Walking difficulties and clumsiness
Walking is very important to the way we live. The impact of losing this ability on a patient’s lifestyle can be readily appreciated. It is not surprising that the ability to walk independently is a prominent factor in all the scales of neurological disability.
Walking on two legs is a complicated process. It requires:







History
In taking the history of a patient with walking difficulties, consider particularly:




Gait analysis
On watching a patient walk, the disturbance can be broadly subdivided into symmetrical and asymmetrical gait disturbances (Fig. 1).
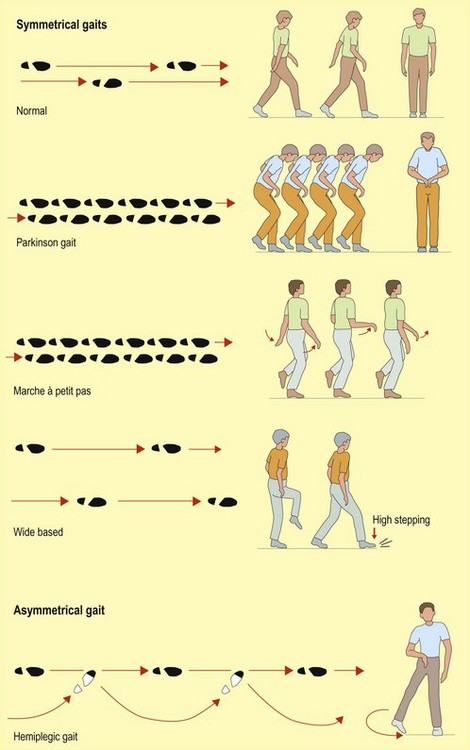
Asymmetrical gait disturbances









Small steps


Abnormal gait patterns



Crossing-over gait – scissoring gait
Patients with bilateral leg spasticity with circumduction from both legs produce a scissoring gait.







Cerebellar syndromes
Clumsiness, incoordination and ataxia are the major symptoms and signs found in cerebellar disease. Cerebellar syndromes occur in different diseases (Box 1). The clinical pattern can be divided into two broad categories: asymmetric syndromes due to focal lesions and symmetrical syndromes due to toxic, metabolic and degenerative causes. The most common causes are multiple sclerosis in younger patients, stroke in older patients and toxins including alcohol and some anticonvulsants. There are a number of rarer degenerative conditions, both inherited, such as the spinocerebellar ataxias (many genes have been identified for these conditions) and sporadic, such as multiple system atrophy. Paraneoplastic cerebellar syndromes can be associated with small cell lung and ovarian cancers, and antineuronal antibodies against the Purkinje cells may be found.











