unit, tubing, and accompanying IV fluid to blood bank
(c) Blood samples as indicated by facility
(d) Urine sample for urine hemoglobin to laboratory
(5) Simultaneously treat patient per physician orders.
(a) Acetaminophen for fever
(b) Diphenhydramine (Benadryl) for itching
(c) Cautious fluid management
(d) Furosemide if needed for diuresis
(e) Frequently monitor and document patient’s response.
2. Delayed hemolytic transfusion reaction
a. Usually occurs several days after transfusion: transfused cells have antigen to which recipient has been previously sensitized
b. Causative antibodies: Anti-E, Anti-C, Kidd system
c. Assessment
(1) Unexplained fever
(2) Definite hemoglobin decrease 2 to 10 days posttransfusion
(3) Positive direct Coombs’ test, elevated bilirubin
3. Pyrogenic (febrile) transfusion reaction
a. Not hemolytic: onset 1 hour into transfusion, may last 8 to 10 hours
b. Causes
(1) WBC or platelet antibodies
(2) Contaminating pyrogenic bacteria
(3) Pregnancy or previous transfusion
c. Assessment and intervention
(1) New-onset chills with fever, temperature increase 2° F.
(2) Flushed skin, headache, tachycardia
(3) Hemolysis: bacteria replicate quickly even when refrigerated—symptoms after infusion of first 50 mL of blood.
(4) Severe hypotension, abdominal and extremity pain
(5) Hematuria, DIC, and renal failure
d. Intervention and evaluation
(1) Discontinue transfusion! Early signs parallel early hemolytic reaction.
(2) Begin transfusion reaction investigation.
(3) Antipyretics (acetaminophen) and antihistamine for itching (diphenhydramine)
(4) Fluids to support blood pressure and urine volume; monitor airway.
4. Allergic transfusion reaction
a. Hypersensitivity response: accounts for 1% to 3% of transfusion reactions
b. Occurs as a result of antibodies to donor blood foreign proteins, often in a patient with significant allergy history
c. Develop urticaria with hives, itching
d. Assessment and intervention
(1) Stop transfusion! Reaction may progress unpredictably.
(2) Assess for glottal edema.
(3) Give IV antihistamine (Diphenhydramine/Benadryl).
BIBLIOGRAPHY
1. American Red Cross, Practice guidleines for blood transfusion, a compilation from recent peer-reviewed literature. ed 2 ( 2007) .
2. Adamson, J.D., New Blood, Old Blood, or No Blood?N Engl J Med 358 (2008) 1295–1296.
3. Advancing Transfusion and Cellular Therapies Worldwide, Circular of information for the use of human blood and blood components. ( 2002) .
4. ASA, Practice guidelines for perioperative blood transfusion and adjuvant therapies, Anesthesiology 105 (2006) 198–208.
5. ASA, Questions and answers about blood management. ed 4 ( 2006–2007) .
6. Dennison, R.D., Pass CCRN. ed 3 ( 2007)Mosby, St Louis.
7. Goodnough, L.T.; Shander, A., Blood management, Arch Pathol Lab Med 131 (2007) 695–701.
8. Joyce, J.A., Toward reducing perioperative transfusions, AANA J 76 (2008) 131–137.
9. Justice, H.M.; Mason, J.D., Recognizing acquired thrombocytopenic coagulations, Emerg Med 39 (7) ( 2007) 7–13.
10. Lambing, A., Bleeding disorders: Patient history key to diagnosis, Nurse Pract 32 (2007) 16–24.
11. Kam, P.C.A., Anaesthetic management of a patient with thrombocytopenia, Curr Opin Anaesthesiol 21 (2008) 369–374.
12. Klein, H.; Spahn, D.; Carson, J., Red blood cell transfusion in clinical practice, Lancet 370 (2007) 415–426.
13. Knippen, M.A., Transfusion-related acute lung injury, AJN 106 (2006) 61–64.
14. Nagelhout, J.; Plaus, K., Nurse anesthesia. ed 4 ( 2010)Saunders, St Louis.
15. Platt, O., Hydroxyurea for the treatment of sickle cell anemia, N Engl J Med 358 (2008) 1362–1369.
16. Rempher, K.J., Assessment of red blood cell and coagulation laboratory data, AACN Adv Crit Care 15 (2004) 622–637.
17. Roisen, M.F.; Fleisher, L., Essence of anesthesia practice. ed 2 ( 2002)WB Saunders, Philadelphia.