Wrist and hand
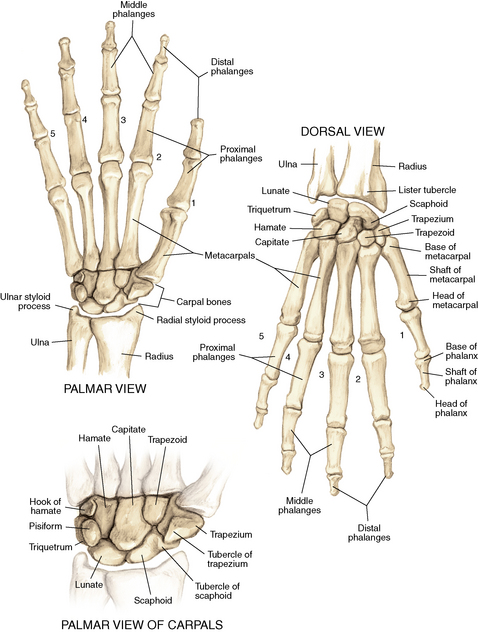
Anatomy
Ligaments: Figure 4-2
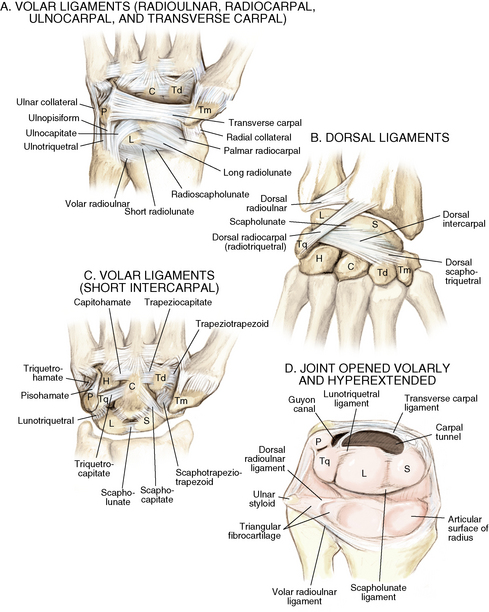
Figure 4-2. A to D, Ligaments of the wrist. Ca, capitate; H, hamate; L, lunate; P, pisiform; S, scaphoid; Td, trapezoid; Tm, trapezium; Tq, triquetrum. (From Chhabra AB: Wrist and hand. In Miller MD, Chhabra AB, Hurwitz S, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, p 150.)
Muscles and tendons: Figures 4-3 through 4-7
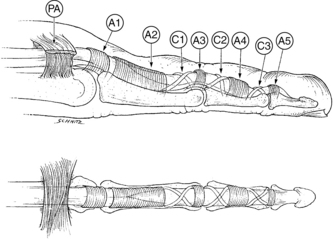
Figure 4-3. Flexor tendon pulley system.
A1 to A5, annular pulleys; C1 to C3, cruciate pulleys; PA, palmar aponeurosis. (From Strickland JW: Flexor tendons: acute injuries. In Green DP, editor: Operative hand surgery, ed 4, New York, 1999, Churchill Livingstone, p 1853.)
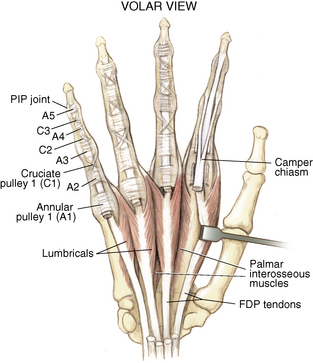
Figure 4-4. Volar muscles of the hand: lumbricals and palmar interossei. FDP, flexor digitorum profundus; PIP, proximal interphalangeal. (From Chhabra AB: Wrist and hand. In Miller MD, Chhabra AB, Hurwitz S, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, p 154.)
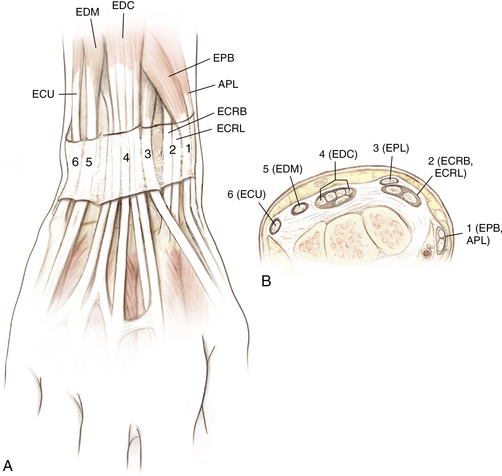
Figure 4-6. A and B, Extensor tendon compartments of wrist. APL, abductor pollicis longus; ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radialis longus; ECU, extensor carpi ulnaris; EDC, extensor digitorum communis; EDM, extensor digiti minimi. (From Chhabra AB: Wrist and hand. In Miller MD, Chhabra AB, Hurwitz S, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, p 157.)

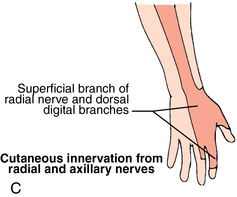
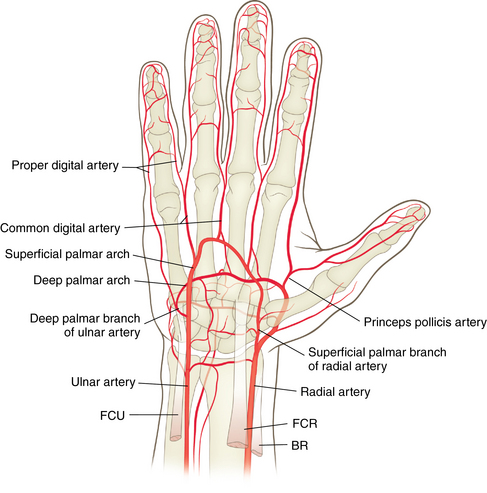
Nerves and arteries: Figures 4-8 through 4-10 and table 4-1


Surface anatomy: Figure 4-11
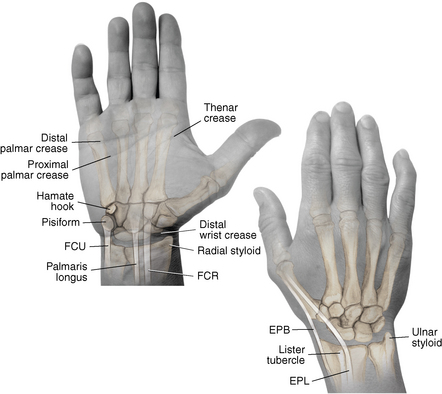
Figure 4-11. Surface anatomy of the hand and wrist.
EPB, extensor pollicis brevis; EPL, extensor pollicis longus; FCR, flexor carpi radialis; FCU, flexor carpi ulnaris. (From Chhabra AB: Wrist and hand. In Miller MD, Chhabra AB, Hurwitz S, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, p 163.)
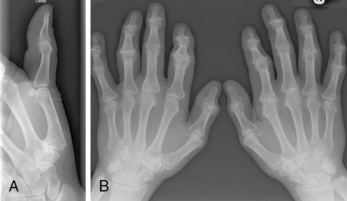
Normal radiographic appearance: Figures 4-12 through 4-14
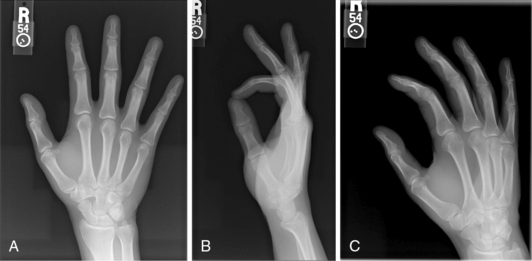
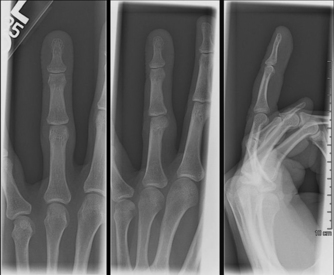
Figure 4-12. Normal radiographs of the hand.
Anteroposterior (A), lateral (B), and oblique (C) views of the hand. (From Hart JA: Overview of the wrist and hand. In Miller MD, Hart JA, MacKnight JM, editors: Essential orthopaedics, Philadelphia, 2010, Saunders, p 303.)

Physical examination
Inspect for scars, muscle atrophy, edema, erythema or deformity.
Palpate specific structures to evaluate complaint:
• Distal radioulnar joint (DRUJ)
• Anatomic snuffbox, scaphoid tubercle
• First extensor compartment, extensor carpi radialis ulnaris, extensor carpi radialis brevis, extensor carpi radialis longus
• Scapholunate (SL) interval (approximately 1 to 3 cm distal from Lister tubercle)
• First carpometacarpal (CMC) joint
• Flexor carpi ulnaris (FCU) tendon
• Extensor carpi ulnaris (ECU) tendon
Normal wrist range of motion (ROM): Table 4-2
Table 4-2.
| Extension | 80 degrees |
| Flexion | 70 degrees |
| Supination | 90 degrees |
| Pronation | 90 degrees |
| Ulnar deviation | 30 degrees |
| Radial deviation | 20 degrees |
Neurovascular examination of the wrist and hand: Table 4-3
Table 4-3.
Neurovascular Examination of the Wrist and Hand
| NERVE | LOCATION OF TEST | TESTS |
| Median nerve | Carpal tunnel | Tinel, Phalen, Durkan test (see page 140) |
| Ulnar nerve | Guyon canal/medial epicondyle | Tinel test |
| Superficial sensory radial nerve | At radial styloid | Tinel test |
| Radial and ulnar artery | At volar wrist | Allen test for dominance or perfusion |
Differential diagnosis of wrist pain: Table 4-4
Table 4-4.
Differential Diagnosis of Wrist Pain
| Radial-sided wrist pain | Distal radius fracture SLL tear Arthritis Scaphoid fracture Extensor tendinitis de Quervain tenosynovitis |
| Ulnar-sided wrist pain | TFCC tear FCU tendinitis Ulnar artery thrombosis Cubital tunnel syndrome Pisotriquetral arthritis ECU tendinitis Distal ulnar fracture Lunotriquetral tear Hook hamate fracture |
| Dorsal wrist pain | Extensor tendinitis Arthritis SLL tear Scaphoid fracture |
| Volar wrist pain | FCU or FCR tendinitis Carpal tunnel syndrome |
Scaphoid fracture











Differential diagnosis







Treatment options
 Conservative management is reserved for nondisplaced fractures in which patient declines surgery or for patients too ill for surgery.
Conservative management is reserved for nondisplaced fractures in which patient declines surgery or for patients too ill for surgery.
 Nondisplaced waist fractures have an 88% to 95% healing rate if treated within 3 weeks of injury.
Nondisplaced waist fractures have an 88% to 95% healing rate if treated within 3 weeks of injury.


 A computed tomography (CT) scan may be necessary to confirm healing after 8 to 12 weeks.
A computed tomography (CT) scan may be necessary to confirm healing after 8 to 12 weeks.



Pearl
An MRI scan is a good way to diagnose an occult scaphoid fracture early. The scan is useful before 3 weeks in high-level athletes or in patients for whom remaining out of work for 3 weeks while in a splint would be financially detrimental.
 ORTHOPAEDIC WARNING
ORTHOPAEDIC WARNING
• This pattern of arthritis is called scaphoid nonunion advanced collapse (SNAC) and is similar to the pattern of arthritis associated with an untreated scapholunate ligament tear (see page 129)
• If arthritis is present, proceed as if treating the underlying arthritis and not the scaphoid nonunion. Treatment would include a wrist support, activity modification, nonsteroidal antiinflammatory drugs, and possible intra-articular steroid injection.
Operative management of acute scaphoid fractures









Surgical procedures
 Dorsal approach for proximal pole fractures
Dorsal approach for proximal pole fractures
 Volar approach for distal pole and waist fractures
Volar approach for distal pole and waist fractures
 For either approach, placement of a forearm-based thumb spica splint
For either approach, placement of a forearm-based thumb spica splint
Open reduction, internal fixation



Percutaneous internal fixation: Figure 4-16

 This technique may be used preferentially for nondisplaced scaphoid fractures. The procedure is similar to the open technique, just performed percutaneously. With the patient’s wrist flexed, a guidewire is placed down the central axis of the scaphoid. The guidewire is also used to measure the appropriate screw length. After fluoroscopic confirmation of adequate reduction, a screw is placed for fixation. Place the patient in a thumb spica splint following surgery.
This technique may be used preferentially for nondisplaced scaphoid fractures. The procedure is similar to the open technique, just performed percutaneously. With the patient’s wrist flexed, a guidewire is placed down the central axis of the scaphoid. The guidewire is also used to measure the appropriate screw length. After fluoroscopic confirmation of adequate reduction, a screw is placed for fixation. Place the patient in a thumb spica splint following surgery.
Estimated postoperative course

• Sutures are removed, and a wound check is performed.
• Radiographs consist of wrist PA, lateral, oblique, and navicular views.
• Immobilization: The patient is placed into a removable thumb spica splint.
• Therapy referral: Start edema control and gentle finger and wrist ROM only.
• Note: Some surgeons prefer cast immobilization in a thumb spica cast during the initial postoperative period, especially if the fracture was difficult to reduce or especially comminuted.

• The patient returns for a motion check.
• Radiographs consist of wrist PA, lateral, and scaphoid views.
• Therapy: If healing is present, progress therapy to more aggressive wrist ROM, wean from the splint, and start gradual weight bearing.
• If no healing is noted, continue gentle ROM and have the patient wear the brace at all times until healing is evident on radiographs.

• The patient returns for a motion check.
• Assess for tenderness at the anatomic snuffbox and scaphoid tubercle.
• Radiographs consist of wrist PA, lateral, and scaphoid views.
• If the injury is healed and no pain is noted on examination, release the patient to regular activities without restrictions.
• If no evidence of healing is seen on radiographs, consider use of a bone stimulator and possibly obtain a CT scan to evaluate for healing.
• Nonunion occurs if there has been no healing by 6 months postoperatively.
Distal radius fractures










Classification
Describe the fracture in terms of displacement, comminution, radial length, surface tilt, and articular step-off (Figure 4-18 and Table 4-6).
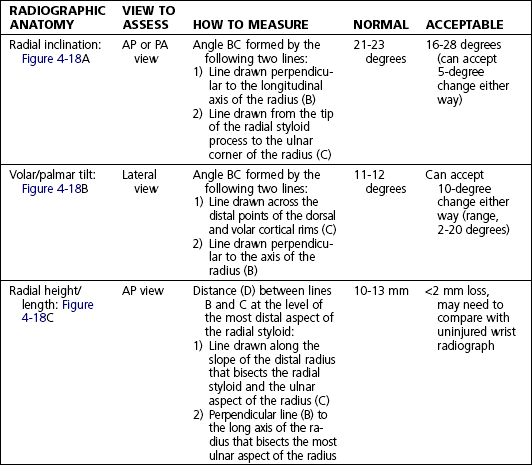
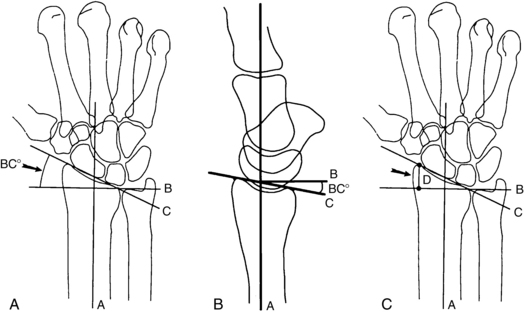
Figure 4-18. How to determine whether a distal radius fracture meets operative criteria. A, Radial inclination. B, Volar tilt. C, Radial height. (Adapted from Baratz ME, Larsen CF. Wrist and hand measurements and classification schemes. In Gilula LA, Yin Y (eds). Imaging of the wrist and hand, Philadelphia, Saunders, 1996.)




Initial treatment
 The distal radius is the most commonly fractured bone in the arm. The fracture pattern determines surgical versus nonsurgical treatment. If the fracture is nondisplaced or if the fracture has been successfully closed reduced and splinted and the fingers are sensate with good perfusion, then the injury can wait several days for evaluation by an orthopaedist. If the patient’s fingers are numb and/or not well perfused or the fracture is not able to be reduced, the patient should have an immediate surgical evaluation.
The distal radius is the most commonly fractured bone in the arm. The fracture pattern determines surgical versus nonsurgical treatment. If the fracture is nondisplaced or if the fracture has been successfully closed reduced and splinted and the fingers are sensate with good perfusion, then the injury can wait several days for evaluation by an orthopaedist. If the patient’s fingers are numb and/or not well perfused or the fracture is not able to be reduced, the patient should have an immediate surgical evaluation.



Treatment options
 Conservative management is reserved for nondisplaced fractures or stable reduced fractures or for patients too ill for surgery.
Conservative management is reserved for nondisplaced fractures or stable reduced fractures or for patients too ill for surgery.
 Nondisplaced fractures require casting for 6 to 8 weeks in a short-arm cast.
Nondisplaced fractures require casting for 6 to 8 weeks in a short-arm cast.
 Generally, after 6 weeks of immobilization, patients may progress with ROM.
Generally, after 6 weeks of immobilization, patients may progress with ROM.
• Stable reduced fractures require 3 weeks in a sugar tong splint with weekly radiographs in the splint to ensure that fracture alignment is maintained. If the reduction is lost, surgery is recommended. If fracture reduction is maintained for 3 weeks, transition the patient to a short-arm cast with radiographs immediately following new cast placement to ensure alignment.
• The fracture is considered healed if there is radiographic evidence of healing and the patient is nontender over the distal radius. This usually occurs in approximately 2 to 3 months, depending on the severity of the original injury.


Operative management of acute distal radius fractures
Codes







Surgical procedures

Open reduction, internal fixation: See figure 4-19
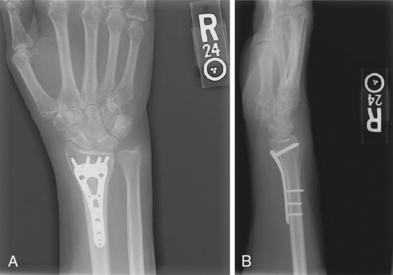
Figure 4-19. Surgical fixation of a displaced distal radius fracture with a volar locking plate. Posteroanterior (A) and lateral (B) views.


Estimated postoperative course

• Sutures are removed, and a wound check is performed.
• Possible radiographs include wrist PA, lateral, and oblique views.
• Immobilization: The patient is placed into a removable spica splint.
• Therapy referral: Start edema control and gentle finger and wrist motion only. Some clinicians start therapy at 3 to 5 days postoperatively.
• Note: Some surgeons prefer cast immobilization in a short-arm cast during the initial postoperative period, especially if the fracture was difficult to reduce or especially comminuted.


Trigger finger




Physical examination








Differential diagnosis



 ORTHOPAEDIC WARNING
ORTHOPAEDIC WARNINGInitial treatment
 Triggering may affect more than one digit, with a higher incidence in patients with diabetes and thyroid disease. There is about an 80% cure rate after the first cortisone injection; if the first injection is unsuccessful, a second injection may be done 3 to 6 weeks later. If triggering is still present after the second injection, consider surgical intervention.
Triggering may affect more than one digit, with a higher incidence in patients with diabetes and thyroid disease. There is about an 80% cure rate after the first cortisone injection; if the first injection is unsuccessful, a second injection may be done 3 to 6 weeks later. If triggering is still present after the second injection, consider surgical intervention.
Treatment options











Surgical procedures
 Local anesthetic can be injected before the skin incision is made.
Local anesthetic can be injected before the skin incision is made.
 A small, transverse incision is made over the level of the A1 pulley.
A small, transverse incision is made over the level of the A1 pulley.
 The skin and subcutaneous tissues are incised to expose the flexor tendon sheath.
The skin and subcutaneous tissues are incised to expose the flexor tendon sheath.
 Identify and protect the neurovascular bundles.
Identify and protect the neurovascular bundles.
 Identify and release the A1 pulley in its entirety.
Identify and release the A1 pulley in its entirety.
 Preserve the A2 pulley to prevent bowstringing.
Preserve the A2 pulley to prevent bowstringing.

 Place the patient in a soft hand dressing following surgery.
Place the patient in a soft hand dressing following surgery.
Estimated postoperative course


Scapholunate ligament tear



Physical examination


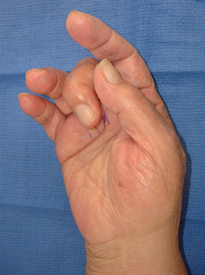
 Positive Watson maneuver (Fig. 4-21)
Positive Watson maneuver (Fig. 4-21)
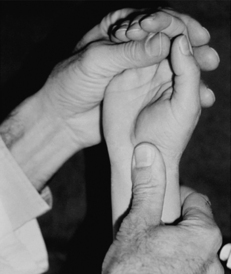
• Watson maneuver tests for SLL instability. The examiner places his or her thumb firmly on the patient’s volar wrist over the scaphoid tubercle and applies pressure. With the other hand, the examiner moves the patient’s wrist from ulnar to radial deviation. A positive test result occurs when there is a palpable “clunk” with pain. The presence of a clunk alone is not a positive test result.
• The clunk occurs when the scaphoid has dissociated from the lunate because of an SLL tear and hits against the dorsal lip of the radius during the maneuver.
Imaging
 Order wrist radiographs: PA, lateral, oblique, clenched fist, and scaphoid (navicular) views.
Order wrist radiographs: PA, lateral, oblique, clenched fist, and scaphoid (navicular) views.
 Clenched fist views may show widening of the SL interval (>3 to 4 mm is abnormal; must compare with the contralateral side) (Fig. 4-22).
Clenched fist views may show widening of the SL interval (>3 to 4 mm is abnormal; must compare with the contralateral side) (Fig. 4-22).

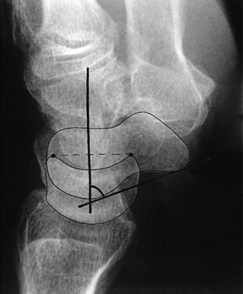
 The lateral view may show an SL angle greater than 60 degrees (an increased SL angle is also known as dorsal intercalated segment instability or DISI). The normal angle is 30 to 60 degrees (Fig. 4-23).
The lateral view may show an SL angle greater than 60 degrees (an increased SL angle is also known as dorsal intercalated segment instability or DISI). The normal angle is 30 to 60 degrees (Fig. 4-23).
 The PA view may reveal a scaphoid ring sign (Fig. 4-24).
The PA view may reveal a scaphoid ring sign (Fig. 4-24).

Figure 4-24. Scaphoid ring sign (arrowheads).
Double arrow, SL interval. (From Green DP, Hotchkiss RN, Pederson WC, et al, editors: Green’s operative hand surgery. In Marc Garcia-Elias and William B. Geissler, editors: Carpal Instability, ed 5, Philadelphia, 2005, Churchill Livingstone p 557.)

 The gold standard for diagnosis of a tear is wrist arthroscopy.
The gold standard for diagnosis of a tear is wrist arthroscopy.
Classification
Stages of instability resulting from ligament injury
 ORTHOPAEDIC WARNING
ORTHOPAEDIC WARNINGScapholunate advanced collapse (SLAC): Figure 4-25

This term refers to a predictable pattern of osteoarthritis of the wrist that results from a chronic untreated SL tear. The radioscaphoid joint is first affected, followed by the lunatocapitate joint (Fig. 4-26).
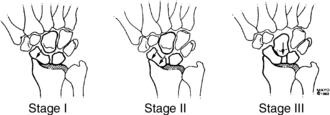
Figure 4-26. Stages of scapholunate advanced collapse (arrows). Note with advancing stage, capitate migrates proximally. (From Shin AY, Moran SL: Carpal instability including dislocation. In Trumble T, Budoff J, Cornwall R, editors: Hand, elbow, and shoulder: core knowledge in orthopaedics, Philadelphia, 2006, Mosby, p 151.)





Initial treatment
 SLL instability is the most common form of carpal instability. Complete tears should be treated surgically within 6 weeks. Complete SLL tears left untreated will lead to wrist arthritis (SLAC wrist). Partial SLL tears may be treated with casting and/or cortisone injections. If symptomatic after conservative treatment, patients with partial SLL tears may undergo wrist arthroscopy for staging, débridement, and treatment planning.
SLL instability is the most common form of carpal instability. Complete tears should be treated surgically within 6 weeks. Complete SLL tears left untreated will lead to wrist arthritis (SLAC wrist). Partial SLL tears may be treated with casting and/or cortisone injections. If symptomatic after conservative treatment, patients with partial SLL tears may undergo wrist arthroscopy for staging, débridement, and treatment planning.


Treatment options
 Conservative management is reserved for patients with partial tears or chronic complete tears with evidence of static instability or patients too ill for surgery.
Conservative management is reserved for patients with partial tears or chronic complete tears with evidence of static instability or patients too ill for surgery.
• Partial tears: Cast immobilization for 4 to 6 weeks is indicated. If immobilization does not provide relief, consider radiocarpal wrist injection.
• Chronic injuries (>6 months) respond poorly to surgical repair. Consider symptom control with splinting and radiocarpal cortisone injections as needed. Patients should be counseled that arthritic changes and loss of motion will be expected.
• Salvage procedures for symptomatic injuries that are identified late (chronic injuries) include proximal row carpectomy and total wrist fusion (for stages 3 and 4). Surgery should be suggested only after conservative treatment has failed.







Surgical procedures





Kienbock disease









Imaging: Figure 4-27

Figure 4-27. Radiograph of stage IIIa Kienbock disease.
The lunate shows increased sclerosis and collapse. (From Thaller JB: Kienbock’s disease. In Miller MD, Hart JA, MacKnight JM, editors: Essential orthopaedics, Philadelphia, 2010, Saunders, p 318.)




Classification: table 4-7
Table 4-7.
Classification and Treatment of Kienbock Disease
| STAGE | RADIOGRAPHIC FINDINGS |
| Stage I | Normal radiographs or linear fracture; abnormal and nonspecific bone scan; on magnetic resonance imaging, lunate shows low signal intensity on T1-weighted images and high or low signal on T2-weighted images |
| Stage II | Lunate sclerosis, one or more fracture lines with possible early collapse of lunate on radial border |
| Stage IIIa | Lunate collapse with normal carpal alignment and height |
| Stage IIIb | Fixed hyperflexion of scaphoid, carpal height decreased, proximal migration of capitate |
| Stage IV | Severe lunate collapse with intra-articular degenerative changes seen at midcarpal joint and/or radiocarpal joint |
From Allan CH, Joshi A, Lictman DM: Kienbock’s disease: diagnosis and treatment, J Am Acad Orthop Surg 9: 128–136, 2001.




Initial treatment
 Kienbock disease is more common in men than in women and usually affects patients 20 to 40 years old. It is usually unilateral. Although the cause is unknown, isolated or repetitive trauma to a lunate predisposed to the disease may lead to necrosis. Treatment is based on symptoms and stage of the disease, and prognosis is very difficult to predict.
Kienbock disease is more common in men than in women and usually affects patients 20 to 40 years old. It is usually unilateral. Although the cause is unknown, isolated or repetitive trauma to a lunate predisposed to the disease may lead to necrosis. Treatment is based on symptoms and stage of the disease, and prognosis is very difficult to predict.
Treatment options (based on stage) table 4-7
 Stage I: immobilization with cast or external fixator for up to 3 months
Stage I: immobilization with cast or external fixator for up to 3 months












Triangular fibrocartilage complex tear
History




Physical examination






Imaging
 Order wrist radiographs: PA, lateral, and oblique views.
Order wrist radiographs: PA, lateral, and oblique views.
 This injury may be associated with ulnar positive variance (defined as ulna >4 mm longer than the radius) and ulnocarpal impaction syndrome (distal ulna abuts the lunate and causes degeneration of the TFCC over time) (Fig. 4-28).
This injury may be associated with ulnar positive variance (defined as ulna >4 mm longer than the radius) and ulnocarpal impaction syndrome (distal ulna abuts the lunate and causes degeneration of the TFCC over time) (Fig. 4-28).

Figure 4-28. Measuring ulnar positive variance. Radiograph shows ulnar positive variance. (From Rynders SD, Chhabra AB: Triangular fibrocartilage complex injuries. In Miller MD, Hart JA, MacKnight JM, editors: Essential orthopaedics, Philadelphia, 2010, Saunders, p 323.)
 Assess for DRUJ widening compared with the uninjured wrist on the PA view.
Assess for DRUJ widening compared with the uninjured wrist on the PA view.
 MRI, with or without contrast, is recommended for evaluating TFCC injuries. The quality of scans and the radiologist’s experience play a role in accurately diagnosing a tear. Studies suggest an accuracy rate of approximately 64% with MRI with an arthrogram. The gold standard for diagnosis is wrist arthroscopy (Fig. 4-29).
MRI, with or without contrast, is recommended for evaluating TFCC injuries. The quality of scans and the radiologist’s experience play a role in accurately diagnosing a tear. Studies suggest an accuracy rate of approximately 64% with MRI with an arthrogram. The gold standard for diagnosis is wrist arthroscopy (Fig. 4-29).

Classification*












Treatment options (based on classification)













Surgical procedures









Osteoarthritis of the wrist and hand
 Osteoarthritis usually affects the first CMC joint, PIP and DIP joints. Less commonly, the MCP joints are affected. Its predilection for the wrist joint is usually the result of a previous injury such as a remote ligament sprain or previous carpal or radius fracture.
Osteoarthritis usually affects the first CMC joint, PIP and DIP joints. Less commonly, the MCP joints are affected. Its predilection for the wrist joint is usually the result of a previous injury such as a remote ligament sprain or previous carpal or radius fracture.
 The patient may report pain, edema, stiffness, or deformity of the affected joint.
The patient may report pain, edema, stiffness, or deformity of the affected joint.
 Pain may be worse in the morning and after repetitive activities.
Pain may be worse in the morning and after repetitive activities.
Physical examination








Imaging: Figure 4-30



Classification
First carpometacarpal joint arthritis
 Eaton stages of first CMC joint osteoarthritis†
Eaton stages of first CMC joint osteoarthritis†
Stage 1: normal joint with exception of possible widening from synovitis
Stage 2: joint space narrowing with debris and osteophytes smaller than 2 mm
Stage 3: joint space narrowing with debris and osteophytes larger than 2 mm
Stage 4: scaphotrapezial joint space involvement in addition to narrowing of the CMC joint






Treatment options




Operative management of distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first carpometacarpal osteoarthritis
Codes

Informed consent and counseling
 Arthrodesis or joint fusion is a pain-relieving surgical procedure that renders the joint immobile.
Arthrodesis or joint fusion is a pain-relieving surgical procedure that renders the joint immobile.
 A risk of nonunion is reported in smokers; smoking is considered a relative contraindication.
A risk of nonunion is reported in smokers; smoking is considered a relative contraindication.

 There is a risk of nail deformity with DIP joint surgical interventions.
There is a risk of nail deformity with DIP joint surgical interventions.
 Almost all surgical interventions for arthritis require postoperative therapy.
Almost all surgical interventions for arthritis require postoperative therapy.



Carpal tunnel syndrome
Carpal tunnel syndrome (CTS) is compression of the median nerve at the wrist and is the most common compression neuropathy of the upper extremity.
History






Physical examination






Further diagnostic testing




Initial treatment


Treatment options



Operative management


Informed consent and counseling

















De quervain tenosynovitis



Physical examination
 Edema and tenderness are noted at the first dorsal extensors extending to the radial styloid.
Edema and tenderness are noted at the first dorsal extensors extending to the radial styloid.
 Positive Finkelstein test (Fig. 4-32): The thumb is clasped into the palm, and the wrist is passively ulnarly deviated. A positive test result consists of severe pain.
Positive Finkelstein test (Fig. 4-32): The thumb is clasped into the palm, and the wrist is passively ulnarly deviated. A positive test result consists of severe pain.

 Pain occurs with thumb motion or active radial deviation.
Pain occurs with thumb motion or active radial deviation.
 Occasionally, this disorder is associated with a ganglion cyst over the first dorsal compartment.
Occasionally, this disorder is associated with a ganglion cyst over the first dorsal compartment.

Differential diagnosis
 Intersection syndrome (inflammation and pain at the point where the first extensor compartment tendons cross over the second extensor compartment tendons [the extensor carpi radialis longus and the extensor carpi radialis brevis tendons, proximal to Lister tubercle of the distal radius])
Intersection syndrome (inflammation and pain at the point where the first extensor compartment tendons cross over the second extensor compartment tendons [the extensor carpi radialis longus and the extensor carpi radialis brevis tendons, proximal to Lister tubercle of the distal radius])





Initial treatment
 de Quervain tenosynovitis is more common in female patients, especially after childbirth. It is an inflammatory condition that is exacerbated by overuse. Treatment may include a thumb spica splint, hand therapy, and/or a cortisone injection. Although effective, cortisone injections in this area may cause subcutaneous fat atrophy and/or skin hypopigmentation at the injection site.
de Quervain tenosynovitis is more common in female patients, especially after childbirth. It is an inflammatory condition that is exacerbated by overuse. Treatment may include a thumb spica splint, hand therapy, and/or a cortisone injection. Although effective, cortisone injections in this area may cause subcutaneous fat atrophy and/or skin hypopigmentation at the injection site.









Surgical procedure
First dorsal compartment release
 Approach via the first extensor compartment radially with a short transverse incision.
Approach via the first extensor compartment radially with a short transverse incision.
 Divide the extensor retinaculum longitudinally.
Divide the extensor retinaculum longitudinally.
 Protect the SSRN and its branches, and avoid excessive dissection.
Protect the SSRN and its branches, and avoid excessive dissection.
 Release the first dorsal compartment on its dorsal margin.
Release the first dorsal compartment on its dorsal margin.







