Chapter 43 WasherLoc and Bone Dowel Tibial Fixation of a Soft-Tissue Graft
WasherLoc and Bone Dowel Surgical Technique
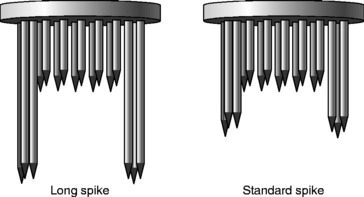
The superior clinical and biomechanical performance of the WasherLoc and bone dowel during aggressive rehabilitation and testing in the laboratory has been extensively documented since the technique was introduced in 1997.1–13 The WasherLoc is a multi-spiked washer with four long peripheral spikes that engage cortical bone and multiple shorter spikes that purchase the soft-tissue graft (Fig. 43-1). The WasherLoc comes in two lengths (long and standard) and three diameters (14, 16, and 18 mm). The preferred fixation for a 9- to 10-mm diameter soft-tissue graft is the 18-mm-long spike WasherLoc; for a 7- to 8-mm diameter graft, the 16-mm long spike WasherLoc.
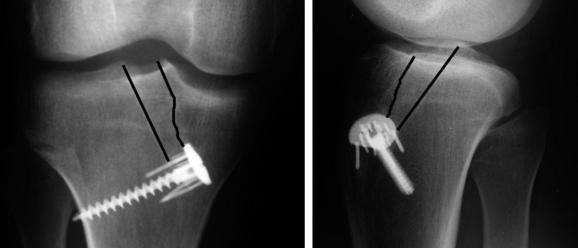
The WasherLoc is seated in a counterbore inside the distal end of the tibial tunnel. The counterbore recesses the WasherLoc below the cortical surface, which eliminates hardware irritation of the overlying skin (Fig. 43-2).9 A self-tapping, cancellous screw compresses the WasherLoc and soft-tissue graft against the back wall of the tibial tunnel. The tip of the screw engages the lateral tibial cortex, which avoids any damage to the more posterior neurovascular structures. The portion of the tunnel anterior to the soft-tissue graft is dilated, and the bone dowel is compacted into the tunnel. The following is a detailed description of the surgical technique with pertinent illustrations.
Harvest a Bone Dowel from the Tibial Tunnel
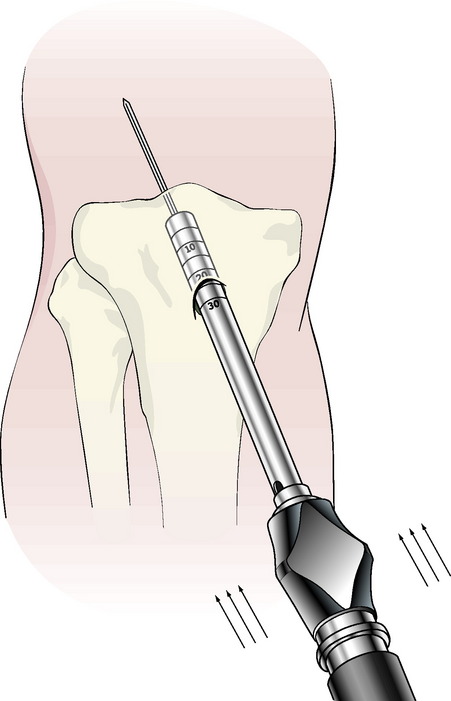
Remove the cortex overlying the distal end of the tibial tunnel. Choose a cannulated reamer that matches the diameter of the soft-tissue ACL graft, and ream over the tibial tunnel guidewire. Slide the calibrated plunger over the tibial guidewire. Impact an 8-mm bone dowel harvester over the plunger and guidewire to the subchondral bone (Fig. 43-3). Rotate the bone dowel harvester several times clockwise and counterclockwise to break off the cylindrical bone. Remove the bone dowel and harvester. If the guidewire is removed with the bone dowel, then insert an 8-mm reamer into the tibial tunnel and rethread the guidewire through the cannulation in the reamer. Finish reaming the tibial tunnel.
Drill the Counter Bore
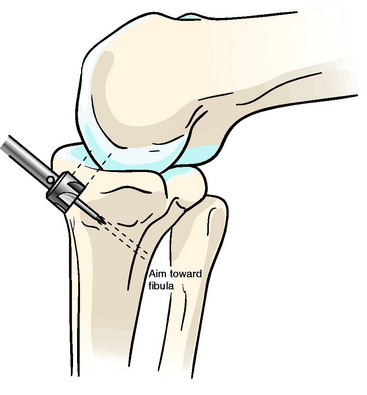
Use electrocautery and a ronguer to remove a small section of the superficial layer of the medial collateral ligament (MCL) that overlies the cortical opening of the tibial tunnel. Insert the counterbore guide into the tibial tunnel until the vertical sleeve abuts against the distal end of the anterior edge of the tibial tunnel. Point the vertical sleeve at the fibula, and impact the awl. Insert the counterbore into the awl hole, and orient the counterbore so that it is parallel to the posterior wall of the tibial tunnel and oblique to the anterior tibial cortex. Remove a small amount of bone from the anterior tibial cortex until the counterbore is flush with the back wall of the tibial tunnel (Fig. 43-4).
Impact the WasherLoc
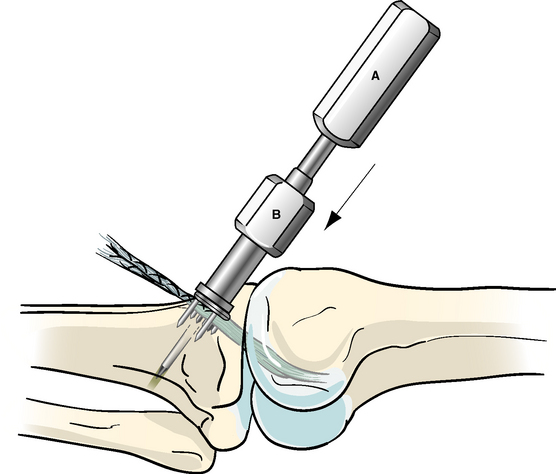
Position the knee in full extension. Thread the awl into the drill sleeve and the drill sleeve into the WasherLoc. Tension the soft-tissue graft. Rotate the flat edge of the WasherLoc distal, place half of the soft-tissue ACL graft on each side of the awl, insert the awl in the hole, and direct the tip of the awl toward the fibula. Impact the WasherLoc into the back wall of the tibial tunnel until it is fully seated (Fig. 43-5).
Dilate the Tibial Tunnel
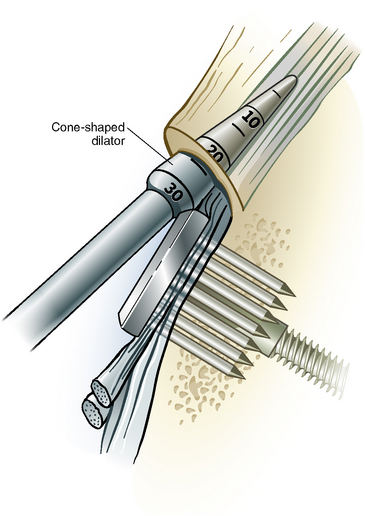
Confirm that stability has been restored to the knee and the tension in the ACL graft is correct. Place the tip of the tapered dilator between the anterior surface of the soft-tissue graft and tibial tunnel (Fig. 43-6). Gently impact the dilator to the level of the joint line, which is typically 25 mm.
Compact the Bone Dowel
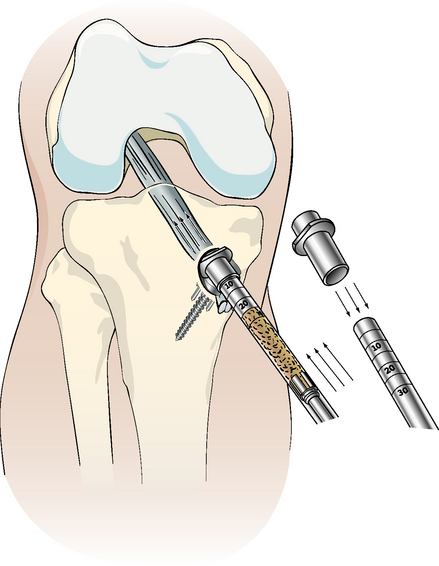
Stuff any loose bone reamings and wallplasty fragments into the tibial tunnel, and compact the bone with a 7 or 8 impingement rod. Place the plastic cover on the sharp tip of the bone dowel harvester, and drive the bone dowel into the tibial tunnel (Fig. 43-7).
Promoting Tendon–Tunnel Healing of a Soft-Tissue Anterior Cruciate Ligament Graft
Healing of a soft-tissue ACL graft14 is a greater concern than that of a BPTB graft because a tendon graft heals slower than a bone plug during the first 6 weeks of implantation.15 Healing is more of a problem in the tibia than in the femur because the marrow is filled with more fat16 and the bone is softer.17 Therefore a soft-tissue graft requires better fixation technique than a BPTB graft,15 especially in the tibia.16 The consequence of not addressing the slow tendon–tunnel healing is slippage during early rehabilitation.18 Slippage is more likely with a soft tissue ACL graft than with a BPTB graft because there is less pain early on.19
Strategies That Promote Tendon–Tunnel Healing
One strategy for promoting tendon–tunnel healing is the use of a long, snug tunnel (Fig. 43-8). The healing of a tendon graft is stronger and stiffer when the tunnel is lengthened and the fit between the tendon and tunnel wall is snug.20 Lengthening the tunnel requires placement of the fixation device at the end of the tunnel and not inside (intratunnel device).12 Compaction of a bone dowel into the tibial tunnel along side a soft-tendon graft increases the snugness of fit by filling gaps between the tendon and tunnel wall.21,22
A second strategy for promoting healing is to allow circumferential and avoid one-sided healing between the tendon and tunnel wall (see Fig. 43-8). The healing of a tendon graft is stronger and stiffer when the tendon heals to the tunnel circumferentially and is not one-sided. Circumferential healing requires placement of the fixation device at the end of the tunnel so that the entire surface area of the tunnel can heal to the graft.12 One-sided healing occurs with intratunnel devices such as the interference screw.23 The interference screw “interferes” and slows tendon–tunnel healing because the screw prevents one side of the tendon from healing to the graft.12
A third strategy is to surround the tendon graft with a biologically active substance. Healing of a tendon is accelerated and stronger when a biologically active substance is inserted in the tunnel with the graft. Wrapping periosteum around the graft accelerates the healing process of a tendon in a bone tunnel and leads to better biomechanical fixation in a shorter period of time.24 Adding bone morphogenetic protein accelerates the healing process when a tendon graft is transplanted into a bone tunnel.25 The acceleration of healing by periosteum and bone morphogenetic protein suggests that compaction of autogenous bone into the tunnel might also benefit healing. Autogenous cancellous bone has viable osteoblasts that may initiate, regulate, and accelerate the ingrowth of bone into the tendon. The use of the WasherLoc at the end of the tibial tunnel with compaction of bone dowel fulfills these criteria for promoting tendon–tunnel healing by providing a long, snug tunnel; circumferential healing; and the addition of a biologically active substance.
WasherLoc Resists Slippage Under Cyclical Load
Several biomechanical studies have shown that the WasherLoc has superior resistance to slippage, higher stiffness, and higher strength than other soft tissue tibial fixations.2,3,4,6–9,11–13 When studies are performed using human bone, the WasherLoc slips less, is stiffer, and stronger than interference screw, double staples, soft tissue washer and screw, and sutures tied to a post.9 Although there has been no head-to-head comparison of the IntraFix versus the WasherLoc in human bone, the IntraFix has been shown to slip more under cyclical load than the interference screw,26 which indicates that the IntraFix slips substantially more than the WasherLoc.
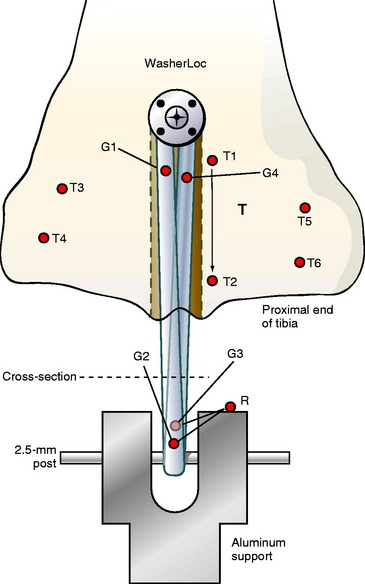
Cyclical testing simulating 6 weeks of normal walking showed that the slippage of a two-strand soft tissue graft fixed with a WasherLoc was less than 0.6 mm, which is clinically imperceptible (Fig. 43-9). The fixation site was loaded 225,000 times from 0N to 170N to simulate the predicted number of steps in 6 weeks of normal walking and the load in the ACL during normal gait.13 The slippage resistance of the WasherLoc is consistent with clinical results that showed excellent anterior stability with use of brace-free, aggressive rehabilitation and early return to sport at 4 to 6 months.1,5
Bone Dowel Limits Tunnel Widening at 1 to 2 Years
Tunnel expansion in ACL reconstruction is greater with a hamstring autograft than with a BPTB autograft27–29 and occurs with a variety of hamstring fixation devices.28–32 The clinical consequences of the common phenomenon of tunnel expansion are being defined; however, tunnel expansion can complicate revision surgery.33,34 Therefore a technique for fixing a hamstring graft to the tibia that limits tunnel expansion to the cross-sectional area of the reamer might have a clinical benefit by simplifying revision surgery.
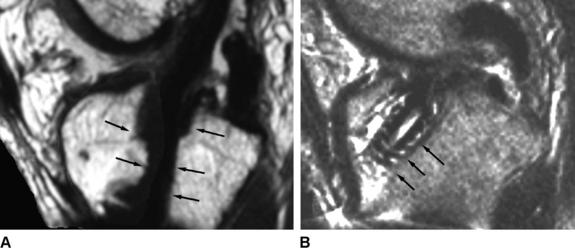
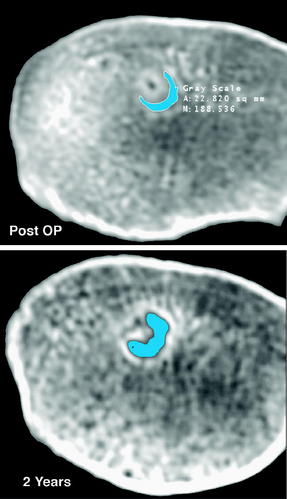
In an in vivo study, a bone dowel averaging 23 mm in length and 7 mm in diameter was harvested from the tibial tunnel in 10 subjects undergoing hamstring ACL reconstruction. The cross-sectional area of the tibial tunnel was calculated on the day of surgery, 4 months, and 1 to 2 years postoperatively from computed tomography scans. The bone dowel reduced the cross-sectional area of the tunnel on the day of surgery and limited tunnel expansion to that of the cross-sectional area of the reamer at 4 months and 1 to 2 years (Fig. 43-10). Ninety percent of the subjects treated with a bone dowel had little to no tunnel expansion at 1 to 2 years. The limitation of tunnel expansion to that of the cross-sectional area of the reamer has not been shown with other tibial fixation techniques. Limiting tunnel expansion to that of the cross-sectional area of the reamer should simplify revision surgery.10
1 Aglietti P, Giron F, Buzzi R, et al. Anterior cruciate ligament reconstruction: bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg. 2004;86A:2143-2155.
2 Bailey SB, Grover DM, Howell SM, et al. Foam-reinforced elderly human tibia approximates young human tibia better than porcine tibia: A study of the structural properties of three soft-tissue fixation devices. Am J Sports Med. 2004;32:755-764.
3 Coleridge SD, Amis AA. A comparison of five tibial-fixation systems in hamstring-graft anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2004;12:391-397.
4 Grover DM, Howell SM, Hull ML. Early tension loss in an anterior cruciate ligament graft. A cadaver study of four tibial fixation devices. J Bone Joint Surg. 2005;87A:381-390.
5 Howell SM, Gittins ME, Gottlieb JE, et al. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001;29:567-574.
6 Howell SM, Roos P, Hull ML. Compaction of a bone dowel in the tibial tunnel improves the fixation stiffness of a soft tissue anterior cruciate ligament graft: an in vitro study in calf tibia. Am J Sports Med. 2005;33:719-725.
7 Kousa P, Jarvinen TL, Vihavainen M, et al. The fixation strength of six hamstring tendon graft fixation devices in anterior cruciate ligament reconstruction. Part II: tibial site. Am J Sports Med. 2003;31:182-188.
8 Kudo T, Tohyama H, Minami A, et al. The effect of cyclic loading on the biomechanical characteristics of the femur-graft-tibia complex after anterior cruciate ligament reconstruction using Bone Mulch screw/WasherLoc fixation. Clin Biomech (Bristol, Avon). 2005;20:414-420.
9 Magen HE, Howell SM, Hull ML. Structural properties of six tibial fixation methods for anterior cruciate ligament soft tissue grafts. Am J Sports Med. 1999;27:35-43.
10 Matsumoto A, Howell SM. Time related changes in the cross-sectional area of the tibial tunnel after compaction of an autograft bone dowel alongside a hamstring graft. Arthroscopy. 2006;22:855-860.
11 Roos PJ, Hull ML, Howell SM. Lengthening of double-looped tendon graft constructs in three regions after cyclic loading: a study using Roentgen stereophotogrammetric analysis. J Orthop Res. 2004;22:839-846.
12 Singhatat W, Lawhorn KW, Howell SM, et al. How four weeks of implantation affect the strength and stiffness of a tendon graft in a bone tunnel: a study of two fixation devices in an extraarticular model in ovine. Am J Sports Med. 2002;30:506-513.
13 Smith CK, Hull ML. Lengthening of a single-loop tibialis tendon graft construct after cyclic loading: a study using roentgen stereophotogrammetric analysis. J Biomech Eng. 2006;128:437-442.
14 Chen CH, Chen WJ, Shih CH, et al. Enveloping the tendon graft with periosteum to enhance tendon-bone healing in a bone tunnel: a biomechanical and histologic study in rabbits. Arthroscopy. 2003;19:290-296.
15 Tomita F, Yasuda K, Mikami S, et al. Comparisons of intraosseous graft healing between the doubled flexor tendon graft and the bone-patellar tendon-bone graft in anterior cruciate ligament reconstruction. Arthroscopy. 2001;17:461-476.
16 Grassman SR, McDonald DB, Thornton GM, et al. Early healing processes of free tendon grafts within bone tunnels is bone-specific: a morphological study in a rabbit model. Knee. 2002;9:21-26.
17 Corry IS, Webb JM, Clingeleffer AJ, et al. Arthroscopic reconstruction of the anterior cruciate ligament: a comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med. 1999;27:444-454.
18 Giurea M, Zorilla P, Amis AA, et al. Comparative pull-out and cyclic-loading strength tests of anchorage of hamstring tendon grafts in anterior cruciate ligament reconstruction. Am J Sports Med. 1999;27:621-625.
19 Feller JA, Webster KE, Gavin B. Early post-operative morbidity following anterior cruciate ligament reconstruction: patellar tendon versus hamstring graft. Knee Surg Sports Traumatol Arthrosc. 2001;9:260-266.
20 Greis PE, Burks RT, Bachus K, et al. The influence of tendon length and fit on the strength of a tendon-bone tunnel complex. A biomechanical and histologic study in the dog. Am J Sports Med. 2001;29:493-497.
21 To JT, Howell SM, Hull ML. Contributions of femoral fixation methods to the stiffness of anterior cruciate ligament replacements at implantation. Arthroscopy. 1999;15:379-387.
22 Wallace MP, Howell SM, Hull ML. In vivo tensile behavior of a four-bundle hamstring graft as a replacement for the anterior cruciate ligament. J Orthop Res. 1997;15:539-545.
23 Weiler A, Hoffmann RF, Bail HJ, et al. Tendon healing in a bone tunnel. Part II: histologic analysis after biodegradable interference fit fixation in a model of anterior cruciate ligament reconstruction in sheep. Arthroscopy. 2002;18:124-135.
24 Kyung HS, Kim SY, Oh CW, et al. Tendon-to-bone tunnel healing in a rabbit model: the effect of periosteum augmentation at the tendon-to-bone interface. Knee Surg Sports Traumatol Arthrosc. 2003;11:9-15.
25 Rodeo SA, Suzuki K, Deng XH, et al. Use of recombinant human bone morphogenetic protein-2 to enhance tendon healing in a bone tunnel. Am J Sports Med. 1999;27:476-488.
26 Caborn DN, Brand JCJr, Nyland J, et al. A biomechanical comparison of initial soft tissue tibial fixation devices: the Intrafix versus a tapered 35-mm bioabsorbable interference screw. Am J Sports Med. 2004;32:956-961.
27 Clatworthy MG, Annear P, Bulow JU, et al. Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc. 1999;7:138-145.
28 L’Insalata JC, Klatt B, Fu FH, et al. Tunnel expansion following anterior cruciate ligament reconstruction: a comparison of hamstring and patellar tendon autografts. Knee Surg Sports Traumatol Arthrosc. 1997;5:234-238.
29 Webster KE, Feller JA, Hameister KA. Bone tunnel enlargement following anterior cruciate ligament reconstruction: a randomized comparison of hamstring and patellar tendon grafts with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2001;9:86-91.
30 Buck DC, Simonian PT, Larson RV, et al. Timeline of tibial tunnel expansion after single-incision hamstring anterior cruciate ligament reconstruction. Arthroscopy. 2004;20:34-36.
31 Buelow JU, Siebold R, Ellermann A. A prospective evaluation of tunnel enlargement in anterior cruciate ligament reconstruction with hamstrings: extracortical versus anatomical fixation. Knee Surg Sports Traumatol Arthrosc. 2002;10:80-85.
32 Simonian PT, Levine RE, Wright TM, et al. Response of hamstring and patellar tendon grafts for anterior cruciate ligament reconstruction during cyclic tensile loading. Am J Knee Surg. 2000;13:8-12.
33 Bach BRJr. Revision anterior cruciate ligament surgery. Arthroscopy. 2003;19:14-29.
34 Fink C, Zapp M, Benedetto KP, et al. Tibial tunnel enlargement following anterior cruciate ligament reconstruction with patellar tendon autograft. Arthroscopy. 2001;17:138-143.






