97 Viral Infections
Epstein-Barr Virus
Clinical Presentation
EBV infection causes a wide spectrum of clinical diseases. In many infants and young children, the symptoms are mild or unrecognized. The symptoms of infectious mononucleosis are malaise, fatigue, prolonged fever, sore throat, headache, nausea, and abdominal pain. Patients often have pharyngitis with exudates, lymphadenopathy, hepatomegaly, or splenomegaly. The incidence of dermatitis may be as high as 15% and is even more pronounced in children who were treated with ampicillin or amoxicillin; it is often called “ampicillin rash” (Figure 97-1). Rare complications of mononucleosis include airway obstruction, central nervous system (CNS) disorders, splenic rupture, thrombocytopenia, and hemolytic anemia.
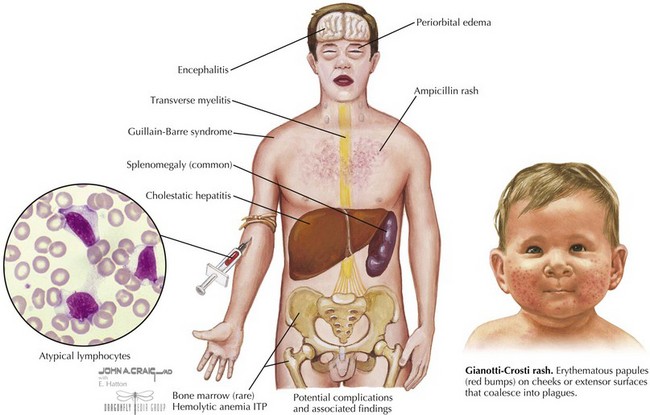
EBV is also associated with Gianotti-Crosti syndrome in which a symmetric rash is seen on the cheeks, extensor surfaces, or buttocks with multiple erythematous papules, which may coalesce into plaques. This may persist for 15 to 50 days and may sometimes look like atopic dermatitis (see Figure 97-1).
Evaluation and Management
In 90% of cases, there is leukocytosis of 10,000 to 20,000 cells/mm3 with a predominance of lymphocytes with 20% to 40% atypical lymphocytes. There may be a mild thrombocytopenia but usually no purpura, and mild elevations of transaminases can occur. A nonspecific test for heterophile antibodies (also called Monospot) can be done. These are immunoglobulin M (IgM) antibodies that agglutinate sheep or horse red blood cells (RBCs) and usually appear during the first 2 weeks of illness and gradually disappear over a 6-month period. This test result is often negative in children younger than 4 years old. EBV can also be detected by serologic antibody testing. In the acute phase, there is a rapid immunoglobulin M (IgM) and IgG response to viral capsid antigen (VCA) and IgG to early antigen(EA). Positive Epstein-Barr virus nuclear antigen (EBNA) (nuclear antigen) antibody indicates past infection because this is not usually present until several weeks to months after infection (Table 97-1).

Measles
Clinical Presentation
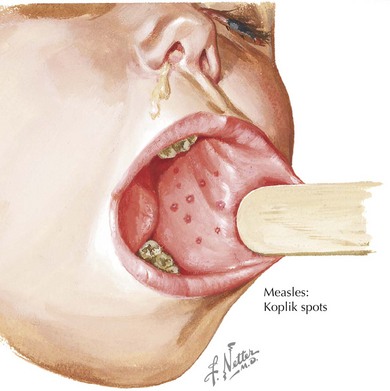
There are four phases to the infection: incubation period, prodrome, exanthem, and recovery. The prodrome period begins with a mild fever that increases to 103° to 105°F, conjunctivitis, coryza, and cough. Koplik spots appear 1 to 4 days before the rash. They appear as red lesions with a bluish white spot in the center and are usually on the inner aspects of the cheek. Rash usually appears after 2 to 4 days and begins on the face as discrete erythematous patches and spreads downward often becoming confluent (Figure 97-2). Lesions are also seen on the palms and soles. Rash fades in about 7 days and may leave desquamation of the skin. Cough can last up to 10 days.
Herpes Simplex Virus
There are 2 types of herpes simplex virus (HSV), type 1 and type 2, that can cause a variety of illnesses depending on the host and the site of infection. A primary herpes infection occurs in those who have never been infected with either HSV-1 or HSV-2. A nonprimary first infection occurs when an individual who was previously infected with one type of HSV then becomes infected with another type. A recurrent infection is a reactivation of the virus from the latent state. HSV can also cause severe neonatal infection (see Chapter 105).
Etiology and Pathogenesis
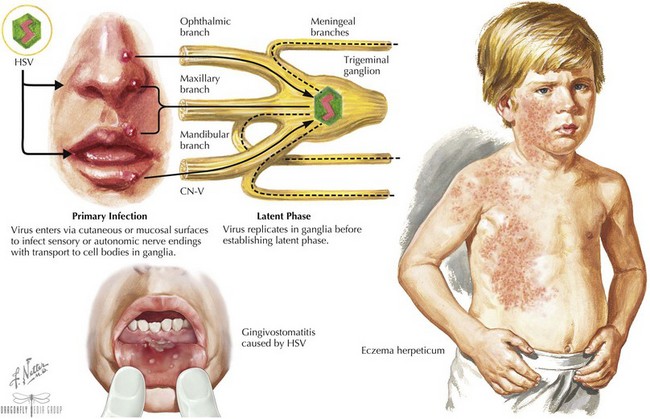
The virus enters through mucosal surfaces and then spreads via nerve endings to sensory ganglia. Some viruses then establish latency in these sensory neurons (Figure 97-3). The incubation period is usually 2 days to 2 weeks.
Clinical Presentation
The most common clinical manifestation of primary infection in children is gingivostomatitis and is usually caused by HSV-1. It causes sudden onset of pain in the mouth often manifested as refusal to eat, drooling, and high fevers. The gums become very swollen, and vesicles that are usually grouped on an erythematous base are seen throughout the oral cavity, including the gums, lips, tongue, palate, tonsils, and pharynx. The vesicles can progress to ulcers, and lymphadenopathy is often seen (see Figure 97-3). The illness usually resolves in 7 to 14 days.
HSV infections can occur on any skin surface that may have breakdown or trauma. Herpetic whitlow is a term used for HSV infections of the fingers or toes. Lesions and pain usually last for 10 days, and complete recovery usually occurs in 18 to 20 days. Eczema herpeticum is described in patients with a history of eczema who are superinfected with HSV (see Figure 97-3). In addition to severe rash, patients can present with high fevers, malaise, and lymphadenopathy. Other areas of the body that may be affected by HSV include the conjunctiva, cornea, and retina as well as the CNS, causing encephalitis and aseptic meningitis. Thus, any vesicles around the eyes should prompt an ophthalmologic examination. HSV has also been implicated in erythema multiforme and Bell’s palsy.
Varicella Zoster Virus
Clinical Presentation
Chicken pox is characterized by fever, malaise, anorexia, headache, and a classic rash that starts centrally and then spreads outward. The rash begins as erythematous macules that then become very pruritic and vesicular. It is often described as a “dew drop on a rose petal” (Figure 97-4). Crusting of the lesions then occurs as new ones arise, resulting in different stages of rash. A child who has been previously vaccinated but infected with VZV may have “breakthrough varicella” in which the rash is more atypical. The rash may be maculopapular and less vesicular with fewer lesions. Severe neonatal chicken pox can develop if a mother develops the disease 5 days before delivery or 2 days after.
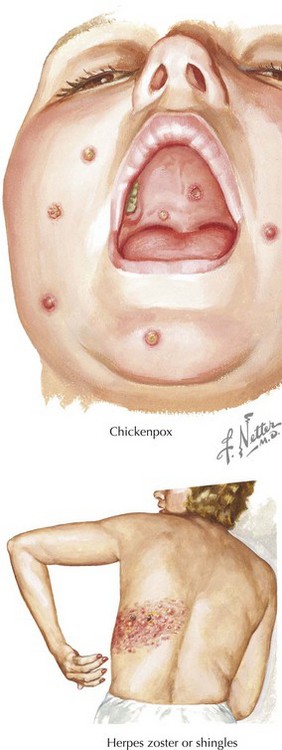
Complications of varicella include bacterial superinfections of the skin, thrombocytopenia, arthritis, hepatitis, cerebellar ataxia, encephalitis, meningitis, and glomerulonephritis. These complications are more common in adolescents, adults, infants, and immunocompromised patients. The reactivation of latent VZV causes zoster or shingles and manifests as grouped vesicles within one or two dermatomes (see Figure 97-4). Although the lesions can cause intense pain in adults, children commonly have a mild rash with minimal symptoms that usually resolve in 1 to 2 weeks.
Human Herpesvirus 6
Clinical Presentation
Roseola is characterized by high fever (usually >103°F) that may persist for 3 to 7 days. During this time some infants may be irritable and anorexic, usually without upper respiratory tract infections. Febrile seizure can occur in 10% to 15% of patients. A rose-colored maculopapular rash usually develops on the trunk during defervescence, spreads to the extremities and face, and then fades after 1 to 3 days (Figure 97-5). HHV-6 can also cause nonspecific febrile illnesses without rash accompanied by cervical or post-occipital lymphadenopathy, respiratory or gastrointestinal (GI) symptoms and inflamed tympanic membranes. It is also thought that HHV-6 reactivation may contribute to disease in the immunocompromised host.

Parvovirus B19
Enterovirus (Nonpoliovirus)
Clinical Presentation
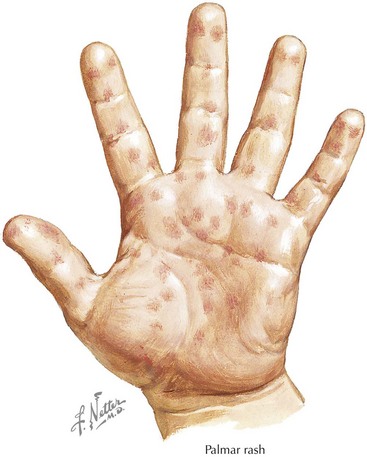
A common manifestation in children is hand, foot, and mouth disease in which children usually have fever, oropharyngeal inflammation, and vesicles with an erythematous ring in the oral cavity usually on the tongue, buccal mucosa, and posterior soft palate. The vesicles can ulcerate and cause anorexia. Often there is also a maculopapular, vesicular, or pustular lesion on the palms, soles, hands, feet, and occasionally buttock and groin (Figure 97-6).
Candy B, Hotopf M: Steroids for symptom control in infectious mononucleosis. Cochrane Database Syst Rev 3:CD004402, 2006.
Caldararo S. Measles. Pediatr Rev. 2007;28:352-354.
Gerber JS, Offit PA. Vaccines and autism: a tale of shifting hypotheses. Clin Infect Dis. 2009;48:456-461.
Papania MJ, Seward JF, Redd SB, et al. Epidemiology of measles in the United States, 1997-2001. J Infect Dis. 2004;189(Suppl):S61-S68.
Perry RT, Halsey NA. The clinical significance of measles: a review. J Infect Dis. 2004;189(Suppl 1):S4-S16.
Chayavichitsilp P, Buckwalter JV, Krakowski AC, Friedlander SF. Herpes simplex. Pediatr Rev. 2009;30:110-130.
Elbers JM, Bitnun A, Richardson SE, et al. A 12 year prospective study of childhood herpes simplex encephalitis: is there a broader spectrum of disease? Pediatrics. 2007;119:e399-e407.
Nasser M, Fedorowicz Z, Khoshnevisan MH, et al: Acyclovir for treating primary herpetic gingivostomatitis. Cochrane Database Syst Rev 4: CD006700, 2008.
Gershon AA. Varicella zoster virus infections. Pediatr Rev. 2008;29:5-11.
Macartney D, McIntyre P: Vaccines for post-exposure prophylaxis against varicella in children and adults. Cochrane Database System Rev 3:CD001833, 2008.
Nguyen HQ, Jumaan AO, Seward JF: Decline in mortality due to varicella after implementation of varicella vaccination in the United States. N Engl J Med 352:450-458, CD001833.
Araujo TD, Berman B. Human herpesviruses 6 and 7. Dermatol Clin. 2000;20:301-306.
Caserta MT, Mock DJ, Dewhurst S. Human herpesvirus 6. Clin Infect Dis. 2001;33:829-833.
Campadelli-Fiume G, Mirandola P. Human herpesvirus 6: an emerging pathogen. Emerg Infect Dis. 1999;5:353-366.
Koch WC. Fifth (human parvovirus) and sixth (herpesvirus 6) diseases. Curr Opin Infect Dis. 2001;14:343-356.
Katta R. Parvovirus B19: a review. Dermatol Clin. 2002;20:333-342.
Koch WC. Fifth (human parvovirus) and sixth (herpesvirus 6) diseases. Curr Opin Infect Dis. 2001;14:343-356.
Smith-Whitley K, Zhao H, Hodinka RL, et al. Epidemiology of human parvovirus B19 in children with sickle cell disease. Blood. 2004;103:422-427.






