[level-membership-for-neurology-category]
Weakness
Weakness is a common symptom and a commonly elicited sign on neurological examination. Weakness arises from lesions at every level of the nervous system. This produces:


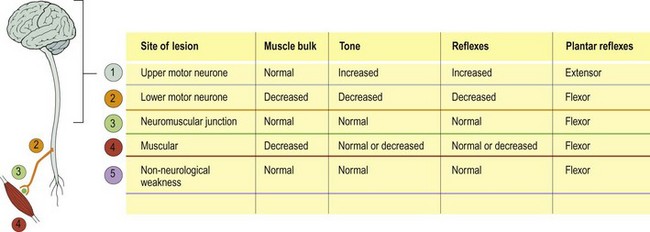
As with all neurology, the time course of the development of the weakness, which comes from the history, is most important in understanding its aetiology. Sometimes patients complain of weakness when they mean something else, for example fatigue. Similarly, other abnormalities can be mistaken for weakness on examination (Box 1).







The distribution of the weakness reflects the site of the lesion (Fig. 2). Broadly speaking, hemisphere or brain stem lesions produce contralateral weakness affecting a combination of the face, arm or leg depending on the site. There are usually other signs, either with disturbance of higher function speech or cranial nerve signs or sensory signs, to help locate the lesion.
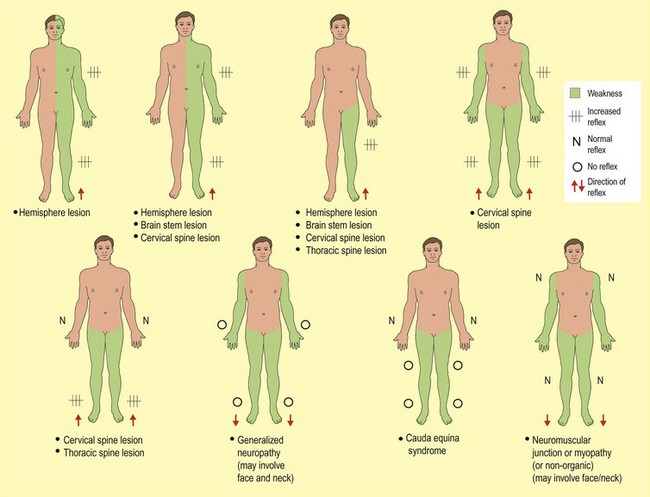
Lower motor neurone lesions




The distribution reflects the pattern of lower motor neurone involvement. A generalized neuropathy can produce generalized weakness, though a distal weakness is more common (p. 102). Nerve root lesions and peripheral nerve lesions produce changes within the distribution of the nerve or root (pp. 82, 106). Usually there are associated sensory signs.
One important pattern of lower motor neurone weakness is the weakness of both legs, particularly of recent onset. This reflects a cauda equina lesion. This is usually associated with sensory and sphincter signs (p. 83).
Anterior horn cell disease produces prominent wasting and fasciculation with normal sensation. Some conditions produce upper and lower motor neurone signs. These include cervical and spine disease where spinal cord compression produces upper motor neurone signs, and where root compression produces lower motor neurone signs. There are usually associated sensory signs (pp. 80–84). Motor neurone disease (amyotrophic lateral sclerosis; ALS) produces a mixture of upper motor and lower motor neurone signs without sensory loss (p. 108).
Muscle weakness
Muscle disease produces weakness in several distributions. Indeed, this pattern of distribution has founded the basis of clinical classification (p. 112). However, most commonly it produces proximal limb weakness.
Non-neurologically determined weakness




[/level-membership-for-neurology-category][not-level-membership-for-neurology-category]
Weakness
Weakness is a common symptom and a commonly elicited sign on neurological examination. Weakness arises from lesions at every level of the nervous system. This produces:
As with all neurology, the time course of the development of the weakness, which comes from the history, is most important in understanding its aetiology. Sometimes patients complain of weakness when they mean something else, for example fatigue. Similarly, other abnormalities can be mistaken for weakness on examination (Box 1).
